Introduction:
Teeth found in excess of the normal dental formula are called supernumerary teeth. These are called supplemental teeth if they closely resemble normal teeth or rudimentary if they are abnormal in shape and size. The most common sites for the occurrence of supernumerary teeth, listed in order of frequency, are the maxillary midline, maxillary molar, mandibular premolar, maxillary lateral incisor, mandibular molar and the maxillary premolar regions1. Supernumerary teeth may occur singly or in multiples, unilaterally or bilaterally and in one or both the jaws.1-3The incidence of supernumerary teeth in the general population is fairly common- approximately 1 in every 110 persons4.
It has been found that the incidence of supernumerary premolars is more common than previously estimated.4 This may be because 75% of these teeth are impacted, unerupted and generally asymptomatic thus avoiding detection. A majority of supernumerary premolars are of the supplemental type and develop later than their normal counterparts.
Multiple case reports describing supernumerary premolars have appeared in the literature over the years.5-11 Solares and Romero4 reviewed most of these reports published in the dental literature since 1932 and found that they are the most common supernumerary teeth in the mandibular arch (7%) and their incidence is much higher than previously reported. Supernumerary premolars have a predilection for the mandibular arch (74%) and are less frequent in the maxillary arch (26%).12,13 They occur three times more frequently in males than in females, indicating a sex-linked inheritance.4 Patients with a previous history of supernumerary teeth have a 24% possibility of developing single or multiple supernumerary premolars at a later age.4
The etiology of supernumerary teeth remains unclear, but several theories have been suggested, both genetic and environmental, for their occurrence such as hyperactivity of the dental lamina, dichotomy of the tooth bud and proliferating epithelial remnants of Hertwig's root sheath.1,4,14 Many syndromes and developmental conditions have been associated with single and multiple supernumerary teeth such as Gardner's syndrome, cleidocranial dysplasia and cleft lip and palate.1,2
The occurrence of multiple supernumerary teeth without any associated systemic conditions or syndromes however is rare, double supernumeraries being found in only 12-13% of cases and multiple in less than 1% of cases.15
Although it does not appear to follow a simple mendelian pattern of inheritance, the prevalence of supernumerary teeth in the relatives of affected subjects has been found to be much greater than the general population.4 This paper describes the presence and management of multiple supernumerary premolars in two siblings, giving further support to the genetic factor in the aetiology of supernumerary teeth.
Case One:
Case one was a 15-year old boy who reported to the department of orthodontics with a complaint of irregular teeth. The medical and dental history was non-significant. Clinical examination revealed a permanent dentition with a class II malocclusion. There was crowding in both the arches with the maxillary right canine blocked out labially and an upper midline shift to the right. The panoramic radiograph (Fig.1) showed the presence of all permanent teeth till the third molars including two supernumerary premolars in the mandible, one each on the right and left sides. Both the supernumerary premolars were developing between the second premolars and the first molars and in close proximity to the roots of the second premolars. The supernumerary premolar on the right side showed crown formation while the left one was in the early calcification stage. Space analysis for the case indicated treatment on an extraction basis. Hence treatment began with the removal of upper first premolars. The supernumerary premolars were extracted surgically under local anaesthesia along with the corresponding lower second premolars of each side. Comprehensive orthodontic treatment followed after the extractions.
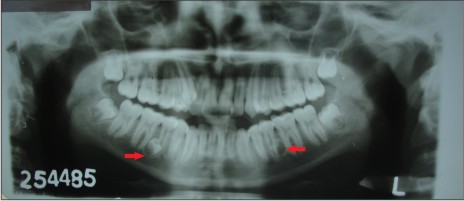 | Fig. 1: Panoramic radiograph of case 1 showing bilateral mandibular supernumerary premolars
 |
Case Two:
Case one was accompanied by his elder brother, aged 19. We decided to examine him after the panoramic radiograph revealed the presence of supernumerary premolars in his younger brother. Clinical examination showed a class 1 occlusion with mildly rotated mandibular incisors. All the permanent teeth till the third molars were present along with a supernumerary tooth which had erupted on the lingual of the lower left side between the first and second molars (Fig.2). Panoramic examination (Fig.3) revealed the presence of two additional unerupted supernumerary premolars, one each in the mandibular and maxillary left segments. The maxillary supernumerary premolar was developing between the first and second premolars while the mandibular supernumerary premolar was present between the second premolar and first molar. Treatment options were discussed with the patient and it was decided to extract the erupted supernumerary tooth in the mandible and monitor the other two supernumerary premolars at six monthly intervals.
 | Fig. 2: Intra-oral photograph of case 2 showing an erupted supernumerary tooth in the mandibular left quadrant
|
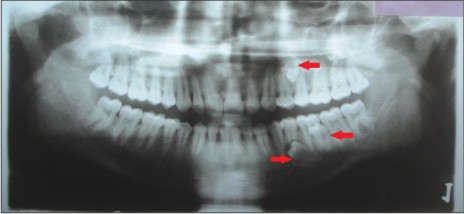 | Fig. 3: Panoramic radiograph of case 2 showing multiple supernumerary teeth
|
Discussion:
The importance of genetic factors in the aetiology of supernumerary teeth has been well recognized by many authors1,2,4,12. The trait has been described as an autosomal dominant one, with lack of penetration in some generations.16 Only a few cases of supernumerary premolars among siblings have been reported in the literature. Scanlan and Hodges17 reported supernumerary premolars in a brother and sister. Mercuri and O'Neill18 reported a case of supernumerary premolar teeth among siblings with a family history including a grandparent and the father. Another case of supernumerary premolars at the age of 12 years with a previous history of mesiodens at an earlier age was reported to have a female cousin with a similar intervention at age 7 years19 .Orhan et al15 reported the presence of non-syndromal multiple supernumerary teeth involving both jaws in two children and their mothers. A recent report described the presence of supernumerary premolars in two siblings with a similar number and location.20 Our report of two siblings with multiple supernumerary premolars lends further credence to the genetic theory.
