Introduction:
School dental screening has been regularly practiced in many countries as a part of school health programme. The process encompasses a visual examination of children in school setting to identify dental disease and conditions by using simple hand instruments. Those children who are screened with positive findings are informed about their dental needs and referred to the parent dental institution for treatment.[1] School dental screening programs are adopted in many countries under different names, in United Kingdom as National Health Service (education act 1918); in US Dept of Health and Human Services 1996; in Ontario Ministry of Health 1997; New South Wales Health 2001.
The aim of School dental screening is to encourage dental attendance and demand for care and also serves as a means of providing dental health education.[2] School dental screening is regarded to be successful if it helps in health improvement of the children by increased attendance to dental clinics for treatment and thereby reducing dental health inequalities.[3],[4] Questions have been raised about the effectiveness and appropriateness of screening.[5] The World Health Organization also promotes dental screening of school children stating ‘Screening of teeth and mouth enables early detection and timely interventions towards oral diseases and conditions leading to substantial cost savings”. It plays an important role in the planning and provision of school oral health services as well as health services.[6]
About 30% - 40% of the total population in India are children, and dental diseases are widely prevalent.[7] The Public Health Dentistry department, PCDS at Bhopal city, India conducts regular school dental screening programme for most of the schools in Bhopal city. The children are screened by a team of dentists for oral diseases. Yellow referral cards are given to those children who have an unmet need, which has to be bought back to the institution to get the treatment done. The basic treatment is provided free of cost.
This study aimed to evaluate the effectiveness of school dental screening program in terms of increasing attendance of those who have been screened positive and likelihood of getting preventive treatment done after having turned up to the institution for curative care.
Material and methods
School children between the ages of 6-16 years were included in the present study. The data regarding the registered schools of Bhopal city were obtained from the Deputy Director of Public Instructions office. A total of 88 schools, 42 public and 46 private schools come into this jurisdiction. Out of which, 12 schools of similar socio-demographic profile were chosen as they were nearer to the institution. The examiner set the criteria of including nearby schools, within 10 kms radius in order to obtain better response rate as it was easily accessible for children.
A 2 stage simple random sampling technique was employed further to decide the sample. In the first stage, 12 were selected by lottery system, and in the second stage, a random allocation of these schools either into the study group or control group were made of each schools (6 each). The concerned authority of each school was then met to obtain permission to conduct the study. Informed consent from parents was also obtained before the start of the study. The study was conducted in 2 phases. In the first phase, children in the study group were examined for 3 months by a single examiner. Dental diseases were measured using the WHO oral health survey basic methods (1997).[8] The examiner was trained and calibrated for the different range of conditions and diseases. The intra examiner reliability was 0.88.
Children who did not cooperate at the time of examination or parents of children who did not give consent were excluded from the study. After examination, referral cards were given to children who required any dental treatment. A letter to the parents of these children was also enclosed in the almanac informing them about their child’s dental health status. Free dental treatment was promised by the parent institution within the next three months of follow-up on submission of the referral card.
The second phase involved examination of children in the control group to record the unmet treatment needs.
The study group comprised of 1832 children in the study group. The control group comprised of 1899 children. Dental health education with models, charts and power point presentations regarding types of teeth, composition of teeth, importance of oral hygiene, proper oral hygiene practices, common oral diseases and their prevention and treatment was rendered. Referral and attendance rate to the dental institution was calculated from the start of the study to 3 months later. Those of the children who turned up to dental college for the required treatment and those who also seeked preventive care were recorded separately.
Descriptive analyses were performed. Chi-square test was used to test the difference between the parameters, with a level of significance < 0.05 to determine statistical significance.
Results
A total of 3732 children were included in the present study with 1832 in the study group and 1899 in the control group. A total of 2238 males and 1493 females were examined overall. Table 1 shows the distribution of school children according to gender in both the study and control group.
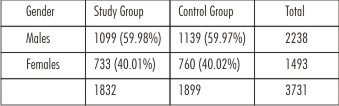 | Table 1 Showing The Overall Distribution Of School Children
 |
The attendance rate for utilizing dental care in the study group was 55.54% and in the control group was 24.97%. Table 2 provides data on children who required treatment in the study and control group and their attendance rate.
 | Table 2
|
40.09% of the children in the study group accepted preventive procedure at the advice of the dentist. Children who attended the dental clinic and also simultaneously obtained preventive care is depicted in Table 3.
 | Table 3 Showing The Children Seeking Preventive Care In Both Groups
|
Discussion
The attendance rate in the present study for the study group was 55.54% and control group was 24.97%, which clearly shows screening was effective in stimulating dental attendance in the study group. These findings are similar to the studies of Mamata etal[2], Donaldson et al[9], Zarod et al[10] and Harding et al[11], but is in contradiction to the studies of K.M. Milson et al[1] and K.M.Milson et al[12].
