INTRODUCTION
Caries, because of its uniqueness as a disease, its ubiquitous nature, and its stubborn resistance to resolution remains as one of man’s most common, oldest, and singly costliest ailment. The total health handicap due to dental caries is staggering and has become a dichotomous disease especially in children. With an age of specialization and compartmentalization of knowledge there has been a decline in prevalence of caries but it still remains a vestigial remnant of bygone time 1. The reduction in caries prevalence has not occurred uniformly for all dental surfaces. With the advancement in oral hygiene awareness and preventive measures there is decline in prevalence of smooth surface caries. But despite of increased understanding of disease process & the availability of effective intervention, many lesions involving occlusal fissures, still progress to the stage where tooth surface is compromised and invasive intervention and restoration are required because of complex invaginated anatomy and minute dimensions of fissures. [Rohr et al.,
1991; Wang et al., 1994; Hannigan et al., 2000] 2
Accurate and reliable diagnosis of non-cavitated occlusal caries is important because these lesions can be arrested at an early stage by preventive measures and if not diagnosed can lead to unnecessary loss of tooth structure. For several decades the accepted method for detection of caries had been visual examination. “Seeing is believing” was the approach adopted by Europeans as diagnostic aid which was modified by C.F.MAURY in 19th century with invention of mouth mirror.3 This combination of visual examination and probing were the mainstay of occlusal caries diagnosis for years because it is acquired easily, requires no special maintenance other than sharpening & does not require additional training, extra time, and special sterilization procedures. Fraction4. That is why visual examination has been used as a diagnostic method in this study. Unfortunately vision alone as a diagnostic tool may leave much to be desired. This realization, coupled with the observation that the use of the dental explorer in the historical manner resulted in an unacceptably high proportion of false-positive
diagnoses on occlusal surfaces, and transfer of cariogenic micro-organisms from one site to another [Loesche et al., 1979]5 indicate that use of visual examination was of limited value for the detection of occlusal caries. Therefore, to complement traditional visual examination use of aided visual examination i.e. with intraoral camera for diagnosis of caries is done in this study, to enhance the reproducibility and efficacy of visual examination. Intraoral camera is a feasible alternative to a visual oral examination for caries screening as it gives a magnified view (x10) and large range of viewing angles. [Ekstrand et al., 1995; Verdonschot et al., 1999].6
But these do not enhance detection of initial occlusal caries lesions in enamel of either permanent or deciduous teeth [Flaitz et al., 1986; Nytun et al., 1992; Ketley and Holt, 1993]. 7,8
Tools based on fluorescence were introduced to overcome this problem. Laser fluorescence (LF) seems to be promising for the detection and quantification of caries lesions on occlusal surface [Hibst and Gall, 1998; Shi et al., 2000; Sheehy et al., 2001]9. Carious lesion scatters the reflected light more than that of sound enamel. (Angmar –Mansson and Ten Bosch, 1987, Backer-Dirks,1966; Neilson and Pitts,1991; Angmar –Mansson et al ,1996)10 Based on this Hibst and Gall (1998) found that red light induced fluorescence (655nm) could reveal considerable contrast between sound and carious tooth tissue and introduced DIAGNOdent (Hibst et al 2001) 11. Fluorescence was found to be more intense in carious tissue (140 relative fluorescence intensity) as compared with sound tissue (20 relative fluorescence intensity). Hence, due to its good reproducibility and validity DIAGNOdent has been proved as a valuable adjunct in early detection of caries. Therefore, in the present study DIAGNOdent is used for early detection and quantification of occlusal caries.
The importance of early detection of caries activity is emphasized by the fact that an incipient carious lesion which are amenable to remineralization can be arrested, reversed or restored with minimal invasion13 Therefore, the aim of this study was to assess the validity and reproducibility of three different methods (visual examination, visual examination with intraoral camera, DIAGNOdent) for early detection of occlusal carious lesions
MATERIALS AND METHODS
Subject Selection
The sample consisted of 48 children ranging between 5-14 years of age with enamel and / or dentine caries The Ethics Committee in D.J.College of Dental Sciences & Research, Modinagar approved the study before the start. Consent was taken from the patients. Inclusion criteria for teeth in this study were the apparent absence of occlusal restorations and fissure sealants, absence of hypoplastic pits, advanced degree of fluorosis, frank occlusal cavitation and large carious lesions on smooth and approximal surfaces.
