Introduction
The symbiosis of the electronic and communication era and the information technology has broadened the scope of knowledge of the profession. Cephalometry has gained prominence as the diagnostic / treatment planning tool not only of the Orthodontist but also by maxillofacial and plastic surgeons. Quantification thus provides a reliable communication tools as day by day interactions between various specialities increases. Cephalometric analysis can be employed to describe, compare, classify and to communicate the nature of Orthodontic and Orthopedic problems.
An accurate anteroposterior measurement of jaw relationships is critically important in orthodontic diagnosis and treatment planning. The angular and linear measurements that have been proposed can be inaccurate because of their dependency on various factors[1]. Science of Cephalometrics is a dynamic study, there’s always space for developing new techniques and new ways. The beginning of Cephalometrics might best be ascribed to J.A.W. Van Loon of Utrecht, Holland. He described a technique concerned with relating the teeth to the rest of the face[2]. Such methods showed the true picture of the stereoscopic significance of the patient’s malocclusion.
Generally used parameters for antero-posterior assessment of jaw relationships are
ANB angle and Wits appraisal.[3] Several authors give some shortcoming of ANB angle[4],[5],[6],[7],[8] and Wits appraisal.[9] Because of the limitation and drawbacks a new measurement BETA angle[10] was developed by Chong Yol Baik and Maria Verveidou(2004) at Tufts University. The Beta angle is a new measurement for assessing the skeletal discrepancy between the maxilla and the mandible in the sagittal plane.
It uses 3 skeletal landmark— point A, point B, and the apparent axis of the condyle (C)—to measure an angle that indicates the severity and the type of skeletal dysplasia in the sagittal dimension.
The Beta angle can be found by, first, locating 3 points:
A point (subspinale)—the deepest midline point on the premaxillae between the ANS and prosthion (described by Downs[11]).
B point (supramentale)—the most posterior point in the concavity between infradentale and pogonion (described by Downs).
The center of the condyle, found by tracing the head of the condyle and approximating its center ( C ).
Next, defining 3 lines:
1. Line connecting the center of the condyle C with B point (C-B line).
2. Line connecting A and B points.
3. Line from point A perpendicular to the C-B line.
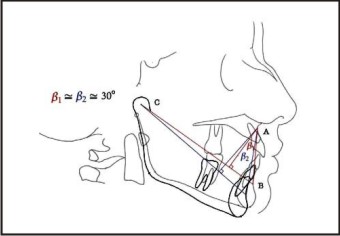
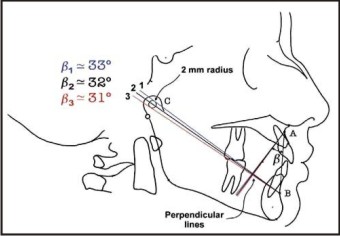
Angle is constructed by the line connecting the center of condyle C with point B, Line connecting the points A and B and Line from point A perpendicular to the line C-B. Angle between the perpendicular line and the A-B line, is known as BETA ANGLE[10].(Fig 1)
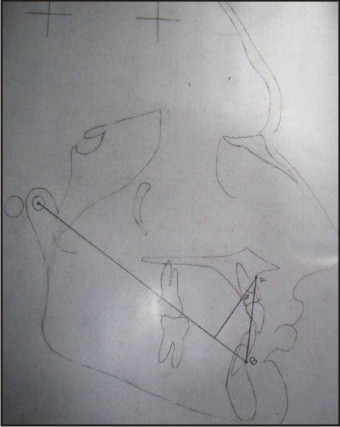 | Fig 1: Measurement Of Beta Angle
 |
Material And Methods
This study was conducted in the Department of Orthodontics and Dentofacial Orthopedics, MM College of Dental Sciences & Research. MM University, Mullana, Haryana, India.
The sample comprising of 150 cephalogram was selected from available patient’s records at Department.All patients selected were between the ages of 9 and 15 years, and had never undergone orthodontic treatment.
