Introduction
Tooth agenesis is a common developmental anomaly that appears in 2.2-10% of the general population (excluding agenesis of third molars). Tooth agenesis is an informative term because it implies the underlying developmental defects.[1] Congenital tooth agenesis can be either hypodontia (agenesis of fewer than six teeth excluding third molars) or oligodontia (agenesis of more than six teeth excluding third molars) and anodontia is the extreme of oligodontia where there is total absence of any dental structure.[2]
Oligodontia can occur either as an isolated condition (non -syndromic oligodontia) or be associated with cleft lip\palate and other genetic syndromes (syndromatic oligodontia)[3]. Isolated cases of missing teeth can be familial or sporadic in nature.[4]
Hypodontia has a prevalence of 1.6% to 9.6% in the permanent dentition, excluding agenesis of the third molars. Oligodontia has a population prevalence of 0.3% in the permanent dentition.[2] It is genetically a heterogenous trait.[5] Oligodontia occurs more frequently in girls at a ratio of 3:2. Agenesis of only the third molars has a prevalence of 9% to 37%. In the deciduous dentition, hypodontia occurs less often (0.1%-0.9%) and has no significant sex distribution.[6],[7] Congenital absence of teeth most commonly occurs with the maxillary lateral incisors, second premolars and mandibular central incisors.[8]
In the literature many terms are used to describe missing teeth, like oligodontia, anodontia, Aplasia of teeth, congenitally missing teeth, absence of teeth, agenesis of teeth and lack of teeth.[4]
Definition/diagnosis criteria: A tooth is defined as congenitally missing if it has not erupted in the oral cavity and is not visible in the radiograph. All primary teeth have erupted by the age of 3 years and all permanent teeth except third molars between the ages of 12 and 14 years. Therefore 3-4 year old children are suitable for diagnosis of congenitally missing primary teeth by clinical examination and 12-14 year old children, for diagnosis of permanent teeth excluding the third molars.[9],[10] The use of panoramic radiography is recommended, together with clinical examination for the detection or confirmation of dental development and performing the diagnosis of hypodontia.[10] It may be unilateral or bilateral.[5] Morphologic dental anomalies may involve a single tooth, groups of teeth, or the entire dentition.[8]
The cause for congenital absence of teeth could be due to any of the following reasons
1) physical obstruction or disruption of the dental lamina,
2) space limitation, and functional abnormalities of the dental epithelium
3) Failure of initiation of the underlying mesenchyme.[2]
The present report describes a case that involves two siblings, suggesting a strong genetic reason for the anomaly without any systemic complications.
Case Report
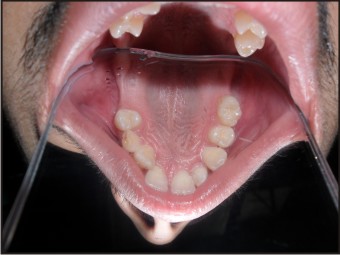
A patient reported with a chief complaint of missing teeth. Patient gave no significant medical and dental history, neither there was any abnormality detected on general examination, suggestive of any syndrome however patient gave a family history of his brother and mother having such a problem. On intraoral examination of probands 22 teeth were present .The teeth present were 15 14 13 12 11 21 22 23 24 25 31 32 33 34 35 36 41 42 43 44 45 46.(Fig 1) (Fig 2) (Fig 3).
 | Fig 1 : clinical picture of patient Harmanjot showing presence of few maxillary teeth 15 14 13 12 11 21 22 23 24 25
 |
 | Fig 2 : clinical picture of patient Harmanjot showing presence of few mandibular teeth 31 32 33 34 35 36 41 42 43 44 45 46.
|
 | Fig 3 : OPG showing multiple missing teeth of the patient harmanjot in both arches
|
Probands male sibling had 11 13 54 15 21 22 23 24 25 31 32 33 34 75 36 41 42 43 44 45 48 (Fig 4) (Fig 5) (Fig 6).
 | Fig 4 : clinical picture of brother showing presence of few maxillary teeth 11 13 54 15 21 22 23 24 25
|
 | Fig 5 : clinical picture showing presence of few mandibular teeth 31 32 33 34 75 36 41 42 43 44 45 48
|
 | Fig 6 : OPG showing multiple missing teeth of the brother in both arches
|
Probands mother aged 45 yrs had 11 13 14 21 22 23 24 25 32 33 34 35 36 42 43 44 45 46.(Fig 7) (Fig 8) (Fig 9).
 | Fig 7 : clinical picture of mother showing presence of few maxillary teeth 11 13 14 21 22 23 24 25
|
 | Fig 8 : clinical picture showing presence of few mandibular teeth 32 33 34 35 36 42 43 44 45 46
|
 | Fig 9 : OPG showing multiple missing teeth of the mother in both arches
|
Probands maternal grandfather had undergone total extraction for the purpose of complete denture so could not be evaluated.
