Introduction
Edentulism is a debilitating and irreversible condition and is described as the “final marker of disease burden for oral health”. Edentulous patients are often more irritable and demanding so, must be treated with patience and understanding[1]. Although , advances in oral disease prevention and increased concern for dental care over the past several decades have resulted in recent generations of people with healthy mouths and teeth. However, there are still many people who loose some or all of their natural teeth. This is due to lack of interest on their behalf , time restraints or for various financial reasons.[2]
In routine practice the dentist frequently comes across various oral complications like bony exostosis, atrophic ridge, flabby tissue, microstomia, xerostomia, gagging, prominent pre-maxilla, bruxism etc. These complications can be easily taken care of by using unconventional techniques of fabricating dentures by utilizing advanced materials.
Apart from the above factors the most expensive commodity in a dental office is chair time. Many dentalschool courses in removableprosthodontics teachthat five or six appointmentsare necessary in fabrication of complete dentures[3]. The typical appointment sequence progresses from preliminary impressions, final impressions, jaw relation appointment, trial denture appointment and insertion appointment.[4] Any attempt to reduce the number of visits and chair time for complete denture fabrication, reduces overhead expenses and is appreciated by patients,[5] without compromising on the denture quality and patient satisfaction.[6] For the dentist one fewer appointment not only saves time but also decreases cost. Designing the denture for the patient according to the patients specific oral complaints alongwith reducing the number of clinical appointments is highly appreciated not only by the patient but also by the fellow prosthodontic community.
A critical search for methods to reduce the number of appointments for complete dentures revealed some techniques previously described in literature.[7],[8] Helft M. et al. described a technique of combining maxillomandibular relations (using intra-oral tracers) and final impressions into one appointment.[8] The disadvantage of this technique was that the impressions were made after the Gothic arch tracings were recorded. Thus the record bases remained unstable during the tracing procedure. The final impressions and the final jaw relations were made using this gothic tracing as a guide, which could be a potential source of error.[9]
Therefore, this article presents a clinical and laboratory technique that combines border molding, jaw relations, trial appointments into single clinical visit and the denture was designed in accordance with the patients oral needs of prominent pre-maxilla and gagging. The technique used in this case report, employed detachable occlusal rims and detachable handles on the same record base that facilitated recording centric relation on the same record base after the final impressions were made.
Case Report
A 45 years old female reported to the Department of Prosthodontics with the chief complaint of loose upper denture, pain while placing or removing the denture after which the pain gradually faded awayand fuller appearance of her upper lips on wearing the denture. Patient had been a denture wearer since past one year and was otherwise satisfied with the visibility and appearance of the teeth. On oral examination, it was found that the fuller appearance of lips was due to prominent pre-maxilla. The patient was hypersensitive and inspite of being an old denture wearer slight inspection of denture in the posterior region led to provocation of exaggerated gag response. Complete medical history of patient revealed that patient was diabetic and was suffering varicose veins because of which she had difficulty in walking. Therefore, considering the chief complaint and medical status of the patient, it was decided to combine final impression and jaw relation appointment in single appointment and omit the trial appointment as the patient was satisfied with the display of teeth in previous denture. To correct the lip fullness special laboratory procedure was carried out to provide maxillary flangeless complete denture to patient.
Technique
First Visit: Preliminary Impressions
Preliminary maxillary and mandibular impressions were made with impression compound (Y-Dents Impression Compositions, MDM Corporation) and primary casts were obtained.
Special laboratory procedure I:
1. Plaster index of the old maxillary denture was made so as to simulate the incisal inclination, incisal visibility and arch form of the previous denture. (Fig.1).
2. Wax spacers were adapted on the primary casts and four die pins with the sleeves were placed on to the spacers on each cast (Fig.2a). Two die pins were placed lingually in the canine region and two die pins were placed lingually in the molar region of maxillary and mandibular casts, respectively. Special care was taken to keep the pins vertically parallel to each other.
3. Temporary denture bases were fabricated using autopolymerising resin over the wax spacer with die pins and sleeves in position. (Fig.2b) Die pins were reduced in height such that they projected 2mm above the temporary denture bases and didnot interfere during jaw relation procedure
4. Aluminium foil was adapted over the temporary denture bases over which another U-shaped thin base was made with autopolymerising resin. (Fig.2c). Record rims were designed over these maxillary and mandibular U-shaped bases.