The sample was divided into three groups comprising of 50 cephalogram each based on ANB angle, Wits appraisal and profile. (Table I) (Graph I)
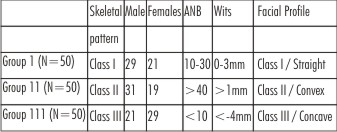 | Table I : Demographics Of The Study.
|
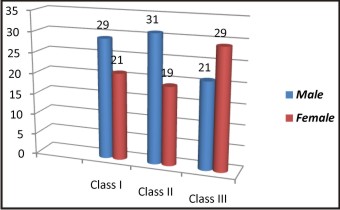 | Graph 1: Gender Based Division Of The Subjects
|
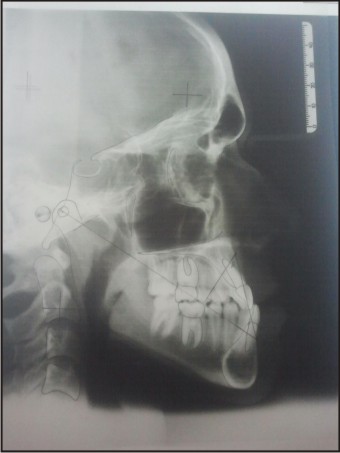
Group 1- comprising of 50 cephalogram with class I Skeletal pattern. Where in ANB angle was 10 - 30, Wits appraisal was 0 to 3mm and pleasant facial profile.(Fig 2)
 | Fig 2: Beta Angle Traced For Group I.
|
Group 2 - comprising of 50 cephalogram with class II Skeletal pattern. Where in ANB angle was more than 40, Wits appraisal was more than 1 mm and convex or class II facial profile.
Group 3 - comprising of 50 cephalogram with class III Skeletal pattern. Where in ANB angle was Less than or equal to 10, Wits appraisal was less than or equal to -4mm and concave or class III facial profile.(Fig 3).
 | Fig 3: Beta Angle Traced For Group III
|
Beta angle was hand traced and measured for each Group each sample. Three readings were made and their mean taken as final reading. All the Recorded data was then subjected to statistical analysis.(Table II)
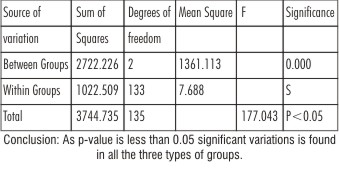 | Table II : One way ANOVA
|
Statistical Analysis & Results
Thus beta angle was between 26° and 37.5° for skeletal class I pattern, < 26° for skeletal class II pattern and >37.5° for skeletal class III pattern. (Table III) (Graph II).
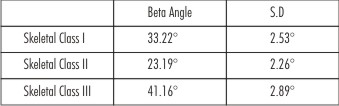 | Table III : Beta angle & Standard Deviation
|
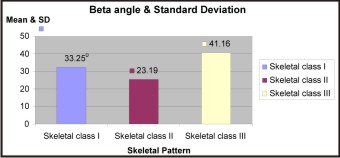 | Graph II: Beta Angle & Standard Deviation
|
Discussion
Moyers et al.[12] in their article clearly stated that any cephalometric analysis based on either angular or linear measurements has obvious shortcomings. Till now the most popularly used parameter for assessing the sagittal jaw relationship is ANB angle.It has been demonstrated in the literature[1],[3],[4],[5],[6],[7],[8],[13] that there is often a difference between the interpretation of this angle and the actual discrepancy between the apical bases. Several authors[4],[14],[15],[16] have shown that the position of nasion is not fixed during growth, and any displacement of nasion will directly affect the ANB angle.[17] Furthermore, rotation of the jaws by either growth or orthodontic treatment can also change the ANB reading.[1] Studies[3],[4],[5],[6],[7],[8] have pointed that the ANB angle had several shortcoming as the position of Nasion is not fixed during growth, and any displacement of Nasion will directly affect the ANB angle[7]. To overcome these shortcomings an alternative was proposed i.e. the Wits appraisal.[1] It does not depend on cranial landmarks but still has the problem of correctly identifying the functional occlusal plane, which can sometimes be nearly impossible. Accurate identification of occlusal plane is not always easy or reproducible[13], especially in mixed dentition patients or patients with open bite, multiple impactions, missing teeth, skeletal asymmetries, or deep curve of spee. Any change in the angulation of the functional occlusion plane, caused either by normal development of dentition or orthodontic intervention, can profoundly influence the wits appraisal.[14]
To overcome these problems a new measurement BETA angle was developed by Chong Yol Baik and Maria Verveidou[10] (2004) at Tufts University for Greece population. They have shown that the Beta angle remains relatively stable when jaws are rotated.(Fig 4) Moreover if there is discrepancy in locating the point that falls in circle between lines 1 and 3, beta angle is affected by less than 1° (Fig 5) which has negligible effect . Their study for Greek population established that for skeletal Class I pattern Beta angle was between 27°-35° and less than 27° is for skeletal class II pattern, Whereas more than 35° is for skeletal class III pattern.
