Introduction
An occlusal plane according to the Glossary of Prosthodontics is defined as the average plane established by the incisal and occlusal surfaces of the teeth.[1] The occlusal plane has its own benefits both anteriorly and posteriorly. Anteriorly, it helps in achieving phonetics and esthetics whereas posteriorly, it helps in mastication.[2] Functionally, the inclination of the occlusal plane is one of the key factors governing balanced occlusion. Changes in the plane of occlusion will modify the physical and functional relationship of the oral musculature leading to an alteration in function, comfort and also in the esthetic value.[2] Hence, occlusal plane lost in patients should be re-established if the prosthesis is to be esthetically and functionally satisfactory. This can be achieved by using an occlusal plane analyzer.
An occlusal plane analyser is particularly used in patients requiring extensive reconstruction of their posterior dentition, severely worn dentition and full mouth rehabilitation cases. In such cases, it helps to assist the operator in the development of an initial mandibular occlusal plane in diagnostic casts, contours of the definitive restorations and guidelines for the actual tooth preparations.[3] Various methods have been used so far for occlusal plane analysis such as Broadrick’s Flag, custom made occlusal plane analyzer jig and cephalometric analysis. This article aims to discuss different occlusal plane analyzers for full mouth rehabilitation.
Historical Background
In 1952, JE Scott described an instrument called the bite plane leveller but this instrument could be used only to check the parallelism of occlusal plane to the ala tragus line.[2]
In 1974, Nikzad Javid described the technique of using J plane with the use of fox plane to establish occlusal plane orientation. The J - plane was meant to be used instead of metallic scale. The procedure had all the disadvantages of using fox plane.[3]
In 1992, Kazanoglu and John W Ugner introduced Camper’s plane indicator. The device consisted of two metal plates connected with a long aluminium rod. The orientation with interpupillary line and right and left Camper’s plane was done separately making it a time-consuming procedure.[2]
In 1998, Urbano, Santana - Penin and Maria J Mora described another device for determining the inclination of the occlusal plane. The device, made of stainless steel, is U – shaped with one shorter, inner arm designed to be positioned against the occlusal surface and one longer, outer arm that lies outside the mouth. The disadvantage was that a metallic scale was required to check the parallelism. Also, the parallelism with interpupillary line cannot be checked using this device.[2]
Broadrick Occlusal Plane Analyzer
Popularly known as Broadrick flag, the instrument was developed by Dr Lawson Broadrick in 1963. The original instrument is an expensive instrument and can be used with few semi adjustable articulators only which limit its use universally. To overcome the expenses, custom made Broadrick flag are popularly used now a days.
Procedure
1. On the articulator, the maxillary cast is mounted by a facebow transfer followed by mandibular cast mounting in centric relation.
2. A custom flag is fabricated using 2mm thick glass fiber sheet, stabilized with the help of metal plates and screws on the top of semi adjustable articulator. Graph paper is pasted on both the sides of the sheet.
3. The compass is placed on the anterior reference point i.e distoincisal edge of the mandibular canines and an arc of 4 inches is drawn from this position on to the graph paper. (Fig. 1)
 | Fig. 1: Anterior Reference Point
 |
4. Then the compass is placed on the posterior reference point i.e distobuccal cusp of the mandibular molar. (Fig. 2) Point where the condylar element of the articulator intersects with the condylar shaft also be used as the posterior reference point in cases of tilted, attrited or mesially drifted molars. If molar is not present, retromolar pad is used.[5] Again an arc is drawn on the graph from this position to intersect the previous arc. This point of intersection is the occlusal plane survey center.
 | Fig. 2: Posterior Reference Point
|
5. From the occlusal plane survey center, a 4 inch radius is drawn through the buccal surfaces of mandibular teeth. (Fig. 3) If there is need to raise the plane of occlusion, the survey center point is moved anterior to the arc of intersecrtion whereas to lower the plane, the point is moved posterior of the intersection.[2]
 | Fig. 3: Curve Of Spee Marked On The Cast From The Point Of Intersection
|
6. After determining the curve of spee on the mandibular cast, the occlusal surfaces of mandibular teeth are trimmed upto that line. A softened modelling wax sheet is adapted to buccal surfaces of mandibular cast. Wax is cut carefully back to this line and this wax is fitted accurately against the teeth intraorally so that it could act as occlusal plane cutting guide.
