Introduction
The introduction of the acid etch technique in 1955 by Buonocore[1] has made enamel bonding possible in all disciplines of dentistry. One of them is the bonding of orthodontic brackets, either direct or indirect.
One of the most dramatic changes in the orthodontic specialty in the 1970s was the use of composite resin as a bonding material.[2]
The chemically cured resins were the first systems developed for bracket bonding followed by ultraviolet light-cured materials.[3],[4] Due to safety problems[5] and limited depth of cure,[6],[7] ultraviolet light curing has been replaced by visible light curing. Blue light generated by conventional halogen light-curing unit has been the most popular method of polymerizing orthodontic adhesives despite its shortcomings like degradation of lamp, filter, reflector, reduced light intensity, broad spectrum of light, and prolonged curing time which can be uncomfortable to patient.[8],[9] In 1995, LED (light-emitting diode) was proposed as an alternative to the halogen curing light.[10]
One of the main objectives of the research of bonding procedures is to seek ways of reducing chair side time. Adhesive precoated brackets (APCs) (introduced in 1991) have improved the quality and accuracy of orthodontic bondingby reducing the steps in bonding procedures, owing to the consistent quality and quantity of adhesive used, better asepsis, less wastage, easy flash removal and a better control of inventory.[9],[11],[12] Various studies comparing the bond strengths of APC brackets and conventional uncoated brackets have yielded contradictory results.[13],[14][15][16][17]
Success of a bond can be ascertained by a number of ways including measurement of bond strength in vitro, measurement of the failed proportion of brackets in vivo, and ex vivo studies utilizing finite-element analysis. Amongst these, in vitro shear bond strength recording is the easiest method. It has been stated that successful clinical bonding can be achieved with bond strengths from 6-8 MPa and above.[18] Adhesive remnant index[19] and modified adhesive remnant index[20] can be used to determine the nature of bond failure and determine the site of fracture when a bracket debonds.
Several studies have evaluated the clinical efficacy of LED light for bonding orthodontic brackets. They have been unable to demonstrate a significant difference between the bond strength obtained with an LED light curing and a halogen light curing device. Effect of curing at different polymerization times has also been evaluated and bonding brackets with LED at shorter exposure time seems to be a good alternative but further studies are still necessary if its use is to be recommended in orthodontic practice.
 | Fig 1: Halogen Light Curing Unit (3m Espe, Elipar, 2500)
 |
 | Fig 2: LED Curing Uni (3m Espe, Elipar, S10)
|
 | Fig 3: Instron Universal Testing Machine
|
 | Fig 4: Force Application Parallel To The Labial Surface Of The Tooth
|
 | Fig 5: Debonded Bracket From The Labial Surface Of The Tooth
|
Therefore this study was undertaken to compare the shear bond strength of adhesive precoated and uncoated brackets cured using two different curing units: a conventional halogen light and a light-emitting diode, to evaluate the effect of different exposure times and different exposure methods (single exposure and exposure from two sides mesial and distal) on shear bond strength of adhesive precoated brackets cured using light-emitting diode and the amount of remnant adhesive on tooth surface after debonding.
Materials And Methods
This in vitro study was carried out on 140 human premolar teeth without caries or filling that had been extracted for therapeutic purpose in patients undergoing orthodontic treatment in the Department of Orthodontics, M.R. Ambedkar Dental College, Bangalore.
One hundred adhesive precoated and forty conventional uncoated metal brackets (Gemini series, 3M Unitek) were used for bonding. The adhesive used was Transbondxt (3M Unitek) with conventional primer.
Polymerization sources used were halogen light curing unit (3M ESPE, ELIPAR, 2500) and LED light-emitting diode curing unit (3M ESPE, ELIPAR, S10).
Method Of Collection Of Data
140 premolar teeth were randomly divided into seven groups of twenty each. Brackets were divided into two groups. Group I included 40 conventional uncoated metal brackets and had two subgroups. Group II included 100 adhesive precoated brackets and had 5 subgroups.
Bonding:
Group I
20 conventional uncoated brackets were bonded with Transbond XT adhesive in each subgroup.
I a: curing was done using halogen curing unit for 40 seconds, 20 seconds each interproximal side.
