Introduction
Every clinician who has performed endodontics has experienced a variety of emotions ranging from the thrill-of-the-fill to an upset like the procedural accident of breaking an instrument. During root canal preparation procedures, the potential for instrument breakage is always present. When instrument breakage occurs, it immediately provokes frustration, despair and anxiety[1]. In fact, the broken instrument dilemma has caused such emotional distress that this event is frequently referred to as a “separated” or “disarticulated” file [2].
Broken instruments prevent access to the apex, and the prognosis of teeth with broken instruments in the canals may be lower than for normal ones. With the advent of rotary NiTi files, there has been an unfortunate increase in the occurrence of broken instruments and the factors contributing to breakage have been identified [3]. Various factors have been associated with the fracture of NiTi rotary instruments: operator experience, rotational speed, canal curvature, instrument design and technique, torque, manufacturing process, and absence of glide path. It has been noted that these NiTi instruments frequently fracture in narrow, curved root canals [4]. The use of ultrasonic devices has also been shown to be successful for the removal of various canal obstructions [5],[6],[7]. The advantage of an ultrasonic instrument is that it has the ability to vibrate the obstruction loose while causing minimal damage to the canal wall [8]. This paper describes three clinical aids in removing broken instruments in the root canal using hand instrumentation, ultrasonic device and nature’s way.
Material And Methods
The technique is based on: hand instrumentation for by passing the broken fragments completely or partially or ultrasonic device for loosening them. The bypassing is done by hand stainless steel K file (Denstply, Maillefer, Switzerland). A little space is obtained between the broken fragments and the dentin of canal wall by the use of K files # 20 or # 25(Denstply, Maillefer, Switzerland) completely or at least mid point is reached. K files thinner than # 20 or #25 is too flexible to obtain predictable result. K file #.8, #10, #15 K file (Denstply, Maillefer, Switzerland) is advanced along the broken fragment. During this procedure radiographs are taken to follow the progress of the instrument and prevent perforation. Solutions of Glyde (Denstply, Maillefer, Switzerland) and saline are alternatively used as canal irrigants. While using ultrasonic device ENDO 2 (Denstply, Maillefer, Switzerland) is mounted on the ultrasonic handpiece is inserted in the root canal and a trough is made in the dentinal wall around the broken instrument. The K file is mounted on the ultrasonic handpiece are not intended to prepare the root canal walls but to lossen the broken fragments from the dentine with the use of vibration. Solution 3% of Sodium Hypochlorite (Vensons, India) is used with the K file mounted on the ultrasonic handpiece. The ultrasonic K file is gently pushed up and down for 1 or 2 mm between the fragments and the root canal wall, and the broken instrument is usually loosened from the root canal wall because of the ultrasonic vibrations of the energized file. The broken fragment can then be washed out with the irrigants.
Case: 1
A 56 year old lady presented with pain in tooth #11. Pulp space therapy was planned for the patient. Pre operative radiograph was taken which revealed a broken instrument with periapical infection with respect to #11(Figure: 1A). Thus, retrival of broken instrument with retreatment was planned for the patient. After gaining access in the pulp chamber using Endo access bur (Denstply, Maillefer, Switzerland) troughing was done around the broken instrument. Around 2mm of broken instrument was made free from the canal walls (Figure: 1B). A unique technique was used to retrieve the fractured instrument a drop of feviglue was put in the canal space and fractured instrument was engaged in 18 gauge needle and was allowed to set for 5 minutes. Then, with a jerk needle was rotated in anticlockwise direction, disengaged and pulled out from the canal space (Figure: 1C). The control radiograph showed complete removal of the broken instruments, working length determination was done (Figure: 1D). The canal was prepared in the crown down technique and filled lateral condensation of gutta-percha.
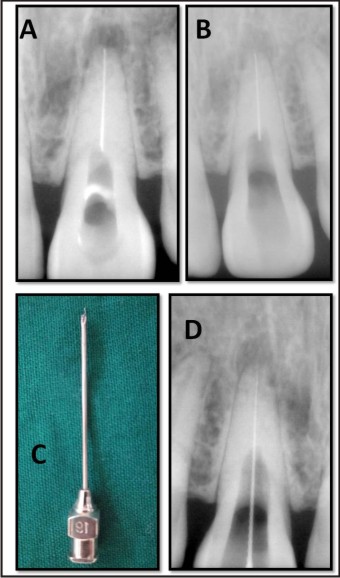 | Figure 1: A) Tooth With Broken Instrument B) Troughing Around The Fractured Instrument C) Complete Removal Of The Broken Instruments Using 18 Gauge Needle D) Working Length Determined
 |
Case: 2
A 26 year lady presented with pain at night with tooth #17. The tooth was tender to percussion. Pulp space therapy was planned. Access was gained in the pulp chamber. During biomechanical preparation led to fracture of S2 Protaper Universal file (Denstply, Maillefer, Switzerland) in the mesiobuccal root canal(Figure: 2A). ENDO-2 (Denstply, Maillefer, Switzerland) ultrasonic tip was mounted on a ultrasonic handpiece and troughing was done around the broken instrument. As described before #15 K file (Denstply, Maillefer, Switzerland) was used along the broken fragment and canal wall, instrument was loosened through ultrasonic vibration(Figure: 2B). The canal was prepeared as described earlier and obturated(Figure: 2C).