12 and 16 were missing and patient had previous history of extraction these teeth.
All three patients were advised OPG which revealed that the mother had 36 that was distoangularly impacted near the lower border of mandible.
Congenitally missing teeth of three generations of a family and the spousal influence on the oligodontia of the third generation was investigated. For clarification, a review of commonly used terms is included in the paper. Although there are a number of factors affecting the failure to develop permanent tooth buds, most researchers believe that an autosomal dominant trait is responsible for the oligodontia in this family. Oligodontia is predicted to affect fifty percent of the fourth generation. It may vary in penetrance and expression.[11] Many syndromes are associated with oligodontia, but none seem to be prevalent in this family. A feature noted in this three generation pedigree is missing permanent maxillary first molars. This is considered rare, especially when few abnormal ectodermal findings are reported. Additional findings include an increased number of missing teeth, decreased tooth size and a prominent maxillary labial frenum. The dental treatment for patients affected will likely involve a multidisciplinary approach. The treatment is particularly important since the lack of a full complement of teeth impacts the emotional and physical well-being of the individual.
Discussion
The development of human dentition is a complex process regulated by a sequence of reciprocal interactions between the epithelial and mesenchymal tissue components. Signal molecules and growth factors from several different families and their specific receptors, as well as several transcription factors have been associated with epithelial - mesenchymal signalling during tooth morphogenesis.[12],[13] This complex regulation is reflected in numerous inherited conditions with dental aberrations.[14]
Agenesis of some teeth is a common human anomaly. Approximately 21% of the population lacks one or more third molars and if third molars are not considered, 8% lacks one or more teeth.[14] Specific terms are used to describe the nature of tooth agenesis like hypodontia: 1-6 teeth missing (excluding third molars) and anodontia: total absence of any dental structure.[15]
Prevalence becomes progressively smaller as the number of missing teeth increases as seen in oligodontia, with an overall prevalence of 0.14%.[16] A higher frequency has been noted in females than males with no difference in the distribution of missing teeth over maxilla / mandible and left and right sides.[17]
In general hypodontia is the term most frequently used when describing the agenesis of one or few teeth. Hypodontia is an anomaly that may result in dental malpositioning, periodontal damage, lack of development of maxillary and mandibular bone height and has significant psychological, aesthetic and functional consequences.[2],[7] Oligodontia, a severe and rare form of tooth agenesis, is defined as the absence of six or more permanent teeth, with the absence of less than six teeth referred to as hypodontia. For oligodontia, a prevalence of 0.16% has been reported. It is associated with several syndromes, but is also inherited as an isolated trait.[17]
Hypodontia and oligodontia are classified as isolated or non-syndromic hypodontia/oligodontia and syndromic hypodontia/oligodontia or hypodontia/oligodontia associated with syndromes.[7] Most often oligodontia appears as part of some congenital syndromes that affect several organ systems.[7] Oligodontia can occur in association with various genetic syndromes, such as ectodermal dysplasia, incontinentia pigmenti, Down syndrome, Rieger syndrome, Wolf-Hirschhorn syndrome , Van der Woude syndrome, Ectrodactyly- ectodermal dysplasia-clefting syndrome, Cleft lip palate ectodermal dysplasia syndrome, Oral facial digital syndrome type I , Witkop tooth-nail syndrome, Fried syndrome, Hair- nail- skin- teeth dysplasias, Hirschhorn syndrome, Hemi facial microsomia and Recessive incisor hypodontia.[2] When oligodontia is associated with a syndrome there may be abnormalities of the skin, nails, eyes, ears and skeleton.[2],[7]
Although tooth agenesis is caused by environmental factors like infection to the tooth bud, trauma, drugs chemotherapy or radiotherapy, but strong genetic component has also been suggested.[2] The heritability of congenitally missing teeth has been shown in many studies.[7] The genetic factors may be dominant or recessive and it is obvious that in many cases multiple genetic and environmental factors are acting together.[7] The importance of genetic factors is shown by appearance of multiple cases among relatives and higher concordance in identical than in non-identical twins.[2],[7] It is also reported that several genes which, when defective, cause congenitally missing teeth.
