Introduction
Oral health is an integral part of general health. It directly and indirectly reflects the overall well-being of an individual, thus maintaining oral hygiene becomes a crucial factor. Oral cavity is free of micro-organisms at birth because the fetus develops in a well-protected environment, but soon after it is habituated by numerous micro-organisms.[1] It may be due to exposure to polluted environment which contains various micro-organisms or change in dietary habits of the child as it grows. Oral diseases can be greatly controlled by reducing the microbial load in the oral cavity and this can be achieved by maintaining proper oral hygiene. Brushing teeth is the primary mode of oral hygiene practice. In earlier days, chewing sticks like Miswak, Neem and Babul were the sole oral hygiene aids used by different populations.[2] Later, toothbrush crept in as a main component among all oral hygiene aids, as a result of civilization. In 1844, the first toothbrush was manufactured by hand and patented as a three-row brush of serrated bristles with large tufts by Dr. Meyer. L. Rhein.[3] Tooth brushes are the most commonly used oral hygiene aid to promote oral health and prevent dental diseases.[4] Unfortunately, proper care of toothbrush is often neglected and is kept in bathrooms which are a good place to harbor millions of micro-organisms. The reason attributed to this toothbrush maintenance. Retention and survival of micro-organisms on toothbrush after brushing represents a possible cause of re-contamination of the mouth.[5] Prolonged use of the toothbrush facilitates contamination by various micro-organisms such as Streptococcus, Staphylococcus, Escherichia Coli and lactobacilli.[6],[7] These micro-organisms are implicated to cause dental caries, gingivitis, stomatitis, infective endocarditis in an individual, affecting both oral and general health.[5],[8] The average life span of a manual toothbrush is approximately 3 months.[9] Hence, American Dental Association (ADA) recommends change of toothbrushes once in 3–4 months based on fraying of toothbrush bristles as it decreases the cleaning effectiveness.[10],[11] However, attention was not given to the microbial contamination when the recommendation for frequency of change of toothbrush was given. Many studies have been conducted on toothbrush bristles and anchoring filaments to assess the microbial contamination and revealed microorganisms are present in the tooth brush head between the bristle tufts.[12] However, extensive exploration of the literature reveals lack of studies conducted to assess the efficacy of using tooth brush sterilizer on microbial contamination of toothbrush head. Hence, an in vitro experiment study was designed to assess the potential of using tooth brush sterilizer in sterilizing toothbrush head.
Material & Methods
Two different methods for testing were employed taking three different microorganisms into consideration. Tooth brush sterilizer was used to check its competence for Echerichia coli, Staphylococcus aureus and Salmonella typhimurium.
Test Method 1:
Bacterial cultures were grown 24 hrs and proper dilutions prepared using sterile saline blanks. Toothbrush was then inoculated into 10ml of the bacterial suspension for 10 minutes. Toothbrush was then removed from bacterial suspension and placed into 10 ml saline for 10 minutes with agitation. This solution was then counted using standard plate count methods, this being “Control Count CFU/brush”.
For second toothbrush, same procedure was carried out but toothbrush was placed into Toothbrush Sanitizer for 1 cycle that lasted up to 6minutes. The toothbrush was then placed into 10ml saline for 10 minutes with agitation to remove any remaining organisms and this solution was counted using same methods for “Remaining Organisms” after 1 cycle. The “Percent Kill” was then calculated. This same procedure was conducted for all three bacterial cultures used.
Test Method 2:
Strain to be used in the experiment was pre-cultured, and then same amounts of bacteria solution with constant concentrations were inoculated on toothbrushes. Immediately after the inoculation, sterilizing physiological saline (0.9% NaCl solution) was applied and intensely stirred which was then used as a experimental solution and the number of bacteria was measured using a plate counting method. Inoculated toothbrushes were put into a sterilizing machine (Portable Toothbrush Sterilizer) provided by the client and operated for 7 minutes. Then was the experimental solution prepared by applying the sterilizing physiological saline (0.9% NaCl solution) applied and stirring intensely, the number of viable bacteria was measured using a plate counting method. Sterilizing ability was expressed a percentage according to following equation :
Sterilizing ability (%) =
Number of viable bacteria of control – number of viable bacteria of trial x 100
----------------------------------------------
Number of viable bacteria of control
Results
Results showed that toothbrush sterilizer reduces exposure to harmful bacteria and viruses by sterilizing one of the most common breeding grounds: toothbrush.
Toothbrush is an ideal environment for the growth of salmonella, micrococcus, bacteria, viruses, and other microorganism posing a risk for tooth decay, halitosis, and a variety of illness. Toothbrush sterilizer eliminates unwanted intruders with UV Ray & Ozone. Toothbrush Sterilizer functions to eliminate unwanted and harmful bacteria, fungi and viruses that reside on the toothbrush. Using a patented UV and Ozone Sterilising lamp, 99% of these germs are eradicated from your toothbrush in approximately 6 minutes. (Table 1).