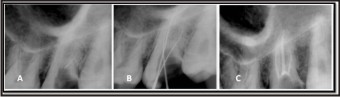 | Figure 2: A) Tooth With Broken Instruments B) Complete Removal Of The Broken Instrument And Working Length C) Obturated Tooth
|
Case: 3
A patient aged 28 year presented with discomfort in his lower anterior teeth. On intraoral examination a discolouration with tooth # 41 was observed, radiograph was taken in relation to the same. Periapical radiolucency was observed in relation to the teeth 31, 32 and 41. Vitality tests showed negative results. Pulp space therapy was planned and working length was determined (Figure: 3A). During biomechanical preparation F1 Protaper Universal file (Denstply, Maillefer, Switzerland) fractured beyond apex of tooth #31(Figure: 3B). The patient was recalled after a week for further treatment. Radiograph was taken movement of the fractured instrument into the canal was observed (Figure: 3C). Patient was observed to evaluate further changes in the movement of the fractured instrument. Patient was recalled after a week and the further movement of the fractured instrument in coronal direction in the root canal till middle third was seen (Figure: 3D). Canal was passively irrigated using the normal saline solution fractured instrument was retrieved (Figure: 3E). As described earlier canal was prepared and obturated (Figure: 3F). Thus, this could be called as nature’s way of retrieval of instrument.
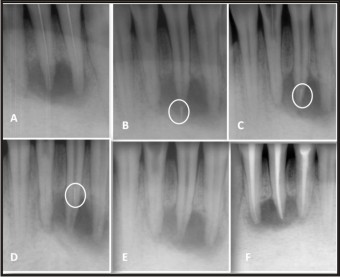 | Figure 3: A) Working Length B) Broken File Beyond Apexc) Upward Movement Of The File In The Apical Third Of The Canald) Movement Of File Uptill The Middle Thirde)After Retrieval Of Broken Filef) Obturated Tooth
|
Discussion
There are various techniques and devices which describe the removal of separated instruments lodged inside the root canal system. The removal depends on several factors: length and location of the fragment, diameter and shape of the canal, tightness of the fragment and its impaction in debris or sealer [9]. Most of them have brought about unpredictable results causing a lot of damage to the remaining root[10]. The removal of a separated instrument from a root canal must be performed with minimum damage to the tooth and the surrounding tissues[11]. Ideally, the original canal shape should be preserved as much as possible, just like during the cleaning and shaping of a canal. Canal enlargement of 40 to 50% of the root width increased susceptibility to vertical fracture[12]. In the past few years ultrasonic has been used to retrieve fractured fragments with minimal damage to dentin walls of the canal. Use of ultrasonic endodontic devices has been used in many cases and is not restricted by the position of the fragment in the root canal or the tooth involved[13].
Conclusion
The future of endodontics is bright and the demand for initial treatment and retreatment will grow significantly in the years immediately ahead. As we have seen in this article, a variety of techniques exist to address endodontically failing teeth. However, not all failures are amenable to successful nonsurgical retreatment. Clinicians need to weigh risk versus benefit and recognize that, at times, a referral, surgery or extraction might be in the patient’s best interest. Interdisciplinary excellence is the foundation for professional fulfillment, patient satisfaction and longterm success.
Refrences
1. Frank AL. The dilemma of the fractured instrument. J Endodon 1983;9(12):515-6.
2. Clifford J Ruddle. Nonsurgical retratement:post and broken instrument removal. Journal of Endodontics December 2004: 1-23
3. Berutti E, Chiandussi G, Gaviglio I, Ibba A. Comparative analysis of torsional and bending stresses in two mathematical models of nickel-titanium rotary instruments: protaper versus profile.J Endodon 2003;29(1):15-9.
4. Terauchi Y, O'Leary L, Suda H. Removal of Separated Files from Root Canals With a New File-removal System: Case Reports.J Endo.2006 Aug;32(8):789-97. Epub 2006 Jun 6.
5. O. Nagai, N. Tani, Y. Kayaba, S. Kodama and T. Osada, Ultrasonic removal of separated instruments in root canals, Int Endod 19; 986: 298–304.
6. D.H. Glick and A.L. Frank, Removal of silver points and fractured posts by ultrasonics, J Prosthet Dent 1986;55:212–215.
7. K.V. Krell, M.W. Fuller and G.L. Scott, The conservative retrieval of silver cones in difficult cases, J Endod 1984;10:269–273.
8. B.H. Gettleman, K.A. Spriggs, M.E. ElDeeb and H.H. Messer, Removal of canal obstructions with the endo extractor, J Endod 1991;17:608–611.
9. Hulsmann M. The removal of silver cones and fractured instruments using the canal finder system. J Endodon 1990;16:596-600.
10. M. Hulsmann and I. Schinkel, Influence of several factors on the success or failure of removal of fractured instruments from the root canal, Endod Dent Traumatol 1999;15: 252–258.
11. U.G.H. Fors and J.O. Berg, A method for the removal of separated endodontic instruments from root canals, J Endod 1983;9:156–159
12. L.R. Wilcox, C. Roskelley and T. Sutton, The relationship of root canal enlargement to finger-spreader induced vertical root fracture, J Endod 1997;19:533–534
13. PlotinoG,PameijerCH,Grande NM, Somma F. Ultrasonics in endodontics: a review of the literatureJ Endod. 2007 Feb;33(2):81-95
|