According to Coon[18], Greeks belong to the Caucasian race and are a blend of "racial" subtypes, the most important of which are the Atlanto-Mediterranean and the Alpine.
Their norms are apt for Caucasian population and as we know there is distinct difference between Indian population as they bear close reference to Afro-Asian race so the Caucasian norms may not correctly applicable for Indian population. This study established norms the norms for beta angle for the North Indian population and the results in this study showed beta angle between 26°and 37.5°in skeletal class I pattern, less than 26° in skeletal class II pattern whereas more than 37.5° in skeletal class III pattern.
 | Fig 4: Affect Of Jaw Opening On Beta Angle.
|
 | Fig 5: Affect Of Location Of Point C On Beta Angle.
|
Conclusion
Beta angle between 26° and 37.5° have skeletal class I pattern; Beta angle less than 26° indicates a class II skeletal pattern and a Beta angle more than 37.5° indicates a class III skeletal pattern for North Indian population. (Table III) (Graph II).
Clinicians should in addition use Beta angle as the Beta angle enriches the current cephalometric tools available to the clinicians and enables better diagnosis and treatment planning for patients.
References:
1. Jacobson A. The ‘Wits’ appraisal of jaw disharmony .Am J Orthod 1975;67:125-38
2. www.ncbi.nlm.nih.gov/pubmed/12073908
3. Jacobson A. The application of ‘Wits’ appraisal. Am J Orthod 1976;70:179-89
4. Freeman RS. Adjusting A-N-B angles to reflect the effect of maxillary position. Angle Orthod 1981;51:162-71.
5. Hussels W, Nanda RS. Analysis of factors affecting angle ANB. Angle J Orthod 1984;85:411- 23
6. Holdaway RA. Changes in relationship of points A and B during orthodontic treatment. Am J Orthod 1956;42:176-93
7. Taylor CM. Changes in relationship of nasion, point A and point B, and the effect upon ANB. Am J Orthod 1969; 56:143-63.
8. Jarvinen S. A analysis of the variation of the ANB angle :a statistical appraisal. Am J Orthod 1985; 87:144-6.
9. Haynes S, Chau M. The reproducibility and repeatability of the Wits analysis. Am J Orthod Dentofacial Orthop 1995;107: 640-7
10. Chong Yol Baik and Maria Ververidou. A new approach of assessing sagittal discrepancies: The Beta Angle. Am J Orthod Dentofacial Orthop 2004;126:100-5
11. Downs WB. Variations in facial relationships: their significance in treatment and prognosis. Am J Orthod 1948;34:812-40.
12. Moyers RE, Bookstein FL, Guire KE. The concept of pattern in craniofacial growth. Am J Orthod 1979;76:136-48.
13. Beatty EJ. A modified technique for evaluating apical base relationships. Am J Orthod 1975;68:303-15.
14. MooreAW. Observations on facial growth and its clinical significance. Am J Orthod 1959;45:399-423.
15. Nanda RS. The rates of growth of several facial components measured from serial cephalometric roentgenograms. Am J Orthod 1955; 41: 658-73.
16. Enlow DH. A morphogenetic analysis of facial growth. Am J Orthod 1966;52:283-99.
17. Binder RE. The geometry of cephalometrics. J Clin Orthod 1979;13:258-63.
18. Coon CS. The races of Europe. New York: Macmillan, 1948
|