Unerupted supernumerary teeth that are asymptomatic generally do not appear to affect the dentition in any way and may be left in situ. However, there is a possibility of complications such as dentigerous cyst formation and root resorption, although it has been reported that only 2% of supernumerary premolars exhibited any pathological changes.21 This has led some authors to recommend that they should be left untreated rather than risk surgical damage given the close proximity of these teeth to the roots of the permanent teeth.1 There is also a potential for these teeth to affect normal occlusal development and they may cause rotations, delayed eruption or impactions.1,4,7 They may also interfere with orthodontic mechanics such as space closure and root uprighting.22,23 In case one, which was indicated for comprehensive orthodontics, the presence of two supernumerary premolars in the mandibular arch would have interfered with the treatment mechanics. Hence extraction of the supernumerary premolars was indicated. This was done simultaneously with the extraction of the permanent mandibular second premolars which prevented surgical complications such as damage to adjacent roots and minimized psychological trauma to the patient. In the second case, only the erupted supernumerary premolar was extracted while the unerupted ones were left in place and kept under observation.
Supernumerary teeth are often discovered incidentally on panoramic radiographs taken prior to orthodontic treatment as was the case with our first patient. Localization of the unerupted supernumerary teeth may be done with the parallax method using two radiographs taken at different angles. Cone beam tomography has recently been used to evaluate supernumerary teeth and may soon become the method of choice because of the detailed three-dimensional images it provides24. Once they have been discovered, decision regarding the appropriate management should be made carefully keeping the risk-benefit ratio in mind with the consent of the patient/parents.
Conclusion:
The presence of multiple supernumerary premolars in siblings has been presented. These findings give support to the role of genetics in the aetiology of supernumerary teeth. Dentists and orthodontists should be aware of the possibility of familial occurrence of supernumerary teeth. Management of these teeth requires careful consideration.
References:
1. Rajab LD, Hamdan MAM. Supernumerary teeth: review of the literature and a survey of 152 cases. IntJ Paediatr Dent 2002;12:244-254.
2. Yusof WZ. Non-syndrome multiple supernumerary teeth: literature review. J Can Dent Assoc 1990; 56:147-149.
3. Stafne, EC. Supernumerary teeth. Dent Cosmos 1932;74:653-659.
4. Solares R, Romero MI. Supernumerary premolars: a literature review. Pediatr. Dent 2004;26:450-8.
5. Hall A, Onn A. The development of supernumerary teeth in the mandible in cases with a history of supernumeraries in the pre-maxillary region. J Orthod 2006;33: 250-255.
6. Mopager V, Sudha P, Anegundi RT, Kulkarni S, Tavarageri A. Supplemental premolars in a 13 year old child- a case report. J Indian Soc Pedo Prev Dent 2002;20(4):169-72.
7. Shapira Y, Haskell BS. Late developing supernumerary premolar. J Clin Orthod 1981;15:571.
8. Chadwick SM, Kilpatrick NM. Late development of supernumerary teeth: a report of two cases. Int J Paediatr Dent 1993;3(4):205-210.
9. Cochrane SM, Clark JR, Hunt NP. Late developing supernumerary teeth in the mandible. Br J Orthod 1997;24(4):293-296.
10. Breckon JJ, Jones SP. Late forming supernumeraries in the mandibular premolar region. Br J Orthod 1991;18(4):329-331.
11. Kawashita Y, Saito T. Nonsyndromic multiple mandibular supernumerary premolars: a case report. J. Dent Child 2010;77(2):99-102.
12. Scheiner MA, Sampson WJ. Supernumerary teeth: a review of the literature and four case reports. Aust Dent J 1997;42:160-165.
13. Grahnen H, Lindahl B. Supernumerary teeth in the permanent dentition: a frequency study. Odontol Revy 1961;12:290-294
14. Primosch RE. Anterior supernumerary teeth-assessment and surgical intervention in children. Pediatr Dent 1981;3:204-215.
15. Orhan AI, Ozer L, Orhan K. Familial occurrence of nonsyndromal multiple supernumerary teeth. Angle Orthod 2006;76(5):891-7.
16. Batra P, Duggal R, Parkash H. Non-syndromal multiple supernumerary teeth transmitted as an autosomal dominant trait. J Oral Pathol Med.2005;34:621-5.
17. Scanlan PJ, Hodges SJ. Supernumerary premolar teeth in siblings. Br J Orthod 1997;24(4):297-300.
18. Mercuri LG, O'Neill R. Multiple impacted and supernumerary teeth in sisters. Oral Surg Oral Med Oral Pathol 1980;50:293.
19. Becker A, Bimstein E, Shteyer A. Interdisciplinary treatment of multiple unerupted supernumerary teeth; report of a case. Am J Orthod 1982;81:417-22.
20. Cho SY. Multiple supernumerary premolars in two siblings: a case report. Prim Dent Care 2009;16(3):111-5.
21. Bodin I, Julin P, Thomsson M. Hyperdontia. I. Frequency and distribution of supernumerary teeth among 21,609 patients. Dentomaxillofac Radiol 1978;7(1): 15-17.
22. Shah A, Hirani S. A late-forming mandibular supernumerary: a complication of space closure. J Orthod 2007;34:168-172.
23. Jamwal R, Sharma P, Sharma R. Late-developing supernumerary mandibular premolar: a case report. World J Orthod 2010Winter;11(4):e94-8.
24. Shah A, Gill DS, Tredwin C, Naini FB. Diagnosis and management of supernumerary teeth. Dent Update 2008;35(8):510-20.
|