I b: curing was done using LED curing unit for 20 seconds, 10 seconds each interproximal side.
Group II
20 adhesive precoated brackets were bonded in each subgroup.
II a: cured using halogen curing unit for 40 seconds, 20 seconds each interproximal side.
II b. curedusing LED curing unit for 20 seconds,10 seconds each interproximal side.
II c: cured using LED curing unit for 20 secondswith single exposure on buccal surface.
II d: cured using LED curing unit for 15 seconds with single exposure on buccal surface.
II e: cured using LED curing unit for 10 secondswith single exposure on buccal surface.
Preparation Of Bonded Tooth For Shear Bond Strength Test:
Acrylic blocks were used to mount the teeth and were stored in distilled water at room temperature before subjecting to shear bond strength test.
Testing Of Shear Bond Strength:
The shear bond strength test was conducted in the laboratory at Composite Technology Park Kengari using an universal testing machine (Instron 4301, Canton, Mass). A load side density of 0-50 Kgs was set in the Instron Machine and the cross head speed was adjusted for 5mm per minute. The load at which the bracket debonded was recorded in Newtons and subsequently calculated in Mega Pascals.
Following the debonding, the residual adhesive remaining on the teeth was assessed by magnifying lens of magnification power 5X using the modified Adhesive Remnant Index (ARI).
Statistical Analysis:
For statistical evaluation of experimental data the mean and standard deviation were calculated for each group. Post-Hoc Tukey test was employed to find the pair wise significance between the groups.Weibull analysis was done to evaluate probability of failure of premolar metal brackets. The chi-square test was usedto determine significant differences in the adhesive remnant index (ARI) scores between the different groups.
Results
Comparison of mean shear bond strength among all groups showed highest shear bond strength for group II b. Group II e recorded lowest mean shear bond strength among all groups. (Table I)
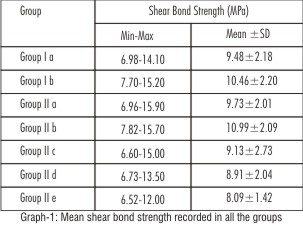 | Table 1: Comparison of Mean Shear bond strength (MPa) in groups of samples studied
|
In order to find out significant difference among pair of groups, Mann-Whitney test was carried out in which shear bond strength recorded in all groups was found to be statistically insignificant (Table II,III,IV,VI ) except among group II b and group II e (Table V).
 | Table II: Pair-wise comparison of shear bond strength (MPa) for group I a
|
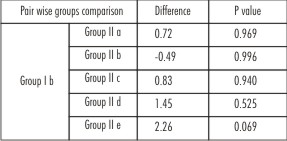 | Table III: Pair-wise comparison of shear bond strength (MPa) for group I b
|
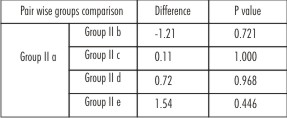 | Table IV: Pair-wise comparison of shear bond strength (MPa) for group II a
|
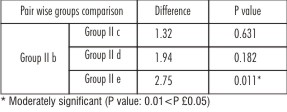 | Table V: Pair-wise comparison of shear bond strength (MPa) for group II b
|
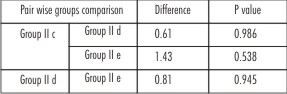 | Table VI: Pair-wise comparison of shear bond strength (MPa) for group II c and II d
|
Analysis Of Ari Scores:
Chi-square test was used to find out if there was any significant association between the ARI scores in different groups. (Table VII)
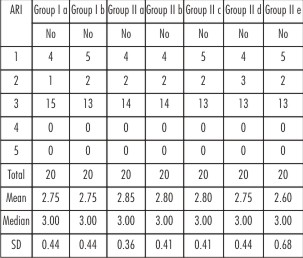 | Table VII: Comparison of ARI score in samples studied
|
c2=1.966; P=0.923
No statistically significant association was found between the ARI scores in all the groups (P>0.05).