The above results showed that tooth brush sterilizer can sterilize tooth brush very effectively by killing 99.9% of the microorganisms in one cycle. (Table 2).
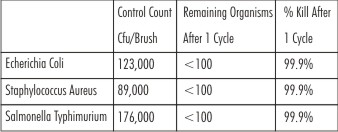 | Following Result Was Obtained In Test Method 1:
 |
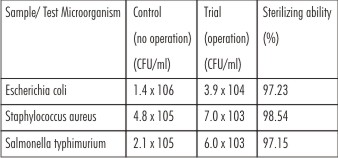 | Following Results Were Obtained When Test Method 2 Was Employed:
|
Discussion
Toothbrushes are used by millions of people everyday as part of oral hygiene procedure. Toothbrushes do a good job of removing dangerous microorganisms from teeth. Unfortunately many of these organisms remain on the brush afterwards and can re-infect our teeth. Toothbrushes also reside in a germ infested environment, namely the bathroom. Droplets from the toilet can reach the brushes and contaminate them with bacteria. Toothbrushes can get contaminated easily during their use. Retention of moisture and the presence of organic matter that has come from the mouth may promote growth of microorganisms on the toothbrush bristles. Such contamination may lead to colonization of microorganisms in the mouth and possibly infection.[Figure 1]. It is also possible that contamination of toothbrushes can occur through insects.[5],[13],[14]
 | Figure 1
|
Apart from the microorganisms taken into consideration for the study, some of the common microorganisms remaining on toothbrushes include: Mutans streptococcus - the main bacterium causing dental caries, Beta-hemolytic streptococcus - the main bacterium causing strep throat (pharyngotonsillitis), Candida albicans - the main fungus causing thrush in babies throats, Coliform bacteria - these are found in the bathroom and Herpes simplex virus - they causes cold sores.[5],[15]
Every time a person brushes their teeth, they are developing more bacterial growth on their toothbrushes. This also means that every subsequent brushing introduces new bacteria into the mouths of an individual since fresh bacteria have grown on the toothbrushes bristles and handle. Dentist tell their patients that the optimum usage time for a toothbrush is two months. However, studies conducted have shown that toothbrushes can become contaminated after four to seven days of continuous use and heavily contaminated after seventeen to twenty four days. It is relevant that tooth brushes play a major role in the contribution and retrieval of infections. Fifty five out of fifty nine patients showed improved symptoms by just changing their toothbrush every two weeks. But as consumers, changing toothbrushes every four to fourteen days can be rather impending to the expense account of an individual.[16] Brook and Gober showed that group A -hemolytic streptococci can survive on toothbrushes and suggested that the failure of treating streptococcal pharyngitis may be due to the persistence of the organism on toothbrushes and orthodontic appliances. This is useful information and not surprising since, as they point out, toothbrushes have been shown to become contaminated with other microorganisms. Based on their study, it was suggested toothbrushes be changed at least once a month and after any illness.[17] The retention and survival of microorganisms on toothbrushes pose a threat of recontamination for certain patients at risk. In an study the in vitro retention of three microbial species (Porphyromonas gingivalis, Streptococcus mutans and Candida albicans) was evaluated for three types of toothbrush. Depending on the microorganism studied, from 0.2% to 2% of the initial inoculum was retained on the brush. The number detected increased with the size of the exposed area. After 24 h, P. gingivalis and S. mutans were found on only one type of brush. C. albicans survived on all three. These results confirm that microorganisms can quickly colonize toothbrushes.[18]
Previous studies have publicized decreased rates of bacterial contamination in toothbrushes after use ofchlorhexidine which was found to be effective in disinfecting contaminated toothbrushes. However, one of the previous studies showed that Listerine was more effective.[1] The higher efficacy of chlorhexidine could be the result of the extended spectrum of action. Also, it is relatively non-toxic, odorless and is commonly used as a mouthwash. These properties may make chlorhexidine a good choice for disinfection of contaminated toothbrushes.[19] But there is always another side of the coin i.e. in general, chlorhexidine does not cause serious side effects but it can stain teeth when used as a mouth rinse and can cause irritation when used on the skin; it is also not recommended to apply this substance to the ears or eyes without medical supervision.Studies have shown that its antibacterial effects can also be neutralized by some toothpaste ingredients.Chlorhexidine in isopropyl alcohol solution has been reported to cause severe complications in neonates, such as extensive chemical burns thought to be due to reduced thickness of the stratum corneum and diminished cohesion between the dermis and epidermis, increasing skin permeability.