Oligodontia as well as hypodontia are highly heritable conditions associated with mutations in the AXIN2, MSX1, PAX9, EDA, and EDAR genes.[18] Oligodontia, the congenital absence of six or more permanent teeth, is a common developmental anomaly of human dentition whose genetic basis is poorly understood. It has been recently reported that a non syndromic form of oligodontia involving mostly all permanent molars in large kindred, caused by a frame shift mutation in exon 2 of the human PAX9 gene and hypothesized that molar oligodontia is due to allelic heterogeneity involving different mutations in PAX9. Pedigree analysis revealed that the oligodontia trait is inherited in an autosomal dominant fashion. Mutational analysis of PAX9 thus far excludes the presence of the previously identified frame shift mutation.[19]
Non-syndromic tooth agenesis has wide phenotypic heterogeneity and is classified as either sporadic or familial, which can be inherited in an autosomal-dominant, autosomal-recessive, or X-linked mode. Dominant mutations in MSX1, PAX9, and AXIN2 have been found in families with non-syndromic tooth agenesis. Mutations in MSX1 segregate with tooth agenesis that involves predominantly second premolars and third molars. Mutations in PAX9 have been identified as the defects responsible for missing permanent molars. However, mutations in these genes were detected in only a few affected individuals, suggesting that there may be other unidentified genetic defects responsible for this disease. PAX9 plays important roles in development and organogenesis. Pax9 knockout fail to form teeth beyond the bud stages. Like the Pax9 knockouts, Msx1 knockouts also lack teeth, and their development is arrested at the bud stage. In contrast to mutations in man, heterozygous Pax9 and Msx1 mouse mutants exhibit no obvious defects. The lower gene dosage appears to be critical for proper development of the more complex human dentition. Furthermore, it remains unknown as to why PAX9 and MSX1 mutations appear to cause different phenotypes. It is possible that PAX9 plays a special role in the development of molar teeth, which show a development distinct from that of other permanent teeth, as they lack deciduous predecessors, instead arising directly from the distal extension of the dental lamina.[14]
It was investigated in Finnish family affected with oligodontia, in which mutational analysis of PAX9 by exon sequencing identified a novel mutation, C76T. The resulting phenotype is distinct from previously reported oligodontia phenotypes caused by mutations in PAX9. For this family, in which oligodontia was inherited as an autosomal-dominant trait, results strongly suggested that the phenotype was caused by the mutation C76T. The mutation results in the substitution of tryptophan for an arginine in exon 2 of PAX9, representing the first missense mutation this far. This mutation appeared in all affected family members. Sequence comparison of all available PAX sequences from different species shows that the arginine at a homologous position was absolutely conserved, whereas the neighbouring amino acids showed considerable variation. In humans, three mutations in homologous arginine have been reported. The arginine is mutated to leucine in PAX3 in one family with Waardenburg's syndrome type 1[20], in PAX6 to glycine in a family with anterior segment abnormalities of the eye[21], and in PAX8 to histidine in one patient with hypoplasia of the thyroid gland.[22]
This far, four different PAX9 mutations have been reported in families affected with severe lack of permanent teeth, in particular of permanent molars and premolars. Characteristically, when a premolar or molar tooth is missing, all the posterior teeth on the same hemi arch are also absent.[23],[24],[25],[26] Oligodontia of molar teeth was most pronounced in a family with complete deletion of one copy of the PAX9 gene. Several second premolars were missing, even though the neighbouring first molar existed, rather resembling the phenotype seen previously in association with mutations of MSX1. In addition to missing teeth, it was noticed that smaller tooth size in affected family members. Reduced permanent tooth size is common in patients with hypodontia or oligodontia.[27], [6] It is worth noting that in their proband, aged six, the deciduous teeth were also reduced in size. Their results indicated that reduction of tooth size associated with tooth agenesis may be caused by a mutation of a single gene.[14]
Nine different genes code for the human PAX molecules, all contains a paired box domain characteristic of all PAX proteins. The condition most probably results from a mutation in the PAX9 gene. It seems that in addition to molars, normal development of all teeth, including incisors, canines, and premolars, depends on the function of the PAX9 gene.[14]
Two novel missense mutations, Leu27Pro (L27P) and Ile29Thr (I29T) in the paired-domain of PAX9 have been identified in case of oligodontia. Analysis of homologous PAX proteins indicated that these two substitutions may affect the function of the PAX9 protein. Results showed that the mutations did not alter the nuclear localization of PAX9. EMSA and luciferase reporter assays indicated that both the mutated proteins could not bind DNA or transactivate the BMP4 promoter.[28]