5. The U-shaped base along with record rims were removed from the temporary denture base such that the die pins came along with the bases leaving the sleeves embedded within the temporary denture bases. (Fig.2d)
6. Another set of die pins were placed into the embedded sleeves in the anterior region and over this aluminium foil was adapted (Fig.2e) followed by fabrication of detachable handles using auto-polymerising resin (Fig.2f). Thus, the modified special tray was obtained from the temporary denture bases which was shortened 2mm of the vestibule.
 | Fig 1: Plaster index of old maxillary denture
 |
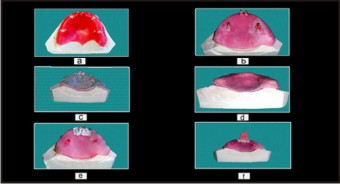 | Fig.2: (a) Waxspacer and die pins placed (b) Fabrication of temporary denture base (c) Adaptation of tin foil (d) Fabrication of U- Shaped base for occlusal rims (e) Die pins and tin foil adaptation for handle (f) Fabrication of handle
|
Second Visit: Single Step Final Impressions And Maxilla-Mandibular Jaw Relations.
• Border molding was performed on the modified special trays by hand manipulation method using green stick compound (DPI Pinnacle Tracing Sticks, DPI, India).
• The tray adhesive (UPS Tray Adhesive, 3M ESPE, Seefeld, Germany) was applied over the borders and internal surface of the modified special tray to record the final impressions accurately. The final impressions were made using light body polyvinyl siloxane material (ExpressTM Light Body, fast set,3M ESPE, Seefeld, Germany) so as to overcome the problem of gagging.
• Now, the detachable handles were removed and U-shaped record rim bases with projecting pins were placed into the sleeves embedded in the temporary denture bases.
• The final impressions with alongwith jaw relations were removed from the mouth as a single unit. Centric record was removed and detachable handles were replaced (Fig.3a).
Special laboratory procedure II:
1. Beading and boxing of final impressions was done and impressions were poured in dental stone and the articulation was done with centric record in place.
2. Final impression alongwith maxillary record base was separated from maxillary cast and a new denture base with occlusal rim was fabricated using mandibular occlusal rim as reference with record was removed from the cast.
3. Similar procedure is followed for fabrication of mandibular occlusal rims.
Special laboratory procedure III :
1. Keeping in mind patient’s chief complaint of excessive upper lip fullness with previous denture, denture flange, that provided support to the labial flange, was removed from labial aspect, forming a window, such that two prongs of denture base extended from canine eminence region, engaging the labial undercut. In addition, the maxillary anterior teeth were reduced in the form of laminates.
2. Maxillary teeth arrangement was done using plaster index of patient’s previous denture. Mandibular teeth arrangement was done keeping maxillary teeth as guide.
3. Before carrying out wax-up, tin foil was incorporated in the window area. The foil was folded and was closely adapted to the cast. The foil served for the easy separation of the lower and upper half of dental flask after investing and also prevented acrylic from flowing into the window area that was created in the temporary denture bases. (Fig.3b)
4. Investing and processing were carried out in conventional manner. After deflasking tin foil was removed and denture was finished and polished.
Third Visit: Denture Insertion
Dentures were delivered to the patient and fit, phonetics and occlusion were verified. The patient was given instructions on the use and care of the new prostheses.(Fig.3c)
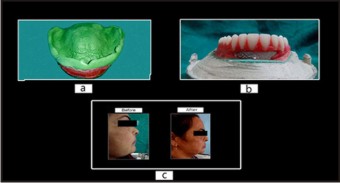 | Fig 3: (a) Centric record with final impression (b) Tin foil adaptation in window area and investing of maxillary trial denture. (c) Profile picture of patient with previous denture and with new denture
|
Discussion
This article describes the technique for fabricating anew set of complete denture in three appointments instead of the five clinical sessions. The chief complaint of the patient regarding fuller appearance of the upper lip and the problem of gag reflex were taken into consideration while providing complete denture treatment. The advantages of reducing clinical visits of the patient are convenience and the economic factor with the cost being reduced to half the cost of conventional complete denture. The benefits to the dentist is saving of chair side time to do more production.
In the past, various techniques have been described, wherein, the number of appointments were reduced to four but technique in this article focuses on reducing the appointments to three thus increasing the efficiency of the clinician.
In this particular case, special technique of border molding and jaw relations was used, in which final impressions were made prior to jaw relations, which avoided any displacement of denture bases during jaw relation records, thus enhancing the reliability of the procedure.