[20],[21],[22],[23] Hibiclens[R] (4% chlorhexidine in 4% w/w isopropyl alcohol, Molnlycke Health Care Inc.) has been associated with bullous corneal keratopathy in a woman who had it applied preoperatively to her face.[24] Thus, based on the observations of previous studies, it cannot be negated that prolonged use of chlohexidine for disinfecting the toothbrush does not cause any harm to the oral mucosa. We found no clinical studies reporting levels of microbial contamination of toothbrushes whose heads can be covered with plastic caps. In one study, the use of a plastic cap leads to the growth of microorganisms like Pseudomonas aeruginosa, a gram negative aerobe and opportunistic pathogen. Therefore, it is not advisable to cover a toothbrush head with a plastic cap. Use of a cap may help retention of moisture that promotes growth of P.aeruginosa.[25]
Different studies have shown that toothbrushes are contaminated by different bacteria, viruses, and fungi after use. Since modern dentistry emphasizes prevention and infection control, toothbrushes should be correctly stored, disinfected, and changed at regular intervals. However, the literature presents few articles on the disinfection of toothbrushes.[28],[29],[30]
The present study which was done to determine the effectiveness of tooth brush sterilizer in disinfecting the tooth brushes revealed that it sterilizes toothbrush and eliminates unwanted intruders with UV Ray & Ozone. Further more, 99.9% of microorganisms are eradicated in one cycle. It is based on the principle of emission of UV (Ultra Violet) rays and activated oxygen (natural ozone) via UV and ozone lamp which combine to kill pathogenic bacteria & viruses. The UV lamp provides a dual mechanism for sterilization. UV-C, also known as germicidal UV, is most effective at wavelengths of 250-260 nanometers. Sufficient doses within this wavelength range function to create chemical and biological reactions within micro-organisms, which disturb their ability to function and reproduce, thus killing them. A Second wavelength frequency range of 180-200 nanometers generates Ozone (O3) which is a naturally occurring molecule which is the second most powerful sterilant in the world. At this wavelength range, natural Oxygen (02) is activated and links up with a free Oxygen atom (O) thus forming Ozone. Ozone acts by rupturing the cell walls and attacking the nucleus of micro-organisms which kills them. UV-C and Ozone are a formidable force in sterilizing the toothbrush. There are air vents to allow for efficient evaporation of moisture. It has a toothbrush holder that can hold tooth brush firmly in optimal position allowing for maximal sterilization efficiency.
The tooth brush sterilizer uses the same technology dentists and hospitals rely on to clean their instruments. A UV lamp is located inside a compact case, safely sterilizing the bristles and head of the toothbrush.[Figure 2]. This auto-sterilization process lasts for about six minutes before the device switches off. Thus, based on the results of the study and the technology used for sterilization, it can be postulated that regular use of tooth brush sterilizer is beneficial and absolutely safe. It should be advocated routinely for maintaining a healthy oral environment and general health status of an individual.
 | Figure 2
|
Conclusion
The toothbrush can act as an incubator for germs and bacteria, since it is located in a warm and moist environment, mainly the bathroom. While the germ-conscious have long been aware of the importance of hand washing and sanitizing kitchen work surfaces and utensils, the toothbrush is often overlooked. Toothbrush is an ideal environment for the growth of salmonella, micrococcus, bacteria, viruses, and other microorganism putting you at risk for tooth decay, halitosis, and a variety of illness.Toothbrush sterilizer eliminates more than 99.9 percent of bacteria and germs which can lead to illness, disease and bad breath. Toothbrush sterilizer reduces exposure to harmful bacteria and viruses by sterilizing one of the most common breeding grounds: toothbrush. It will sterilizes toothbrush and eliminates unwanted intruders with UV Ray & Ozone.
References
1. McCarthy C, Synder ML, Parker RP. The indigenous oral flora of man. The newborn to the 1 year old infant. Arch Oral Biol 1965;10:61-70.
2. Bhat S, Hegde KS, George R. Microbial contamination of toothbrushes and their decontamination. J Indian Soc Pedo Prev Dent 2003;21:108-12.
3. Toothbrush origin - Toothbrush history. Available from: http://www.toothbrush express.com/html/toothbrush_history.html [last accessed on 2010 Apr 20].
4. Carranza FA Jr, Newman MG. A textbook of Clinical Periodontology. 8th ed. Philadelphia: W. B. Saunders; 1996. p. 493.
5. Wetzel WE, Schaumburg C, Ansari F, Kroeger T, Sziegoleit A. Microbialcontamination of toothbrushes with different principles of filament anchoring. J Am Dent Assoc 2005;136:758-64.
