Introduction
Energy of the light emitted from a light-curing unit decreases drastically when transmitted through resin composite,[1] leading to a gradual decrease in degree of conversion of the resin composite material at increasing distance from the irradiated surface. Decrease in degree of conversion compromise physical properties & increase elution of monomer[2], [3], [4], [5] & thus may lead to premature failure of a restoration or may negatively affect the pulp tissue. When restoring cavities with light-curing resin composites, it has therefore been regarded as the gold standard to apply & cure the resin composite in increments of limited thickness of 2mm.[6],[7] However, restoring deep cavities with resin composite in increments is time consuming with increasing possibility of incorporating voids or contamination between the composite layers & bond failures between increments.
SureFil (Dentsply) has been introduced recently as a light curable composite material, having enough strength, so that it can be used as a restorative material for the posterior teeth which can be placed in 4-5mm thick bulks instead of current incremental placement technique without negatively affecting polymerization shrinkage, cavity adaptation and degree of conversion.
Tetric N-Ceram Bulk Fill (Ivoclar Vivadent) is a state-of-the-art, light-curing, radiopaque hybrid composite for direct restorations in posterior teeth. It comprises a newly designed patented photoinitiator in addition to the conventionally used initiator systems to achieve a material that can be quickly and reliably cured in increments of upto 4mm.
An adequate polymerization of resin composites is essential for the ultimate success of the restoration.[8] The degree of cure of resin composite materials influences their mechanical properties, solubility, dimensional stability, color change and biocompatibility.[3],[9] Depth of cure & microhardness testing has been widely used to assess the relative degree of cure of resins. To define depth of cure based on top and bottom hardness measurements, it is common to calculate the ratio of bottom/top hardness & give an arbitrary minimum value for this ratio. It has been suggested that acceptable polymerization of a given composite has occurred when the test specimen’s bottom surface hardness is at least 80% of the top surface hardness.[10],[11]
The current in vitro study evaluated depth of cure (hardness ratio) of two bulk fill resin composites in different thicknesses by Vickers hardness of the top and bottom surface.
Methodology
Depending on the type of composites, there were two groups of 30 samples each. According to the thickness of composite resin each group were further divided into three groups of 10 each.
Group IA (n=10): Tetric N-Ceram with thickness of 3 mm
Group IB (n=10): Tetric N-Ceram with thickness of 4mm
Group IC (n=10): Tetric N-Ceram with thickness of 5mm
Group IIA (n=10): SureFil with thickness of 3 mm
Group IIB (n=10): SureFil with thickness of 4mm
Group IIC (n=10): SureFil with thickness of 5mm
Thirty specimens of each composite were prepared in standardized cylindrical stainless steel molds (10mm x 2mm) with different heights of 3, 4 and 5 mm. The mold was placed on mylar strip supported by glass slide of 1mm thickness. The restorative material was placed in bulk thickness of 3mm, 4mm and 5 mm respectively into the mold with a Teflon coated spatula.
After complete loading of the material in the mold, the material was covered with another transparent mylar strip on top of the mold. A glass slide was placed against the top surface of transparent mylar strip and pressed with light pressure to expel excess material from the mold.
The specimens were polymerized through the 1mm thick glass slide with the quartz halogen light (Spectrum-800, Dentsply) calibrated at 500 mW/cm2 and the intensity was checked with an in-built radiometer before curing each specimen. Curing time was set at 30 seconds and all specimens were light cured from the upper surface.
Distance between light source and specimen was standardized by the use of 1mm thick glass slide and placing the tip of the curing system in contact with the top glass slide.
The samples were removed from the mold and bottom surfaces were marked to distinguish them from top surfaces. After retrieval from the mold, all specimens were stored in a container at 37ºC and 100% relative humidity for 24 hours in an incubator.
Depth of Cure measurement
The depth of cure was measured by evaluating the Vickers hardness on the top and bottom surface of each specimen. The Vickers hardness was determined for each specimen using microhardness tester. A diamond indenter was used to apply a load of 100 gm for 15 seconds. For each sample, three VHN readings were recorded for the irradiated top and non irradiated bottom surfaces. Then for each thickness, the mean value and corresponding standard deviation of the VHN were measured. A bottom to top VH % was determined & a value of 80% was used to indicate acceptable curing.
