Introduction
The fracture of acrylic dentures is an unresolved problem in removable prosthodontic. Typically, the ratio of maxillary and mandibular complete denture facture is about 2:1[1]. Fracture can be caused as a result of impact if a denture is accidentally dropped on a hard surface or by fatigue failure when a denture base is repeatedly deformed under occlusal forces [2].The most common types of fractures are de-bonding/fractures of denture teeth (33%) in complete and partial dentures followed by midline fractures of complete dentures (29%) [3]. Fracture is most commonly seen in maxillary complete dentures and characterized by midline fractures. [1], [3],[4],[5]
Fractures in dentures result from twodifferent types of forces, namely, flexuralfatigue and impact. Flexural fatigueoccurs after repeated flexing of a materialand is a mode of fracture wherebya structure eventually fails after beingrepeatedly subjected to loads that are sosmall that one application apparently doesnothing detrimental to the component.This type of failure can be explained by the development of microscopic cracksin areas of stress concentration. Withcontinued loading, these cracks fuse toan ever growing fissure that insidiouslyweakens the material. Catastrophic failureresults from a final loading cycle thatexceeds the mechanical capacity of theremaining sound portion of the material. [6]
The midline fracture in a denture is often a result of flexural fatigue. Impact failures usually occur out of the mouth as a result of a sudden blow to the denture or accidental dropping whilst cleaning, coughing or sneezing. [7]
Fracture may be due to a multiplicity of factors rather than the denture base material itself and these factors have been discussed in detail [8]. For example, any factor which increases the deformation of a denture base; [9], [10] additional factors which form areas of stress concentration such as a large frenal notch; [11] dentures with thin or under-extended flanges; poorly fitting dentures or a lack of adequate relief; dentures with a wedged or locked occlusion; poor clinical design and dentures which have been previously repaired. [12], [13]
This article illustrates a clinical report which describes the factors that contribute to the midline fracture of the maxillary denture and its management. Recognition of these factors and their prevention or correction will result in a maxillary denture that is physiologically and functionally acceptable for the patient for an extended period of time.
Clinical Report
A 54 years old male patient reported in clinic with history of fracture of maxillary complete denture 3 times. Intraoral examination reveals that patient had high ridge with a flat crest and nearly parallel maxillary residual alveolar ridge, class III (According to House Classification) labial frenum, class I (According to House Classification) buccal frenae, V-shaped hard palate and prominent midpalatine raphe. Palpation of midpalatine raphe area and alveolar ridge revealed that there is marked difference in mucosal resiliency and mucosa is loosely attached at midpalatal area (Fig - 1).
On examination of maxillary prosthesis it reveals the labial notch was too broad but encroached to labial frenum, maxillary teeth were arranged too buccally and anterior interferences were also present (Fig-2). The thickness of acrylic denture base was approximately 3mm in palatal area. The fracture line was extending from labial notch to the post dam area throughout the midline (Fig-3).
 | Fig.1 : V - Shaped Palate & Prominent Midpalatine Raphe.
 |
 | Fig 2 : Over-trimmed Labial Notch.
|
 | Fig.3 : Fracture Line Of Maxillary Complete Denture.
|
Management
Prosthodontic management started right from the diagnosis. Preliminary impression was made with impression compound (DPI Impression compound, Mumbai) and diagnostic castwas made. Palpation of midpalatine raphe area and alveolar ridge mucosa revealed that there is marked difference in mucosal resiliency. To compensate this, modification was done in spacer design by increasing the thickness of spacer twice in midpalatine raphe area, by providing umbrella spacer along with full arch spacer (Fig - 4). This provides more thickness of impression material to record the midpalatine area in relived state. The final impression (wash impression) was made with zinc oxide eugenol impression paste (DPI Impression paste, Mumbai) (Fig -5).
 | Fig.4 : Modified Spacer Design.
|
 | Fig.5 : Final Maxillary Impression.
|
After orientation jaw relation record, vertical and centric jaw relation record were made. The neutral zone was recorded at the time of maxillo-mandibular relationship recording by swallowing technique. Teeth were arranged in neutral zone with bilateral balance occlusal scheme to reduce the lateral forces on residual ridge and torsional forces on acrylic denture base (Fig -6 a, b).
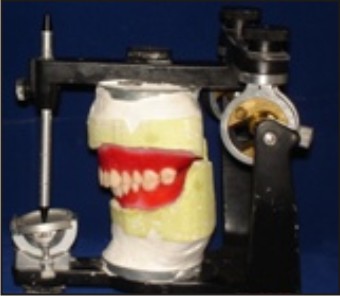 | Fig.6 (A) : Teeth Arrangement In Bilateral Balance Occlusion
|
 | Fig.6 (B) : Teeth Arrangement In Bilateral Balance Occlusion
|
After denture try in, denture was processed with high impact acrylic denture base material (Luciton 99, Dentsply Canada Ltd.). During denture insertion the maxillary denture was relived in midpalatine area (Fig - 7). Special care was taken during adjustment of labial notch, that is labial frenum was relieved properly neither it impinge to frenum during function nor over trimmed.
 | Fig. 7 : Extra Relief In Midpalatine Area.
|
Discussion
Denture fractures result primarily from flexural fatigue following repeated flexing of denture base. This type of failure can be explained by the development of microscopic cracks in area of stress concentration [1], [4], [6]. In order to understand and resolve the problem of complete denture fracture, it is essential to identify the regions of stress concentration.
In this clinical report, repeated fracture of maxillary complete denture occurred due to low and broad (class III) labial frenum, labial notch in maxillary denture was over trimmed, too buccally arranged teeth.