Mutations were identified in the EDARADD, AXIN2, MSX1, and PAX9 genes, respectively. EDARADD mutations have been reported in a few families segregating hypohidrotic ectodermal dysplasia and EDARADD mutation is also associated with isolated oligodontia.[18]
Recently, a mis sense mutation in the EDA gene has been reported in a Chinese family with X-linked non-syndromic hypodontia. Following this report, another mutation (p.Gln358Glu) was detected in affected members of an Indian family with X-linked hypodontia. Unlike XLHED, affected persons in both families had no other clinical features but tooth agenesis. Specifically, affected males in both families exhibited oligodontia, with 6-24 teeth absent, while almost all female carriers were normal or had a milder phenotype. Therefore, EDA gene might be a candidate gene for non-syndromic oligodontia in affected males. EDA gene encodes the protein ectodysplasin-A (EDA), a member of the tumor necrosis factor (TNF) super family. EDA is a type II transmembrane protein with a C-terminal TNF homology domain consisting of 10 predicted anti-parallel β-sheets linked by variable loops. The TNF homology domain forms a homotrimer which is required for interaction with the receptor at the monomer–monomer interface. Mutations in the TNF domain affect the interaction of EDA with its receptors, ectodysplasin-A receptor (EDAR) and ectodysplasin-A2 receptor. The missense mutations observed in the study were all located within the TNF-like domain (residues 245–391) of EDA. It was found that these mutations can also affect the interaction of EDA with its receptors, which correlates with the non-syndromic phenotype.[29]
It has been identified a consanguineous Pakistani family where oligodontia is inherited along with short stature in an autosomal-recessive fashion. Increased bone density was present in the spine and at the base of the skull. It was identified that a 28 Mb homozygous stretch shared between affected individuals on chromosome 11q13. Screening selected candidate genes within this region, identification of homozygous nonsense mutation, Y774X, within LTBP3, the gene for the latent TGF-β binding protein 3, an extracellular matrix protein believed to be required for osteoclast function[30]
Mutations in different genes may cause different types of oligodontia i.e. different sets of teeth are missing. Perhaps the best family study of tooth agenesis was done by Grahnen in 1956.[31] He found that if either parent had one or more congenitally missing teeth, there was an increased likelihood that their children also would be affected. This familial relationship suggests that the genes are important. Comprehensive literature review shows only countable number of cases reporting maximum number of congenital missing of permanent teeth. Tsai et alhave reported a case of oligodontia in 6-year-old female patient with congenital absence of 16 permanent teeth.[32] Akkya et alin their case report of 16-year-old patient have reported oligodontia of 6 permanent teeth.[33] Rasmussen P9 reported 9-cases of non-syndromic oligodontia with 14 - 24 missing teeth excluding third molar.[34] Nagveni NB et al have reported a case of non syndromic oligodontia in a 13-year old patient with 14 missing teeth.[35] Guruprasad R et al have reported a case of non-syndromic oligodontia in a 9-year old patient with 26 missing teeth hypodontia. The present case report shows developmental agenesis of 8 permanent teeth excluding the third molars with no identifiable etiology. Oligodontia was not associated with family history and the patient was not suffering from any syndromes or systemic disorders. However the genetic evaluations were not performed.[2]
Oligodontia and hypodontia have similar associated anomalies. Several dental anomalies have been reported together with congenitally missing teeth. Examples of these are delayed formation and eruption of teeth, reduction in tooth size and form, malposition of teeth (ectopic maxillary canines and ectopic eruption of other teeth), infraposition of primary molars, teeth with short roots, taurodontism, rotation of premolars and or maxillary lateral incisors, enamel hypoplasia, hypocalcifation and dentinogenesis imperfecta.[36], [37]
The present case involve female patient along with her brother and mother with almost equal distribution of missing teeth over maxilla and / mandible and left and right sides.
In the reported case Oligodontia was also determined in the patients’ kindred via family history and it revealed no definite etiologic relationship whereas missing teeth were found to be more than six without involvement of any systemic disorders or syndromes suggesting isolated or non syndromic Oligodontia. The incidence of missing teeth may vary considerably depending upon dentition, gender, and demographic or geographic profiles. The dentition in oligodontia manifests in a wide diversity.