A total of 100 sites were selected from 48 children which comprise 36 1st deciduous molar, 30 2nd deciduous molar & 34 permanent first molar.(flowchart1). After oral prophylaxis careful cleaning of the occlusal surfaces with rotating bristle
brush and water, was done.
EXAMINATION METHODS:
Sterilization of instruments
Instruments used in the study were autoclaved for 45 minutes in hot air autoclave or cold sterilization accordingly.
Visual examination
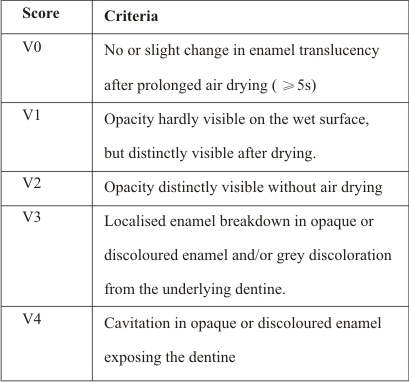
Visual inspection was performed with patients positioned in a dental chair, with the aid of a light reflector, air/water spray and plane buccal mirror using the criteria shown in table 1 [Ekstrand et al., 1997]. Visual examination was done both on wet surface and after drying with compressed air and isolation with sterilized cotton rolls. This was done because transition from sound enamel (enamel translucency) to opacity which is visible after or without air-drying is an indicator of caries initiation , and transition from opacity visible after air-drying to opacity without air-drying is an indication of caries progression (Thylstup and co-workers,1996).
INTRAORAL CAMERA
Diagnosis with intraoral camera (Miura) was also done both on wet surface and after isolation with sterilized cotton rolls. The carious lesion was examined under standard dental operating light with mouth mirror and intraoral camera using television, which shows the magnified images (10X) of the tooth examined with intraoral camera. They were scored using the criteria shown in table 1.Intraoral camera act as an enhancement aid to improve the reproducibility of visual examination
DIAGNODENT
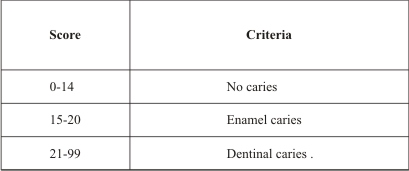
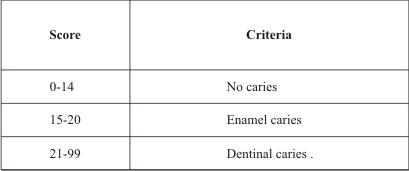
The DIAGNOdent (KAVO,Birbech Germany) measurements were conducted in accordance with the operating manual after drying the tooth for 10 second. Prior to use the instrument was calibrated in accordance with the manufacturer’s instructions and recalibrated for each examination session of approximately 25 teeth. The angle of the tip was rotated and scanned over the area of interest on the tooth surface to record the peak value which could range from 0 (sound) to 99 (caries). The readings of peak value were then recorded according to the criteria given by Lussi et al (1999) (Table 2).
OPERATIVE INTERVENTION
(Pit and fissure opening)
Operative intervention was done after interpretation of values of all three diagnostic methods.. Out of 100 teeth examined, 8 teeth had a visual score 0 and 1 (Ekstrand criteria) and DIAGNOdent value less than 15(Lussi criteria) thus indicating that no caries was present. Thus, out of 100 teeth 92 occlusal carious molars were opened with a airrotor handpiece. Penetration depth of carious lesion was estimated visually using WHO periodontal probe. The greatest extent of caries was classified according to the following score given by Ekstrand et al, 2001(Table No. 3). The restoration of carious teeth was done according to carious lesion In the teeth having caries up to outer 1/3rd of enamel enameloplasty was done. All
teeth having depth greater than 1/3rd of enamel were restored with glass ionomer cement (N100 3M ESPE)
STATISTICAL ANALYSES
The data was statistically analyzed to test the validity separately for lesion in enamel and dentine in terms of sensitivity (proportion of carious lesion identified correctly).The inter-rater agreement (Kappa) was observed for all four modalities to evaluate agreement of diagnostic modalities with respect to operative intervention.and Inter- comparision between all four diagnostic methods were done by using kappa statistics.