7. Then the diagnostic wax up is done on the trimmed cast and template is made with the help of putty according to the waxed up cast for provisional restorations.
This technique enables the clinician to use an analyzer with a widely used semi adjustable articulator when no such accessory is available.
Advantages
Ø Replicates maxillary teeth orientation both in frontal & sagittal plane.
Ø Canines, posteriors & hinge axis are all in the same vertical plane.
Ø The thickness of the template guides the technician, so that it is easy to work with wax or ceramic.
Disadvantages
Ø Using this method, the radius of occlusal curvature is often an arbitrary choice.
Ø The use of compass during the wax up stage is unreliable and difficult to control.
Custom Made Occlusal Plane Analyzer Jig
A jig is made of brass that consists of a horizontal platform representing horizontal reference plane which is supported by three pillars which can be raised up & down according to the requirement. Jig helps to evaluate the occlusal table slant or angulation (pitch) as it relates to the horizontal table.
Procedure
1. Maxillary cast is mounted with the help of facebow transfer.
2. The analyser jig is placed on the lower member of the Hanau articulator and is raised till the incisal edges of the maxillary cast touch the horizontal table of the jig.
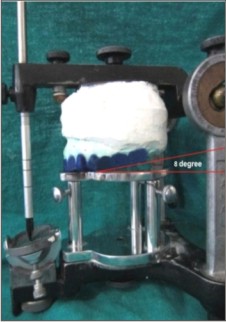
3. A 6-10 degree slant of the occlusal plane referenced from horizontal level, as measured by the protracter, is waxed with curve of spee to artistically create a soft smile line (Fig 4 and Fig 5).
 | Fig. 4: The Analyser Jig With An Angle Of 80 From The Horizontal Table
|
 | Fig. 5: Diagnostic Wax Up Completed In Accordance With The Occlusal Plane Angle
|
Advantages
Ø Allows better assessment of the maxillary occlusal asymmetries & discrepancies when referenced to the horizontal ground.
Ø Gives an accurate relationship in frontal / sagittal axis.
Ø Assists both the dentist & lab technician to better communicate a more representative occlusal plane orientation for occlusal waxing & smile design.
Ø It is a simple & inexpensive technique.
Ø Allows for a more proportional distribution & crown length ratio between the upper & lower posteriors.
Ø Prevents the need to excessively reduce the maxillary posterior occlusion during crown preparation.
Cephalometric Analysis
Cephalometric is defined as the measurement of the cranio-skeletal landmarks by means of lateral plane view radiographs of the head. It is the simplest method available for occlusal plane analysis.
Procedure
1. A lateral cephalogram of the patient is taken.
2. Two critical points that determine the curve of spee are located on this lateral cephalogram, which by definition must join the mean center of a line joining the condylar heads, between right and left (posterior point) to the mean occlusal point of mandibular incisors or canine.
3. A transparent film containing concentric circles is then overlaid on the sagittal cephalometric radiograph. The concentric circles are drawn with a radius varying from 30 mm to 180 mm at 1 cm intervals. The best circle that crosses the posterior and anterior definition points of curve of spee is then chosen. (Fig. 6).
4. Corresponding to the chosen circle on the transparent film, a template is selected from collection of clear plastic disks (Fig. 7). From the articulator, the maxillary cast is then removed and set aside for later use.