In our case we reported seven permanent teeth (molars) were missing excluding the third molars. The patient was ruled out for being associated with any syndrome and systemic disorder. Thus, congenital lack of more than six permanent teeth without any systemic disorder or syndrome was suggestive of Idiopathic Non Syndromic Oligodontia in Permanent Dentition.
In this modern world, hypodontia is often encountered by the dental practitioners. Hence the use of OPG is recommended, together with clinical /systemic examination for the detection or confirmation of dental development and coming to the diagnosis of hypodontia / Oligodontia
Conclusion
Current understanding of rare conditions like oligodontia may be enhanced by reporting of such cases. Oligodontia cases should be evaluated carefully for the presence of any syndromes and managed appropriately. Patients suffering from oligodontia may have severe functional, esthetic and psychological problems. When compared with other clinical groups, children with oligodontia appear to have worse oral health-related quality of life than children withdental decay and malocclusion, but better oral health-related quality of life than children with oro-facial condition.[38] Thus, early diagnosis and treatment of these patients is very important. Dental treatment can vary depending on the severity of the disease and generally requires a multidisciplinary approach. Treatment options include orthodontic therapy, implants, adhesive techniques, removable partial prostheses, fixed prostheses and over dentures. Treatment not only improves speech and masticatory function but also has psychological implications that may greatly help in regaining self-confidence of the patient.
References
1. Vastardis H. The Genetics of Human Tooth Agenesis: New discoveries for understanding Dental Anomalies. Am J Orthod Dentofacial Orthop 2000; 117:650-56
2. Hiremath Mallayya C. Nonsyndromic Oligodontia: A rare case report. AOSR 2012; 2 (2):103-7.
3. Frenkel B, Blinder D, Penn M.Isolated Oligodontia: A Case Presentation and Review of the Literature. Refuat Hapeh Vehashinayim 2010; 27(2):6-9.
4. Vanishree G, Surekha VSR.Oligodontia of Permanent Teeth- Rare Case Report. AEDJ 2010; 2(4):101-04.
5. PratibhaRS, Nihal NK. Oligodontia of Permanent Dentition: A Case Report. AEDJ 2010; 2(4):225-8.
6. Brook AH, Elcock C, Al-Sharood MH, McKeown HF, Khalaf K, Smith RN.Further studies of a Model for the Etiology of Anomalies of Tooth Number and Size in Humans. Connect Tissue Res 2002; 43:289- 95.
7. Cakur B, Dagistan S, Bilge M. Nonsyndromic Oligodontia in Permanent Dentition: Three Siblings.The Internet Journal of Dental Science 2006; 3:2.
8. Kumar M, Sai Sankar AJ, Srikanth RK. Pyramidal Molar Roots in Primary and Permanent Dentition Along with Non Syndromic Oligodontia in a 11 year Old Boy. AEDJ 2010; 2(4):36-9.
9. Guruprasad R, Nair PP, Hegde K, Singh M: Nonsyndromic Oligodontia- A case report. IJDA 2011; 3: 450-3.
10. White SC, Pharoah MJ .Oral radiology principles and interpretation. In: White SC (Ed).Dental anomalies. St. Louis, PA: Mosby; 2000:305-306.
11. Stimson JM, Sivers JE, Hlava GL.Features of oligodontia in three generations. J Clin Pediatr Dent 1997; 21(3):269-75.
12. Jernvall J, Thesleff I.Reiterative signaling and patterning during mammalian tooth morphogenesis. Mech Dev 2000; 92: 19–29.
13. Nieminen P, Pekkanen M, Åberg T, Thesleff I. Gene expression in Tooth. Developmental Biology Programme Finland: Institute of Biotechnology, University of Helsinki, 2003, http://biteit.helsinki.fi.
14. Lammi L, Halonen K, Pirinen S, Thesleff I, Arte S, Nieminen P.A Missense Mutation in Pax 9 in a family with distinct phenotype of Oligodontia. European Journal of Human Genetics 2003 ;( 11):866–71.
15. Stewart RE, Barner TK, Troutman KC, Wei SHY.Pediatric dentistry, scientific foundations and clinical practice. 1st Ed, St Louis; CV Mosby Company; 1982:87-109.