6. Taji SS, Rogers AH. The microbial contamination of toothbrush: A pilot study. Aust Dent J 1998;43:128-30.
7. Fernandez V, Cesar D. Microbiology evaluation of toothbrushes. In Vitro Cell Dev Biol Anim 2006;42:31A.
8. Boylan R, Li Y, Simeonova L, Sherwin G, Kreismann J, Craig RG, et al. Reduction in bacterial contamination of toothbrushes using violight, ultraviolet light activated toothbrush sanitizer. Am J Dent 2008;21:313-7.
9. Yankell SL, Saxer UP. Toothbrushes and Toothbrushing methods. In: Harris NO, Garcia-Godoy F. Primary Preventive Dentistry. 6th ed. New Jersy: Prentice Hall; 2004. p.110.
10. ADA: Time to change that brush. Chain Drug Review 2009. Available from: http:// www. findarticles.com / p/articles/mi_hb3007/is_3_31/ai_n31352565/ [last accessed on 2010 Apr 20].
11. Glaze PM, Wade AB. Toothbrush age and wear as it relates to plaque control. J Clin Periodontol 1986;13:52-6.
12. Karibasappa GN, Nagesh L, Sujatha BK. Assesssment of microbial contamination of toothbrush head: An in vitro study. Ind J Dent Res 2011;22(1):2-5.
13. Bhat SS, Hedge KS, George RM. Microbial contamination of toothbrushes and their decontamination. J Ind Soc Pedo Prev Dent 2003;21:108-112.
14. Filho PN,Macari S,Faria G,Assed S, Ito IY.Microbial contamination of toothbrushes and their decontamination. Paediatric Dent 2000;22:381-4.
15. Sumasogi HP, Subbareddy VV, ShashiKiran ND. Contamination of toothbrush at different time intervals and effectiveness of various disinfecting solutions in reducing the contamination of toothbrush. J Indian Soc Prev Dent 2002;20:81-5.
16. "Toothbrush Contamination: A Potential Health Risk?" Quintessence International (Jan. 1986):39-42. Abstract. Medline. PubMed. 15 May 1999.
17. Fischer. Contaminated Toothbrushes & Pharyngitis. Arch Otolaryngol Head Neck Surg 1999;125(4): 479.
18. Bunetel L, Tricot-Doleux S, Agnani G, Bonnaure-Mallet M. In vitro evaluation of the retention of three species of pathogenic microorganisms by three different types of toothbrush. Oral Microbiology and Immunology 2000;15(5):313–316.
19. Nelson-Filho, Paulo –da Silva, Lea Assed Bezerre, de Silva, Raquel Assed Bezerra; da Silva, Luciana Lima, Ferreina, Paula Dariana Fernandes, Ito Izabel Yoco. Efficacy of microwave and chlorhexidine on disinfection of pacifiers and tooth brushes: An in vitro study. Pediatric Dentistry 2011;33(1):10-13.
20. Watkins AM, Keogh EJ. Alcohol burns in the neonate Journal of Paediatrics and Child Health 1992;28(4):306-8
21. Reynolds PR, Banerjee S, Meek JH. Alcohol burns in extremely low birth weight infants: still occurring. Archives of Disease in Childhood. Fetal and Neonatal Edition 2005; 90 (1): F10.
22. Mannan K, Chow P, Lissauer T, Godambe S 2007 Mistaken identity of skin cleansing solution leading to extensive chemical burns in an extremely preterm infant. Acta Paediatrica 2007; 96 (10): 1536-7.
23. Garland JS, Alex CP, Mueller CD, Cisler-Kahill LA. Local reactions to a chlorhexidine gluconate impregnated antimicrobial dressing in very low birth weight infants The Pediatric Infectious Disease Journal 1996;15(10):912-4.
24. Varley GA, Meisler DM, Benes SC, McMahon JT, Zakov ZN, Fryczkowski A. Hibiclens keratopathy. A clinicopathologic case report Cornea 1990;9(4): 341-6
25. Mehta A, Sequeira PS, Bhat G. Bacterial contamination and decontamination of toothbrushes after use. NY State Dent J 2007;73(3):20-2.
26. Kozai K, Iwai T, Miura K.. Residual contamination of toothbrushes by microorganisms. J Dent Child 1989;56:201-204.
27. Malmberg E, Birkhed D, Norvenious G, Norén JG, Dahén G. Microorganism on toothbrushes at daycare centers. Acta Odontol Scand. 1994;52:93–98.
28. Nelson-Filho P, Macari S, Faria G, Assed S, Ito IY. Microbial contamination of toothbrushes and their decontamination. Pediatr Dent 2000;22:381-384.
29. Fratto G, Nazzicone M, Ortolani E. Disinfezione degli spazzolini dentali. Ricerca sperimentale. Prev Assist Dent. 1990;16:7-10.
30. Caudry SD, Klitorinos A, Chan ECS. Contaminated toothbrushes and their disinfection. J Can Dent Assoc 1995;61:511-516.
|