5. The hinge axis on the articulator is represented by a rigid plastic tube placed between the two condylar balls. The chosen template is placed between the hinge axis and the mandibular canine. This allows to correctly determine the height of each cusp tip during the wax procedure. (Fig. 8).
 | Fig. 6: Lateral Cephalogram With Concentric Circles
|
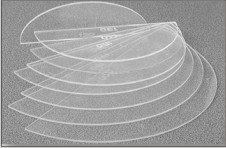 | Fig. 7: Clear Plastic Discs With Different Radii
|
 | Fig. 8: Wax Up In Accordance With The Template
|
Advantages
In comparison to the broadrick’s technique, cephalometry offers various advantages such as:
Ø Permits investigation of deep and superficial cranial and dental structures
Ø Simple and non invasive technique.
Ø Low cost.
Ø Replicates maxillary teeth orientation both in frontal & sagittal plane.
Ø Canines, posteriors & hinge axis are all in the same vertical plane.
Ø The thickness of the template guides the technician, so that it is easy to work with wax or ceramic.
Disadvantages
Ø Exposure to X-ray radiation is required which may not be a feasible option in all cases.
Ø Cephalometric machine is required which may not be available.
Discussion
Proper occlusal plane is an essential consideration when multiple long span posterior restorations are designed. The determination of the occlusal plane can have a profound effect on the short and long term success of a restorative case. The curve of Spee that determines the occlusal plane may be pathologically altered in situations resulting from rotation, tipping, and extrusion of teeth. Restoration of the dentition to such an altered occlusal plane can introduce posterior protrusive interferences. Such interferences have been shown to cause abnormal activity in mandibular elevator muscles, especially the masseter and temporalis muscle.[2] This can be avoided by reconstructing the curve of Spee to pass through the mandibular condyle.
The various occlusal plane analyzers help in re-construction of the curve of Spee in harmony with anterior condylar guidance. Their use help in proper functional and esthetic positioning of the mandibular teeth and prevents the introduction of protrusive interferences. In this article, various latest techniques for analyzing the occlusal plane have been discussed with their merits and demerits.
Conclusion
Full mouth rehabilitation entails all the procedures necessary for healthy, esthetic, well functioning and self ¬ maintaining masticatory mechanism. Various latest techniques for analyzing the occlusal plane are used for re¬establishing the decimated occlusal plane in harmony with the somatognathic system. So, all the three methods (cephalometry, broadrick analyser and custom made analyser jig) are reliable but it depends upon the clinician’s choice, availability of armamentarium and ease of using them, which technique to be used for particular cases.
Refernces
1. Glossary of Prosthodontic Terms. J Prosthet Dent 2005; 94: 10-92.
2. Chokalingam S, Rao G. Broadrick occlusal plane analyzer. J Dent Med Res Feb 2014; 13(1): 54-58.
3. R.Gupta, Occlusal Plane Analyzer: A customized Device for Determining the Occlusal plane, International Journal of Prosthodontics and Restorative Dentistry, 1(2), 2011,97-100.
4. Manvi S, Miglani S, Rajeshwari C L, Srivasta G, Arora S. Occlusal plane determination using custom made broadrick occlusal plane analyzer: a case control study, International Scholarly Research Network Dentistry, 2012, 373870.
5. Tooothaker RW, Graves AR. Custom adaptation of an occlusal plane analyzer to a semi-adjustable articulator. J Prosthet Dent 1999; 81:240-2.
6. Perez C, Re J P, Giraudeau A, Ager P, Zoghby A, Orthlieb J D. Reconstruction of the curve of spee. Stomatologie 2008; 105: 29-32.
7. Sehgal M, Kapur S, Arora A. Functional and esthetic recreation of worn out dentition. Nat J Med Dent Res Jul-Aug 2013; 1(3): 52-55.
8. Chaturvedi S, Verma A K, Ali M, Shah M. Full mouth rehabilitation using a custom made broadrick flag: A case report. IJCRI 2012; 3(5): 41-44.
|