Weibull analysis done to evaluate probability of failure of premolar metal brackets showed maximum probability failure of 40% with group II e. Group II b and group I showed minimum failure probability of 5% calculated at clinically acceptable shear bond strength of 8MPa. (Table VIII)
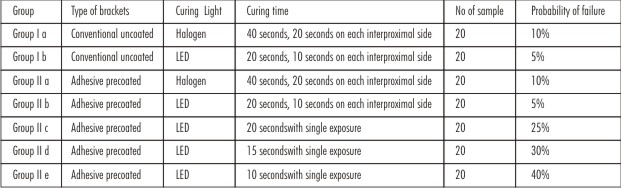 | Table VIII: Probability of failure premolar metal brackets tested at clinically accepted shear bond strength of 8 MPa
|
Discussion
Bonding of orthodontic brackets has become a routine orthodontic procedure in fixed appliance therapy. Maximum conversion of monomer to polymer is necessary to achieve optimal physical properties of adhesive cements and depends on the composite composition, the light source, and the exposure time. It has been suggested that bond strength values between 5.9 MPa and 7.8 MPa are sufficient for a clinically effective orthodontic bonding.[18]
In the present study comparing shear bond strength of conventional uncoated and adhesive precoated brackets showed statistically insignificant difference irrespective of type of curing light used for polymerization.These findings are in agreement with most other previous studieswhich showed no significant difference in bond strength between the brackets.[13][14][15] However these findings are not in concordance with previous studieswhich concluded that precoated brackets had significantly lower shear bond strength than the uncoated brackets bonded with Transbond XT.[16],[17] It was suggested that increased viscosity of adhesive used on APC brackets combined with mesh retention mechanisms incorporated in metal bracket bases seemed to lower shear bond strength.Another study showed higher shear bond strength and less bond failure rate for adhesive precoated brackets.[21]
Results from this study concluded that shear bond strength was not dependent on type of brackets used. There are many light cured adhesives available in the market, differing in the amount of filler particles and viscosity including dual cured composites and glass ionomer cements. All, however, are subject to bond failure because of bracket base contamination and inconsistent amounts of adhesive applied to the bracket. Adhesive precoated brackets have indisputable clinical advantagesowing to the consistent quality and quantity of adhesive used, better asepsis, less wastage, easy flash removal and a better control of inventory.[9],[11],[12]
Taking in view some advantages and differences among halogen light and light emitting diode curing unit, the present in vitro study compared the shear bond strength of brackets polymerized with two different light sources, halogen (3M ESPE, ELIPAR, 2500) and LED (3M ESPE, ELIPAR, S10). Results showed statistically insignificant difference in shear bond strength values between the groups regardless of type of curing light used for polymerization which is in agreement with the results of a previous investigation in which shear bond strength of brackets cured using new intensive LED curing units (OrtholuxTM LED, 3M Unitek; UltraLume LED 5, Ultradent Products, Utah) were compared with halogen curing lamp (OptiluxTM 501).[22],[23] Another study also showed no significant differencesin total bond failure rate between brackets cured with a LED lamp (Ortholux LED, 3M Unitek) and thosecured with a halogen lamp (Ortholux XT, 3M Unitek).[24]
In the present study LED curing units reduced the time necessary to bond orthodontic brackets which was half of that used for halogen. The difference in shear bond strength values was not significant among groups whether halogen or LED curing light was used for polymerization. So LED curing light can be used for polymerization of orthodontic adhesive because it has advantages such as a short time to reach material polymerization, longer lifetime of over 10,000 hours, no filters to produce blue light, resistant to shock and vibration, and use minimal power to operate, stable, efficient, long-lasting output of blue light with little amount of wasted energy and minimum heat generation.[25],[26] It may be speculated that this difference is due to the fact that LED emission spectrum is close to the maximum absorption peak of camphoroquinone which is a photoinitiator used in light cured adhesives and are more efficient in delivering usable light to activate the camphoroquinone.[25]
In the present study, curing using LED unit was done at different exposure times and using different exposure methods. Results showed statistically insignificant difference in shear bond strength values for groups II b, II c and II d so polymerization using LED curing unit for 20 and 15 seconds with single exposure may also be used instead of the traditional 20 seconds, 10 seconds on each interproximal side. Group II e showed significantly low values so single exposure for 10 seconds can be considered insufficient for adequate polymerization of adhesive and for a stronger bond which is in accordance with a study which concluded 10 seconds of LED (Elipar FreeLight, 3M ESPE, Seefeld, Germany) curing resulted in significantly decreased shear bond strength values.[27] These findings are not in concordance with previous studies which showed that the high intensity LED curing devices (Elipar FreeLight 2, 3M ESPE; OrtholuxTM LED, 3M Unitek; UltraLume LED 5; Ultradent Products, South Jordan, Utah ; Bluephase G2,) reduced the exposure time required to efficiently bond orthodontic attachments to only 10 seconds.[28],[29]
The mean shear bond strengthvalues in all groups wereall beyond the range of 5.9 – 7.8 MPa which is clinically acceptable for effective orthodontic bonding. Weibull survival analysis was done to predict the number of bonds likely to fail at a clinically acceptable strength of 8MPa.