RESULTS :
After operative intervention was used as a gold standard it was found that out of 100 teeth, 8 had no caries ( score 0), 20 teeth had enamel caries ( score 2), 72 had caries extending up to dentine (score 2) according to Ekstrand criteria
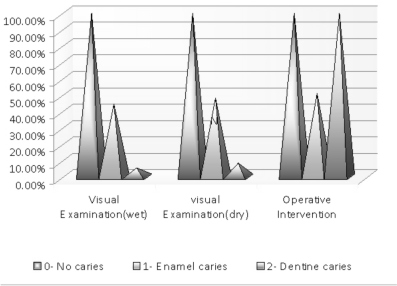
While observing visual examination on wet surface with respect to operative intervention out of 100 cases visual examination (wet) correlated 100% score 0, while it correlated only 44.4% with score 1 i.e. it gave 28 true positive results and 27 true negative results. The correlation between visual examination and operative intervention score 2 is only 5.4% i.e. it gave only 2 true positive result and 35 true negative results. (Graph 1)
While comparing visual examination on dry surface with respect to operative intervention out of 100 cases visual examination (dry) correlated 100% with score 0, while it correlated only 48.4% with score 1 The correlation between visual examination and operative intervention score 2 is only 8.4% (Graph 1)
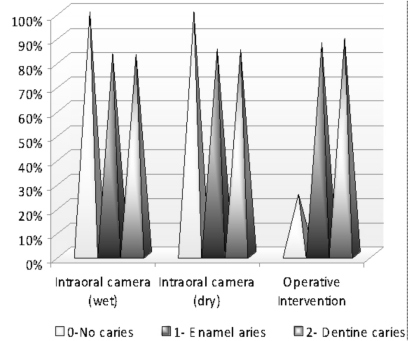
While observing intraoral camera on wet surface with respect to operative intervention out of 100 cases intraoral camera (wet) correlated 25% with score 0 i.e. gave 2 true positive results and 6 false positive results , while it correlated 82.8% with score 1 i.e. it gave 48 true positive results and 7 false positive results.
The correlation between intraoral camera and operative intervention score 2 is 100% i.e. it gave 37 true positive results. (Graph 2)
While comparing intraoral camera and operative intervention on dry surface out of 100 cases intraoral camera (dry) correlated 40% with operative intervention score 0 while it correlated 84.8% with score 1 and for score 2 is 100% i.e. it gave 37 true positive results. (Graph 2)
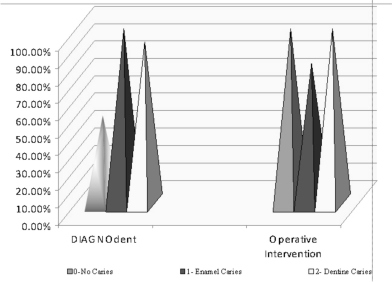
While observing DIAGNOdent with respect to operative intervention out of 100 cases DIAGNOdent correlated 100% with operative intervention score 0 i.e. gave 8 true positive results , while it correlated 80.8% with score 1 i.e. it gave 44 true positive results, 8 true negative results and 3 false positive results The correlation between DIAGNOdent and operative intervention score 2 is 100% i.e. it gave 37 true positive results.