16. Polder BJ, Van't Hof MA, Van der Linden FPGM, Kuijpers Jagtman AM.A meta-analysis of the prevalence of dental agenesis of permanent teeth.Community Dent Oral Epidemiol 2004; 32:217-26.
17. Rolling S, Poulsen S. Oligodontia in. Danish school children. Acta Odontol Scand 2001; 59:111-2.
18. Bergendal B, Klar J, Stecksén-Blicks C, Norderyd J , Dahl N. Isolated oligodontia associated with mutations in EDARADD, AXIN2, MSX1, and PAX9 genes. Am. J. Med. Genet 2011; 155: 1616–22.
19. Frazier-Bowers SA, Scott MR, Cavender A, Mensah J, D'Souza RN. Mutational analysis of families affected with molar oligodontia. Connect Tissue Res. 2002; 43(2-3):296-300.
20. Hoth CF, Milunsky A, Lipsky N, Sheffer R, Clarren SK, Baldwin CT: Mutations in the paired domain of the human PAX3 gene cause Klein–Waardenburg syndrome (WS-III) as well as Waardenburg syndrome type I (WS-I). Am J Hum Genet 1993; 52: 455–62.
21. Hanson IM, Fletcher JM, Jordan T et al: Mutations at the PAX6 locus are found in heterogeneous anterior segment malformations including Peters' anomaly. Nat Genet 1994; 6: 168–73
22. Macchia PE, Lapi P, Krude H et al: PAX 8 mutations associated with congenital hypothyroidism caused by thyroid dysgenesis. Nat Genet 1998; 19: 83–6
23. Stockton DW, Das P, Goldenberg M, D'Souza RN, Patel PI: Mutation of PAX9 is associated with oligodontia. Nat Genet 2000; 24: 18–9.
24. Nieminen P, Arte S, Tanner D et al: Identification of a nonsense mutation in the PAX9 gene in molar oligodontia. Eur J Hum Genet 2001; 9: 743–6.
25. Frazier-Bowers SA, Guo DC, Cavender A et al: A novel mutation in human PAX9 causes molar oligodontia. J Dent Res 2002; 81: 129–33.
26. Das P, Stockton DW, Bauer C et al: Haploinsufficiency of PAX9 is associated with autosomal dominant hypodontia. Hum Genet 2002; 110: 371–6.
27. Schalk-van der Weide, Steen WH, Beemer FA, Bosman F: Reductions in size and left–right asymmetry of teeth in human oligodontia. Arch Oral Biol 1994; 39: 935–9
28. Liang J, Song G, Li Q, Bian Z.Novel missense mutations in PAX9 causing oligodontia. Arch Oral Biol 2012; 57(6):784-9.
29. Song S, Han D, Qu H, Gong Y, Wu H, Zhang X et al. EDA Gene Mutations Underlie Non-syndromic Oligodontia. J Dent Res. 2009; 88(2): 126–31.
30. Noor A, Windpassinger C, Vitcu I, Orlic M, Rafiq MA, Khalid M et al. Oligodontia Is Caused by Mutation in LTBP3, the Gene Encoding Latent TGF-^6; Binding Protein 3. The American Journal of Human Genetics 2009; 84(4): 519-23.
31. Grahnen H. Hypodontia in the permanent dentition. Clinical and genetical Investigation. Odont Revy 1956; 7:15-9.
32. Tsai PF, Chiou HR, Tseng CC. Oligodontia – A case report. Quintessence Int 1998; 29:191-3
33. Akkya N, Kiremitci A, Kansu O. Treatment of a patient with Oligodontia: A case report. J Contemp Dent Pract 2008; 9:121-7.
34. Rasmussen P. Severe Hypodontia: diversities in manifestations. J Clin Pediatr Dent 1999; 23:179-88
35. Nagveni NB, Umashankar KV, Radhika NB, Satisha TS: Non-syndromic oligodontia- Report of a clinical case with 14 missing teeth. BJMS 2011; 10:200-2.
36. Ghazahfaruddin M, Mishra G, Hassebuddin S, Mishra A. Oligodontia of permanent teeth A rare case report. Indian J Stomatol 2011; 2(4):285-7.
37. Gupta DK, Kamal M, Sharma H, Gupta S. Idiopathic Non-syndromic Oligodontia in permanent dentition. A case report IJDS 2012; 4(2):67-9.
38. Locker D, Jokovic A, Prakash P, Tompson B.Oral health-related quality of life of children with oligodontia. Int J Paediatr Dent. 2010; 20 (1):8-14.
|