Although groups II c, II d and II e showed shear bond strength values beyond the range clinically acceptable for effective orthodontic bonding, Weibull analysis showed high probability of failure of 25%, 30% and 40 % respectively in these groups. This suggests that LED with single exposure for 20, 15 and 10 seconds may be inadequate for orthodontic bonding as there are increased chances of failure of bonds.
The analysis of ARI indicated that most of the adhesive remained adhered to the tooth surface after debonding and was independent of type of brackets and light-curing unit used. This was in accordance with previous studies which also showed cohesive type of bond failure with most adhesive remaining on enamel surface.[17],[30],[31]
Analyzing bracket debonding, it is desirable that the failure occurs between the bracket and the adhesive or at the adhesive interface. Failure between adhesive and enamel can create enamel fractures or cause irregularities. On the other hand, there was greater difficulty in removing excessive adhesive, which is consistent with the findings of a previous study.[25]
Thus LED can be used for bonding orthodontic brackets. An exposure time of 20 seconds, 10 seconds on each interproximal surface would seem to be optimal. However it should be kept in mind that laboratory studies are a valuable screening tool, but clinical studies are needed to validate the preliminary in vitro performance of brackets bonded with the LEDs in vivo.
Conclusions
This study concluded that:
LED with a shorter curing time which is half of that used for halogen provides clinically acceptable bond strength with minimal chances of bond failures.
LED with single exposure for 20, 15, and 10 seconds may be inadequate for orthodontic bonding as there is increased chances of failure of bonds.
Shear bond strength is not dependent on type of brackets used whether adhesive precoated or conventional uncoated brackets.
In all groups most of the adhesive remained on the tooth surface after the debonding of the brackets which is desirable as failure between adhesive and enamel can create enamel fractures or cause irregularities.
References
1. Buonocore MG. A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res 1955;34:849-53.
2. Newman GV. Epoxy adhesives for orthodontic attachments. Am J Orthod 1965;51:901-3.
3. Johnson WT, Hembree JH, Weber FN. Shear strength of orthodontic direct-bonding adhesion. Am J Orthod 1976;70:559-66.
4. Keizer S, Ten Cate JM, Arends J. Direct bonding of orthodontic brackets. Am J Orthod 1976;69:318-27.
5. Burdsell DC, Bannon PJ, Webb PB. Harmful effects of near ultra violet radiation used for polymerization of a sealant and a composite resin. J Am Dent Assoc1976;92:775-8.
6. Lee HL, Orlowski JA, Rogers BJ. A comparison of ultraviolet curing and self curing polymers in preventive, restorative and orthodontic dentistry. Int Dent J 1976;26:134-40.
7. Newman SM, Murray GA, Yates JL. Visible lights and visible light-activated composite resins. J Prosthet Dent 1983;50:31-5.
8. Yoon TH, Lee YK, Lim BS, Kim CW. Degree of polymerization of resin composites by different light sources. J Oral Rehabil 2002;29:1165–73.
9. Sfondrini MF, Cacciafesta V, Scribante A, Klersy C. Plasma arc versus halogen light curing of orthodontic brackets: a 12-month clinical study of bond failures. Am J Orthod Dentofacial Orthop 2004;125:342-7.
10. Mills RW. Blue light emitting diode- an alternative method of light curing ? Br Dent J 1995;178:169.
11. Cooper RB, Goss M, Hamula W. Direct bonding with light-cured adhesive precoated brackets. J Clin Orthod 1992;26:477-9.