(Graph 3)
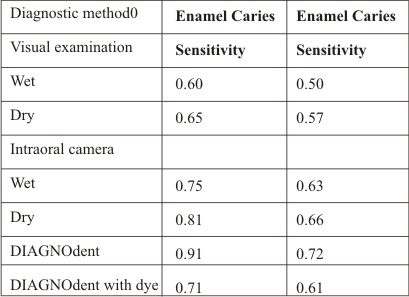
For enamel caries the sensitivity was found to be highest for DIAGNOdent i.e. 0.91 & lowest for visual examination (wet)
i.e. 0.6087. For dentine caries the sensitivity was found to be highest for DIAGNOdent i.e. 0.72 & lowest for visual examination i.e. 0.50
Thus, it was observed that out of the four methods, DIAGNOdent is more sensitive in detecting enamel and dentine caries.
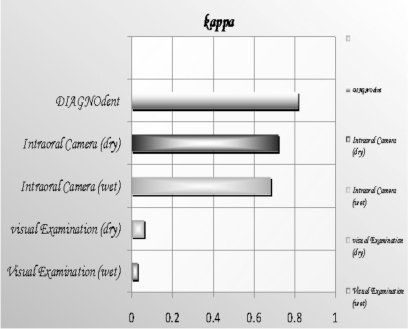
The inter-rater agreement (Kappa) was observed for all three modalities to evaluate agreement of diagnostic While observing measurement of kappa for all four test the value of kappa is highest for DIAGNOdent i.e.0.816 which signifies almost perfect agreement with operative intervention according to Landis and Koch interpretation results (1977) and is lowest for visual examination (wet) i.e.0.03 which denotes slight agreement with operative intervention ( graph 4) Thus, the results reveals that DIAGNOdent is a better diagnostic modality than other modalities used in the present study with respect to operative intervention.
INTERCOMPARISION BETWEEN METHODS.
While intercomparing kappa value between diagnostic test it was found that the value of kappa is highest between DIAGNO dent and intraoral camera (dry) i.e.0.667 which signifies substantial agreement between DIAGNOdent and intraoral camera (dry) and is lowest between visual examination (wet) and intraoral camera i.e. 0 which signifies no agreement between visual examination (wet) and intraoral camera according to Landis & Koch criteria. (Table 5)
DISCUSSION .
For both clinical and epidemiological studies, it is a fundamental premise that diagnostic methods exist which may provide consistent and standardized expressions of the condition in question. This premise places emphasis on the issue of reproducibility and validity of the diagnostic methods available [Nyvad et al., 1999]. The present investigation has demonstrated that the DIAGNOdent device is capable of obtaining high sensitivity on the occlusal sites of deciduous teeth with macroscopically intact surfaces. The performance was similar to that found in a recently published in vitro study in deciduous
teeth [Attril and Ashley, 2001] as well as in in vitro and in vivo studies in permanent teeth [Lussi et al., 1999, 2001; Shi et al., 2000].
An ideal diagnostic method should offer, among other characteristics, high sensitivity Normally, a very high specificity is obtained at the expense of reduced sensitivity. Likewise,an increase in sensitivity will be accompanied by a decrease in specificity (increase in the false-positive diagnosis). Considering that a rise in the false-positive proportion can be dangerous as it can lead to overtreatment, a technique that offers high specificity even at the expense of a slight reduction in sensitivity seems to be more appropriate [Downer, 1989]. In this study, for all diagnostic methods higher values sensitivity was found to be for DIAGNOdent i.e. 0.91 & lowest for visual examination (wet) i.e. 0.6087 A possible explanation for less efficacy and validity of visual examination in the present study can be attributed to the fact dental caries is a dynamic process, in which early lesion may undergo demineralization before being expressed clinically, thus missed visually
Among the examination methods used in
this study, the DIAGNOdent device was found to have the highest sensitivity for lesions into enamel and dentin. DIAGNOdent seems to be promising for the detection and quantification of caries lesions on occlusal [Hibst and Gall, 1998; Shi et al., 2000; Sheehy et al., 2001]. In 1998, a laser-based diagnostic system was developed using a diode laser as light source and a photodiode combined with a long-pass filter as detector [Hibst, 1999]. The teeth are illuminated by laser light (Ï = 655 nm), which is absorbed by the tooth substance. Some of this light is reemitted as near-infrared fluorescent light, and changes in the tooth substance that are associated with progression of the caries process are reflected in an increase in the amount of fluorescent light [Angmar-Månsson and ten Bosch, 1987].