This utilization rates are not very high in spite of providing free of cost dental treatment. This could be attributed to various reasons - dental care being a low priority in a developing country like India when compared to medical care. Another important factor to be considered is that parents of screened children are under the false assurance that their children have received some kind of an oral examination, which further gets aggravated in the low income and less educated class of people. What they fail to understand is that screening has to be followed by appropriate treatment procedure. Also adding to this are other intangible costs like transportation of the child to the clinic, absenteeism from school, parents having to take off from work to accompany the child, parent’s educational background and apprehension of the child towards the dentist and his team. The quality of the treatment provided is also doubted as it is provided free of cost.
It was found during the course of the study that children of higher ages reported better to the institution. This could be due to the better understanding and comprehension of the older child in conveying the message to his or her parents. Also, that the older child is more independent and may come for treatment without waiting for a parent to accompany him or her.[3],[13] This could also be enhanced as public schools were chosen for the present study. Primary dentition is never considered important in these disadvantaged groups as they have a notion that anyways they are going to fall off. The older child would have developed aesthetic perception and would want to look good amongst his or her peers and hence an increased attendance rate.
It was observed that more number of male children enrolled into schools when compared to their female counterparts. Also, the attendance rate or follow-up of males were slightly more than females. This is not surprising in a country like India, where a male child is more preferred than a female child. Opportunities and chances are generally given more to boys than girls.[14]
40.09% children in the study group and 49.80% in the control group got preventive procedure done. This depicts that screening programme has some motivational force in primary preventive procedures. It becomes the duty of the dentist and his team to educate on preventive methods to the children and accompanying parents to improve oral health. Further research is needed to identify the barriers associated with screened positive children which prevents them from accepting preventive care.
Questions are often raised on the ethical basis of school dental screening programme in improving the oral health of children as no treatment is provided in the school setting. If follow up is not done, then it is incomplete. It is recommended a longitudinal trial to be conducted in schools using elaborate follow up procedures to demonstrate its effectiveness in reducing untreated diseases.
Conclusion:
It was seen that 55.54% of children utilized dental treatment in the study group. Out of which 40.09% received preventive care. Efforts have to be made to stress on the primary prevention of dental diseases at the time of screening and on reporting back at the clinics as they are cost effective. The present method of school dental screening needs amendment. Alternative methods have to be explored to ensure treatment be provided to the needy children and to improve response rate the dental clinics.
References:
1. Milsom K, A.Blinkhorn, H.Worthington, A.Threlfall, K.Buchnan, P.Kearrey-Mitchell and M.Tickle.The effectiveness of school dental screening: A Cluster randomized control trial. J Dent Res 2006;85(10):924-928.
2. Mamata Hebbal, Ramesh Nagarajappa. Does school based dental screening for children increase follow up treatment at dental school clinics. Journal of Dental Education 2005;69(3):382-386.
3. National Screening Committee (1998). First report of the National Screening Committee. Health departments of the United Kingdom.1998. London:HMSO (http://www.nsc.nhs.uk/pdfs/nsc-firstreport.pdf)
4. National Screening Committee(1999). First report of the National Screening Committee. Health departments of the United Kingdom.1999. London:HMSO (http://www.nsc.nhs.uk/pdfs/second report.pdf)
5. Preston ST, Davis GM, Craven R. an investigation of parents attitudes to dental health and school dental screening. Community Dental Health 2001;18:105-109.
6. World Health Organization. Oral health promotion: an essential element of a health promoting school. WHO information series on school health 2003;Document eleven. Geneva: WHO.
7. Damle SG.Pediatric Dentistry:Scope and rationale. In:Damle SG ed. New Delhi:Arya (Medi) Publishing House, 2000:4.
8. Oral health surveys.Basic methods. 4th edition, Geneva:WHO 1997.
9. Donaldson M, Kininons M.The effectiveness of the school dental screening in stimulating dental attendance for children in need of treatment in Northern Ireland. Comm Dent Oral Epidemiol 2001;29:143-149.
10. Zarod BK, Lennen MA.The effect of school dental screening on dental attendance: The results of a randomized controlled trial. Community Dental Health 1992;9:361-368.
11. Harding M, Taylor G.The outcome of school dental screening in 2 suburban districts of greater Manchester, UK. Community Dent Health 1993;10:269-275.
12. K.M.Milson.The effectiveness of school dental screening: dental attendance and treatment of those screened positive. British Dental Journal 2006;200(12):687- 690.
13. Michael D, Mc Cunniff, Daminano PC.The impact of WIC dental screenings and referrals on utilization of dental services among low income children. Pediatr Dent 1998;20:181-187.
14. Ghosh S. Discrimination begins at birth. India Pediatric 1986;23:9-15.
|