Moreover, since the patient experienced exaggerated gag reflex, therefore, it was planned to make impression with fast setting light body impression material that had setting time of 3.5 minutes as compared to zinc oxide eugenol impression paste that had final setting time of 10 minutes. This not only helped in saving time, recording accurately the oral tissues, obtaining better patient’s compliance, ease of handling and recording the severe labial undercut due to prominent pre-maxilla without breakage of material itself , but also the disadvantage of burning sensation caused by zinc oxide eugenol impression paste was overcome.
Patients frequently request new dentures after becoming dissatisfied with the appearance of their previous dentures. The original dentures provide valuable information that can be used to increase the success of the patient’s adaptation to the new dentures.[10] In this particular case, the patient had prominent premaxilla that made the upper the upper lip look fuller. Since, the patient precisely mentioned in her chief complaint that she is satisfied with the placement of the teeth but also specifically mentioned that she was unhappy with the fuller appearance of the old denture. Since, the patient was satisfied with the teeth arrangement of the old denture, therefore, plaster index of the teeth of previous denture was made which was used to complete the teeth arrangement, thus enabling us to omit the trial appointment.
To reduce the fullness of lips, it was planned to give a gum fitted denture to the patient. This had the advantage of providing better esthetics without surgical intervention and also prevented the tissue from undue trauma during placement and removal. Further, to decrease the lip fullness, the anterior teeth were reduce in the form of laminates that helped in curtailing the fuller appearance of upper lip. Since there was no denture base in the area of prominence, the lips and the peri oral tissues were in direct contact with the ridge which reduced the fullness of mouth.[11] Removing the acrylic and providing prongs to engage the canine eminence enabled us in achieving the esthetics without compromising denture retention and stability.
Advantages:
• Patient’s visits were reduced from five visits to three visits.
• As the record bases were stable therefore chances of error were minimal.
• Patient went satisfied with the prostheses.
Disadvantages :
• Laboratory procedures are cumbersome.
• Operator skill is required.
• Long clinical sittings may be tiring for the patient.
Conclusion
A simplified method for fabrication of complete denture was described wherein patient’s visits were reduced from five to three. Moreover, due care was given to patient’s esthetic concern for fullness and gag issues during complete denture treatment procedure. The use of this technique to fabricate complete denture benefits both the patient and clinician. By using the state of art, this technique not only reduces strain and apprehension to the patient but also reduces the cost and chair side time while still providing quality dentures. The only limitation is the excellent operator skills and good laboratory support that is required as the laboratory procedures involved are cumbersome.
References
1. Zarb GA, Bolender CL, Carlsson GE, Boucher’s Prosthodontic Treatment for Edentulous Patients, 11th edition, page 226, 1997.
2. Bergman B, Carlsson GE. Clinical long term study of complete denture wearers. J Prostht Dent 1985;53:56-61.)
3. Levin B, Richardson G, Complete Denture Prosthodontics: Clinical and Laboratory Procedures. University of Southern California School of Dentistry, 19th Edition, page 10,1995.
4. Lola Giusti. A simplified method for the fabrication of new complete denture. CDA 2007; 35:351-54.
5. Haney SJ, Nicoll R, Mansueto M. Functional impressions for complete dentures fabrication. A modified jump technique. Text Dent J 2010;127(4):377-84.
6. Obtaining maxillomandibular recordsand definitive impressions in a single visitfor a completely edentulous patient witha history of combination syndrome. J Prosthet Dent 2008;99:489-49.
7. Krantz WA et al. Combining final impressions and the centric jaw relation records into one appointment by using an irreversible hydrocolloid blockout technique. J Prosthet Dent 1991; 66(6):821-822.
8. Helft M et al.Combining final impressions with maxillomandibular relation records in stabilized record bases. J Prosthet Dent 1978; 39(2):135-138.
9. Tucker KM. Accurate record bases for jaw relation procedures. J Prosthet Dent 1966; 16(2):224-226.
10. Catherine M. Gorman, Michael O'Sullivan . Fabrication of a duplicate denture using visible light-polymerized resin as an interim denture base. J Prosthet Dent 2006;96 (5): 374-6.
11. Virag Srivastava, Laxman Singh ,Devendra , Abhishek . Gum fit denture an alternative to alveoloplasty. Journal of Dental Sciences & Oral Rehabilitation. 2011 Oct-Dec;4:51-2.
|