Statistical Analysis
The results were statistically analyzed using one way ANOVA followed by post hoc (Bonferroni) and t-tests. Mean values and standard deviations of Vickers hardness and depth of cure were calculated for each group of specimens and subjected to statistical analysis using Statistical Package for Social Sciences (SPSS). Paired student t-test was performed to determine the significant differences between the groups (P < 0.05). Post hoc test was done to determine differences within the same group.
Results
Table 1 shows mean values and standard deviations of Vickers hardness and depth of cure for each group of specimens.
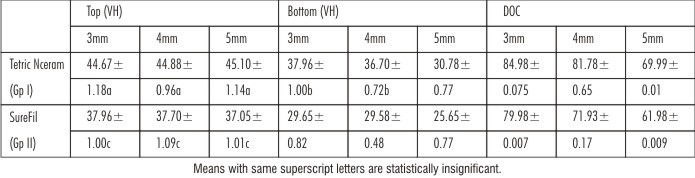 | Table 1: Mean values and standard deviations of Vickers hardness and depth of cure (DOC) for each group of specimens
 |
For both bulk fill material, the top surface hardness values were consistently higher than those of the bottom surface values.
When both bulk fill materials were compared, Tetric N-Ceram showed higher hardness value at both top & bottom surfaces and at all thickness. The difference between both the group was statistically significant (p>0.05).
Both Tetric N-Ceram and Surefil bulk fill material showed different bottom to top surface microhardness ratio and the difference was statistically significant (p>0.000). The bottom to top surface hardness ratio for Tetric N-Ceram at 3mm was 85%, at 4mm was 80% and at 5mm was 70% and for Surefil at 3mm was 80%, at 4mm was 72% and at 5mm was 62%.
When mean value of top surface microhardness of Tetric N-Ceram at different thickness were compared, p value were found to be insignificant (p>1.000). For the bottom surface, the mean hardness value at different thickness was found to be statistically significant (p>0.000) except between IA and IB (p>0.008).
When mean value of top surface microhardness of SureFil at different thickness were compared, p value were found to be insignificant (p>1.000). For the bottom surface, the mean hardness value at all thickness was found to be statistically significant (p>0.000).
Discussion
The degree of polymerization plays an important role in physical & mechanical properties of composite materials.[12]
There are direct & indirect methods for investigating the depth of cure. Infrared spectroscopy & laser raman are direct methods & microhardness, scratching & visual inspection are some of the indirect methods.[12] Direct methods are complex, expensive & time consuming; however, microhardness testing appears to be the most popular method because the other indirect methods tend to over-estimate the curing depth.
The Vickers microhardness test was selected in this study because it is the most accurate available & simple test for measuring the microhardness of a brittle material like composite restorations.[13] The bottom to top hardness ratios ranging from 0.80-0.90 have been used as criteria for the adequate degree of conversion at a specific sample thickness.[10],[14] It means that the bottom to top surface microhardness ratio of 80 % or more is adequate curing.
In our study, top surface hardness values were consistently higher than those of the bottom surface values as a result of adequate polymerization.
Several studies have shown that with the increase in thickness of composite resin, a decrease in depth of cure was observed & this finding is congruent with our study.[10],[15]
Surface microhardness (Vickers or knoop) has been shown to be an indicator of the degree of conversion & correlates well with the infrared spectroscopy.[12] Hardness reflects both the degree of polymerization, the filler size and loading and quality of coupling between filler and polymer. In highly filler loaded composites or materials with rather large prepolymer particles the filler effect on hardness is more pronounced than in composites with low filler loading.
In the present study, Tetric N-Ceram bulk fill when compared with SureFil bulk fill composite showed higher microhardness value in all thicknesses and the difference was statistically significant. This difference could be due to the higher filler loading in Tetric N-Ceram having two types of barium aluminium silicate glass fillers (61%) with average particle size 0.4 and 0.7 um and prepolymer fillers (17%). In comparison to this SureFil has filler loading of 65% with average particle size of about 0.8 um.
In our study, the difference in depth of cure between both bulk fill composite material was affected by composite composition rather than the intensity of light source, distance from curing tips or its shade, as all these factors were standardized.