Previous studies indicate stress always follows the same trend of increasing to a maximum at the tip of the frenum notch [14] and stress concentrates in anterior palatal areas of maxillary dentures rather than in posterior regions [5]. Fracture of the denture bases may be due to the weakening effect of the frenum notch, concentration of stress in the anterior palatal region, material fatigue caused by alternate force, or by the reduced strength of the base material as a result of unsatisfactory processing in the laboratory. [5], [14], [15], [16] Labial frenum should record properly during preliminary and final impression, should trimmed properly to accommodate the labial frenum and placing a thin beading around a labial frenum to improve the seal.
Palatal relief in the anterior portion of palate is planned to reduce excess load over median palatine suture. Modification in spacer design was done by increasing the thickness of spacer wax twicein midpalatine area, by providing umbrella spacer along with full arch spacerto provide extra relief in this area. This provides more thickness of impression material to record the midpalatine area in relived state.
Teeth arrangement was done in neutral zone according to bilateral balance occlusal scheme to distribute the occlusal forces uniformly.
A majority of the midline fractures can be avoided by the application of established Prosthodontic principles during denture construction. The principles include even and adequate bulk of denture base material cured to achieve optimum polymerization and free of porosity; relief of incompressible tissue in the center of the hard palate; addition of labial flange to increase rigidity of denture base as well as even and balanced occlusion to reduce wedging effect and locking of occlusion. Improvements in denture base resin and the reduction of stress concentrators such as notches and diastema to minimum would also help prevent these fractures.
However, when no such improvements are possible, yet fracture remains a problem – usually because of exceptionally high occlusal loading – a stronger denture base material is often indicated, e.g. cobalt – chromium alloy denture bases, stainless steel palates, Modified polymeric denture base materials like Carbon fibres, Ultra-high-modulus polyethylene fibres (UHMPE), Glass fibres, Metal strengtheners that possessing better physical strength. [13], [17]
The flexible denture is a promising material for preventing midline fractures in a single maxillary denture. It is well tolerated by the patients as compared to the methyl meth-acrylate dentures.[18] Implant supported overdenture also may be the treatment option in that case.
Conclusion
A technique has been presented that allows the practitioner to prevent and correct the most common and recurrent type of fracture in maxillary complete denture e.g. midline fracture by proper recording and relieving labial notch area, by giving anterior palatal relief , by doing teeth arrangement in neutral zone according to bilateral balance occlusal scheme.
References
1. Beyli MS, Von fraunhofer JA. An analysis of causes of fracture of acrylic resin dentures. J Prosthet dent 1981; 46:238-41.
2. Kim SH, Watts DC. The effect of reinforcement with woven E-glass fibers on the impact strength of complete dentures fabricated with high –impact acrylic resin. J Prosthet dent 2004; 91:274-80.
3. Darbar UR, Huggett R, Harrison A. Denture fracture – A survey. Br Dent J 1994; 176: 342-5.
4. Kally E. Fatigue failure in denture base polymers. J Prosthet dent 1969; 21: 257-66.
5. Vallittu PK, lassila VP, lappalainen R. evaluation of damage to removable dentures in two cities in Finland. Acta Odontol Scand 1993; 51:363-9.
6. Wiskott HWA, Nicholls JI, Belser UC. Stress fatigue: Basic principles and prosthodontic implications. Int J Prosthodont 1995; 8: 105-16.
7. Jagger DC, Harrison A, Jandt KD. The reinforcement of dentures. J Oral Rehabil 1999; 26: 185-94.
8. Jagger DC, Harrison A. The fractured denture-solving the problem. J Primary Dent Care 1998; 5: 159-62.
9. Kydd WL. Complete base deformation with varied occlusal tooth form. J Prosthet Dent 1956; 6: 714-18.
10. Lambrecht JR, Kydd WL. A functional stress analysis of the maxillary complete denture base. J Prosthet Dent 1962; 12: 865-72.
11. Rees JS, Huggett R, Harrison A. Finite element analysis of the stress concentrating effect of fraenal notches in complete dentures. Int J Prosthodont 1990; 3: 238-40.
12. Yunus N, Harrison A, Huggett R. Effect of microwave irradiation on the flexural strength and residual monomer levels on an acrylic repair material. J Oral Rehabil 1994; 21: 641-8.
13. Some clinical problems and solutions. R M Basker, J C Davenport. Prosthodontic treatment of edentulous patients. Blackwell : Munksgaard, 2002: 289-94.
14. Rees JS, Huggett R, Harrison A. Finite element analysis of the stress concentrating effect of fraenal notches in complete dentures. Int J Prosthodont 1990; 3: 238-40.
15. Shim JS, Watts DC. An examination of stress distribution in a soft – lines acrylic resin mandibular complete denture by finite element analysis. Int J Prosthodont 2000 ;13: 19-24.
16. Nishigawa G, Mastunaga T, Moryo T, Okamoto M, Natsuaki N, Minagi S. Finite element analysis of the effect of bucco-lingual position of artificial posterior teeth under occlusal force on the denture supporting bone of the edentulous patient. J Oral Rehabil 2003; 30: 464-52.
17. Gogu#5;ă, L. M., Bratu, D., Jivănescu, A., Erimescu, R. and Mărcău#5;eanu, C. Glass fibre reinforced acrylic resin complete dentures: a 5-year clinical study. Gerodontology 2012; 29: 64–69.
18. RK Dhiman, SK Roy Chowdhury. Midline fractures in single maxillary complete acrylic Vs flexible dentures. Armed Forces Med J India 2009; 65:141-5.
|