When evaluating a diagnostic method it is very important to test whether it provides a reliable and minimal diagnostic variability between measurements to assure consistency and reproducibility along time. While observing measurement of kappa for all three test the value of kappa is highest for DIAGNOdent i.e.0.816 which signifies almost perfect agreement with operative intervention according to Landis and Koch interpretation results (1977) and is lowest for visual examination (wet) i.e.0.03 which denotes slight agreement with operative intervention Thus, the results reveals that DIAGNOdent is a better diagnostic modality than other modalities used in the present study. This should allow the device to be used for longitudinal monitoring of caries and thus, also, for assessing the outcome of preventive interventions.
In conclusion, this study clearly demonstrated that DIAGNO dent was the most accurate and valid system tested for the detection of occlusal caries. It has the advantage of quantifying the mineral content, helping to improve the diagnostic efficacy and treatment and accurate assessment of fissures where the visual examination alone is not adequate, thus complementing the traditional dental examination.
Hence, DIAGNO dent being a modern, noninvasive ,sensitive and easier method is an improvement on the currently available methods for detection of initial caries.
LEGENDS
Table 1 . Criteria used in visual examination (Ekstrand et al, 1998)
Table 2 . Criteria used in examination with DIAGNOdent (Lussi et al, 1999)
Table 3 . Criteria used in examination after Pit & Fissure opening ( Ekstrand et al, 2001)
Table 4 : Sensitivity and Specificity of each diagnostic method for Enamel and Dentine caries.
Table 5 : Inter-comparision values of kappa statistics of four diagnostic test
Table 1 . Criteria used in visual examination (Ekstrand et al, 1998)
Table 2 . Criteria used in examination with DIAGNOdent (Lussi et al, 1999)
Table 3 . Criteria used in examination after Pit & Fissure opening ( Ekstrand et al, 2001)
Table 4 : Sensitivity of each diagnostic method for Enamel and Dentine caries.
Table 5 : Inter-comparision values of kappa statistics of four diagnostic test
VE: Visual Examination (wet)
VEd: Visual Examination (dry)
IC: Intraoral Camera (wet)
ICd: Intraoral Camera (dry)
DIAG: DIAGNOdent
Illustrations:
Flowchart 1: Division of Sample
Graph 1 : The comparision Visual Examination and Operative Intervention.
Graph 2 : The comparision Intraoral camera and Operative Intervention
Graph 3 :The comparision DIAGNOdent and Operative Intervention
Graph 4 : The comparision of kappa of all test
Graph 1 : The comparision Visual Examination and Operative Intervention.
GRAPH 2
GRAPH 3
GRAPH 4
 |
 |
 |
|
REFRENCES:
1. Fanerjee A, Watson TF, Kidd EAM. Dentine caries excavation: a review of current clinical techniques. British Dental Journal 2000; 188: 476–482.
2. Willershausen B, Azrak B, Wilms S. Fear of dental treatment and its possible effects on oral health. European Journal of Medical Research 1999; 4:72–77.
3. Habib CM, Kronman J, Goldman M. A chemical evaluation of collagen and hydroxyproline after treatment with GK-101 (N-chloroglycine). Pharmacology and Therapeutics in Dentistry 1975; 2:209–215.
4.Goldman M,kronam JH .A preliminary report on a chemomechanical means of caries removal. J Am Dent Assoc 1976; 93(6):1149 -53.
5. Schutzbank SG, Galaini J, Kronman JH, Goldman M, Clarke REA. A comparative in vitro study of the effect of GK-101 and GK-101E in caries removal. Journal of Dental Research 1978; 57: 861–864.
6. Beeley JA, Yip HK, Stevenson AG. Chemomechanical caries removal: a review of techniques and latest developments. British Dental Journal 2000; 188: 427–430.
7. A. Lussi, S. Imwinkelried, N.B. Pitts, C. Longbottom, E. Reich. Performance and Reproducibility of a Laser Fluorescence System for Detection of Occlusal Caries in vitro. Caries Res 1999;33:261-266.