Tetric N-Ceram consists of Ivocerin as a photoinitiator in addition to the conventionally used initiator systems. Ivocerin is a new initiator that features a high absorption coefficient and is therefore highly effective even if used in only small quantities. Ivocerin allows for increased quantum efficiency and is therefore far more effective than camphorquinone or Lucirin. This enables the material to polymerize faster and, as an additional advantage, increases the depth of cure. Hence, Ivocerin acts as a polymerization booster and is therefore far more effective than conventional initiator systems. Translucency is another factor in depth of curing.[10],[16] Since the refractive index of mixed oxide in Tetric N-Ceram bulk fill is matched to that of the polymer, the degree of translucency is not diminished. Glass particles also have an important role in light transmission.[15] Tetric N-Ceram bulk fill incorporates barium aluminium silicate glass filler & prepolymer filler mixture consisting of monomer glass filler. The presence of glass & its translucency could have caused better depth of cure by Tetric N-Ceram.
The depth of cure decreased with increase in thickness of both the bulk fill composite resin material. The acceptable depth of cure for Tetric N-Ceram was upto 4mm and bottom to top surface microhardness ratio was 80%. Whereas, SureFil showed the acceptable depth of cure upto 3mm and bottom to top surface microhardness ratio was 80 %.
There are no studies done till date contradicting or corroborating the findings of our study.
Further studies needs to be done to find the mechanical properties of newly introduced bulk fill composites and their efficacy in clinical scenario.
Conclusion
Microhardness of Tetric N-Ceram bulk fill on both top & bottom surfaces was significantly higher than SureFil bulk fill composite resin in all thicknesses.
Depth of cure decreased with increase in thickness of both bulk fill composites resin.
The acceptable depth of cure for Tetric N-Ceram was upto 4mm and for SureFil was upto 3mm.
References
1. Price RB, Murphy DG, Dérand T. Light energy transmission through cured resin composite and human dentin. Quintessence Int 2000;31:659–67.
2. Ruyter IE, Oysaed H. Conversion in different depths of ultraviolet and visible light activated composite materials. Acta Odontol Scand 1982;40:179–92.
3. Ferracane JL, Mitchem JC, Condon JR, Todd R. Wear and marginal breakdown of composites with various degrees of cure. J Dent Res 1997;76:1508–16.
4. Poskus LT, Placido E, Cardoso PE. Influence of placement techniques on Vickers and Knoop hardness of class II composite resin restorations. Dent Mater 2004;20:726–32.
5. Sideridou ID, Achilias DS. Elution study of unreacted Bis-GMA, TEGDMA, UDMA, and Bis-EMA from light-cured dental resins and resin composites using HPLC. J Biomed Mater Res B Appl Biomater 2005;74:617–26.
6. Sakaguchi RL, Douglas WH, Peters MC. Curing light performance and polymerization of composite restorative materials. J Dent 1992;20:183–8.
7. Pilo R, Oelgiesser D, Cardash HS. A survey of output intensity and potential for depth of cure among light-curing units in clinical use. J Dent 1999;27:235–41.
8. Yoon TH, Lee YK, Lim BS, Kim CW. Degree of polymerization of resin composites by different light sources. J Oral Rehabil. 2002;29(12):1165- 73.
9. Hinoura K, Akiyama Y, Miyazaki M, Kuroda T, Onose H. Influence of irradiation sequence on dentin bond of resin inlays. Oper Dent. 1995;20(1):30-3.
10. Bouschlicher MR, Rueggeberge FA, Wilson BM. Correlation of bottom to top surface ratios for a variety of resin composite compositions. Oper Dent 2004;29(6):698-704.
11. Moore BK, Platt JA, Borges G, Chu TM, Katsilieri I. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Oper Dent 2008;33:408–12.
12. Aguiar FH, Braceri OA, Lima DA. Effecct of light curing modes and light curing time on the microhardness of a hybrid composite resin. J Contemp Dent Pract 2007;8(6);1-8.
13. ToledaoM, Oserio E, Oseerio R. Microhardness of selected restorative materials. J Prosthet Dent 1999;81:610-15.
14. Dewald JP, Ferracane JL. A comparison of four mode of evaluating depth of cure of light activated composites. J Dent Res 1987;66(3):727-30.
15. Ceballos L, Fuentes MV, Tafalla H, Martinez A, Flores J, Rodriquez J. Curing effectiveness of resin composites at different exposure times using LED and halogen units. Med Oral Patol Oral Cir Bucal 2009;14(1):E51-6, 10).
16. Polydorou O, Manolakis A, Hellwig E, Hahn P. Evaluation of the curing depth of two translucent composite materials using a halogen and two LED curing units. Clin Oral Investig 2008;12(1):45-51.
|