12. Ash S, Hay N. Adhesive pre-coated brackets, a comparative clinical study. Br J Orthod 1999;23:325–29.
13. Bearn DR, Aird JC, McCabe JF. Ex-vivo bond strength of adhesive precoated metallic and ceramic brackets. Br J Orthod 1995;22:233-6.
14. Bishara SE, Ajlouni R, Laffoon J. Effects of modifying the adhesive composition on the bond strength of orthodontic brackets. Angle Orthod 2002;72:464-7.
15. Kula K, Schreiner R, Brown J, Glaros A. Clinical bond failure of pre-coated and operator coated orthodontic brackets. Orthod Craniofacial Res 2002;5:161–65.
16. Bishara SE, Olsen M, Von Wald L. Comparisons of shear bond strength of precoated and uncoated brackets. Am J Orthod Dentofacial Orthop 1997;112:617-21.
17. Sfondrini MF, Cacciafesta V, Klersy C. Halogen versus high intensity light-curing of uncoated and pre-coated brackets: a shear bond strength study. J Orthod 2002;29:45-50.
18. Reyonlds IR. A review of direct orthodontic bonding. Br J Orthod 1975;2:171-78.
19. Artun J, Bergland S. Clinical trials with crystal growth conditioning as an alternative to acid etch enamel pretreatment. Am J Orthod 1984;85:333-40.
20. Olsen ME, Bishara SE, Damon P, Jakobsen JR. Evaluation of Scotch bond multi-purpose and maleic acid as alternative methods of bonding orthodontic brackets. Am J Orthod Dentfacial Orthop 1997;111:498–501.
21. Chung LLK, Kerr WJ.The clinical evaluation of APC brackets in relation to bond failure. (online) 2011 Nov 21. Available from: URL: http://www.orthocj.com/archive/issue 6/apc.htm
22. Mavropoulos C, Staudt B, Kiliaridis S, Krejci I. Light curing time reduction: in vitro evaluation of new intensive light-emitting diode curing units.Eur J Orthod 2005;27:408–12.
23. Retamoso LB, Onofre NM, Hann , Marchioro EM.Effect of light-curing units in shear bond strength of metallic brackets: an in vitro study.J Appl Oral Sci. 2010;18(1):68-74.
24. Koupisa NS, Eliades T, Athanasios E.Clinical evaluation of bracket bonding using two different polymerization sources. Angle Orthod 2008;78:922-25.
25. Mills RW, Jandt KJ, Ashworth SH. Dental composite depth of cure with halogen and blue light emitting diode technology. Br Dent J 1999;186:388-391.
26. Dunn WJ, Taloumis LJ. Polymerization of orthodontic resin cement with light-emitting diode curing units. Am J Orthod Dentofacial Orthop 2002;122:236–24.
27. Usumez S, Buyukyilmaz T, Karaman AI. Effect of light-emitting diode on bond strength of orthodontic brackets. Angle Orthod 2004;74:259–63.
28. Mavropoulos C, Staudt B, Kiliaridis S, Krejci I. Light curing time reduction: in vitro evaluation of new intensive light-emitting diode curing units.Eur J Orthod 2005;27:408–12.Galindo HR, Sadowsky PL, Vlachos C, Jacobson A, Wallas D. An in vivo comparison between a visible light cured bonding system and a chemically cured bonding system. Am J Orthod Dentofacial Orthop 1998;113:271-75.
29. Cerekja E, Cakirer B. Effect of short curing times with a high-intensity light-emitting diode or high-power halogen on shear bond strength of metal brackets before and after thermocycling. Angle Orthod 2011;81:510–16.
30. Swanson T, Dunn WJ, Childers DE, Taloumis LJ.Shear bond strength of orthodontic brackets bonded with light-emitting diode curing units at various polymerization times. Am J Orthod Dentofacial Orthop 2004;125:337-41.
31. Thind BS, Stirrups DR, Charles H, Lloyd.A comparison of tungsten-quartz-halogen, plasma arc and light-emitting diode light sources for the polymerization of an orthodontic adhesive. Eur J Orthod 2006;28:78–82.
|