8. H. Eggertsson, M. Analoui, M.H. van der Veen, C. González-Cabezas, G.J. Eckert, G.K. Stookey. Detection of Early Interproximal Caries in vitro Using Laser Fluorescence, Dye-Enhanced Laser Fluorescence and Direct Visual Examination. Caries Res 1999; 33: 227-233.
9. Magorzata Tomasik et al. Comparison of visual and laser examination of first permanent molars in patients aged 6-7 years. Durham Anthropology Journal 1999; 12:2-3.
10 X.-Q. Shi, U. Welander, B. Angmar-Mansson. Occlusal Caries Detection with KaVo DIAGNOdent and Radiography: An in vitro Comparison. Caries Res 2000; 34: 151-158
11 Attrill D, PF Ashley. Occlusal caries detection in primary teeth: a comparison of DIAGNOdent with conventional methods. British Dental Journal 2001; 190 (8) : 440-443
12 Sheehy EC, Brailsford SR, Kidd EA, Beighton D, Zoitopoulos L: Comparison between visual examination and a laser fluorescence system for in vivo diagnosis of occlusal caries. Caries Res. 2001; 35(6): 421-6.
13 Lussi A, Megert B, Longbottom C, Reich E, Francescut P. Clinical performance of a laser fluorescence device for detection of occlusal caries lesions. European Journal of Oral Sciences. 2001 Feb; 109(1):14-19.
14 Azza A. El-Housseiny, Hana Jamjoum. Evaluation of visual, explorer, and a laser device for detection of early occlusal caries. Journal of Clinical Pediatric Dentistry.2001; 6(1): 41-48.
15 Raimund Hibst, Robert Paulus, Adrian Lussi. Detection of Occlusal Caries by Laser Fluorescence: Basic and Clinical Investigations. Medical Laser Application. 2001; 16(3): 205-213.
16 Alwas-Danowska HM, Plasschaert AJ, Suliborski S, Verdonschot EH. Reliability and validity issues of laser fluorescence measurements in occlusal caries diagnosis. Journal of Dentistry. 2002 May ; 30(4) : 129-134.
17 Heinrich-Weltzien R, Weerheijm KL, Kühnisch J, Oehme T, Stösser L. Clinical evaluation of visual, radiographic, and laser fluorescence methods for detection of occlusal caries. ASDC J Dent Child. 2002 May-Aug; 69(2): 127-32.
18 Camila Pinelli, Mônica Campos Serra, Leonor de Castro Monteiro Loffredo.Validity and Reproducibility of a Laser Fluorescence System for Detecting the Activity of White-Spot Lesions on Free Smooth Surfaces in vivo. Caries Res 2002; 36: 19-24.
19 A.M. Lennon, W. Buchalla, L. Switalski, G.K. Stookey. Residual Caries Detection Using Visible Fluorescence. Caries Res 2002; 36: 315-319.
20 Anttonen V, Seppa L, Hausen H. Clinical study of the use of the laser fluorescence device DIAGNOdent for detection of occlusal caries in children. Caries Res 2003; 37: 17-23.
21 Chong MJ, Seow WK, Purdie DM, Cheng E, Wan V. Visual-tactile examination compared with conventional radiography, digital radiography, and Diagnodent in the diagnosis of occlusal occult caries in extracted premolars. Pediatr Dent. 2003 Jul-Aug; 25(4): 341-9.
22 Rocha RO, Ardenghi TM, Oliveira LB, Rodrigues CR, Ciamponi AL. In vivo Effectiveness of Laser Fluorescence Compared to Visual Inspection and Radiography for the Detection of Occlusal Caries in Primary Teeth. Caries Res 2003; 37: 437-441.
23 A. Lussi, P. Francescut. Performance of Conventional and New Methods for the Detection of Occlusal Caries in Deciduous Teeth. Caries Res 2003; 37: 2-7.
24 Heinrich-Weltzien R, Kühnisch J, Oehme T, Ziehe A, Stösser L, García-Godoy F. Comparison of different DIAGNOdent cut-off limits for in vivo detection of occlusal caries. Oper Dent. 2003 Nov-Dec; 28(6): 672-80
25 Pinheiro I V A, Medeiros M C, Ferreira M A, Lima K C. Use of laser fluorescence (DIAGNOdent) for in vivo diagnosis of occlusal caries. J of Minimal Intervention Dentistry 2004; 1(1): 48-51.
26 Isauremi Vieira de Assuncao Pinheiro, Maria Cristina Dos Santos Medeiros, Maria Angela Fernandes Ferreira, Kenio Costa De Lima. Use of Laser Fluorescence (Diagnodent) for in vivo diagnosis of occlusal caries: A Systematic Review. J Appl Oral Sci 2004; 12: 177- 81.
27 Reis A et al. Occlusal caries detection: a comparison of DIAGNOdent and two conventional diagnostic methods. J Clin Dent. 2004; 15(3): 76-82.
28 Shinkoku Naoko et al. The research on objective diagnosis of dental caries of permanent tooth occlusal surface in the initial stage. The relationship between measured values with explorer (probe) and DIAGNOdent. Nihon University Dental Journal 2004 ; 78 (3) : 159-164.
29 Mendes, Fausto Medeiros, Nicolau, Jose. Utilization of Laser Fluorescence to Monitor Caries Lesions Development in Primary Teeth. Journal of Dentistry for Children May-August 2004; 71( 2) :139-142.
30 Erten H et al. The assessment of unaided visual examination, intraoral camera and operating microscope for the detection of occlusal caries lesions. Oper Dent. 2005 Mar-Apr; 30(2): 190-194. diagnosis of occlusal occult caries in extracted premolars. Pediatr Dent. 2003 Jul-Aug; 25(4): 341-9.
22 Rocha RO, Ardenghi TM, Oliveira LB, Rodrigues CR, Ciamponi AL. In vivo Effectiveness of Laser Fluorescence Compared to Visual Inspection and Radiography for the Detection of Occlusal Caries in Primary Teeth. Caries Res 2003; 37: 437-441.
23 A. Lussi, P. Francescut. Performance of Conventional and New Methods for the Detection of Occlusal Caries in Deciduous Teeth. Caries Res 2003; 37: 2-7.
24 Heinrich-Weltzien R, Kühnisch J, Oehme T, Ziehe A, Stösser L, García-Godoy F. Comparison of different DIAGNOdent cut-off limits for in vivo detection of occlusal caries. Oper Dent. 2003 Nov-Dec; 28(6): 672-80.
25 Pinheiro I V A, Medeiros M C, Ferreira M A, Lima K C. Use of laser fluorescence (DIAGNOdent) for in vivo diagnosis of occlusal caries. J of Minimal Intervention Dentistry 2004; 1(1): 48-51.
26 Isauremi Vieira de Assuncao Pinheiro, Maria Cristina Dos Santos Medeiros, Maria Angela Fernandes Ferreira, Kenio Costa De Lima. Use of Laser Fluorescence (Diagnodent) for in vivo diagnosis of occlusal caries: A Systematic Review. J Appl Oral Sci 2004; 12: 177- 81.
27 Reis A et al. Occlusal caries detection: a comparison of DIAGNOdent and two conventional diagnostic methods. J Clin Dent. 2004; 15(3): 76-82.
28 Shinkoku Naoko et al. The research on objective diagnosis of dental caries of permanent tooth occlusal surface in the initial stage. The relationship between measured values with explorer (probe) and DIAGNOdent. Nihon University Dental Journal 2004 ; 78 (3) : 159-164.
29 Mendes, Fausto Medeiros, Nicolau, Jose. Utilization of Laser Fluorescence to Monitor Caries Lesions Development in Primary Teeth. Journal of Dentistry for Children May-August 2004; 71( 2) :139-142.
30 Erten H et al. The assessment of unaided visual examination, intraoral camera and operating microscope for the detection of occlusal caries lesions. Oper Dent. 2005 Mar-Apr; 30(2): 190-194.
|