Introduction:
The World Health Organization has defined oral leukoplakia as a predominantly white lesion of the oral mucosa that cannot be characterized as any other definable lesion. Leukoplakia usually occurs in adults older than 50 years of age. Prevalence increases rapidly with age, especially for males, and 8% of men older than 70 years of age are affected. Approximately 70% of oral leukoplakia lesions are found on the buccal mucosa, vermilion border of the lower lip, and gingiva. They are less common on the palate, maxillary mucosa, retromolar area, floor of the mouth and tongue[1].
Leukoplakia has been studied for many years and is commonly agreed upon as representing the most common pre-malignant oral mucosal lesion[2]. Leukoplakia most commonly represents a benign keratosis. At the time of identification of leukoplakia, biopsy has revealed dysplasia in 12% - 25% of patients and carcinoma in 3% – 10%. The presence of dysplasia within leukoplakia implies an increased risk of malignant transformation[3],[4].
Recent studies indicate that even with obvious strong carcinogens, there seems to be secondary factors, either external or internal which may have a modifying effect[3].The biochemistry of copper and zinc suggests that these metals may play an important role in carcinogenesis[5].
Hence, the present study was conducted to evaluate the levels of serum copper and zinc in leukoplakia and to investigate the prospective association between serum concentrations of these metals at baseline and in patients with leukoplakia.
Aims and Objectives
To investigate the association between serum concentrations of copper and zinc at baseline and in patients with leukoplakia and to evaluate the hypothesis that serum levels of copper, zinc and copper zinc ratio can be used to assess the risk of malignant transformation of oral leukoplakia. The primary objectives of the study were to estimate the serum levels of copper, zinc and copper zinc ratio in various stages of leukoplakia, to estimate the serum levels of copper, zinc and copper zinc ratio in different study groups, to estimate the serum levels of copper, zinc and copper zinc ratio in different types of leukoplakia, to estimate the serum levels of copper, zinc and copper zinc ratio in different grades of dysplasia.
Subjects and Methods:
Experimental procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975, as revised in 2000.
Experimental Subjects:
Inclusion criteria:
Routine intra oral examination was carried out on all subjects reporting to Hospital, and during soft tissue examination, subjects with well-defined white patch, localized or extensive, that is slightly elevated and that has a fissured, wrinkled, or corrugated surface or a mixed red-and-white lesion in which keratotic white nodules or patches are distributed over an atrophic erythematous background or presence of thick white lesions with papillary surfaces in the oral cavity which is consistent with the diagnosis of leukoplakia was taken for the study.
Control Subjects:
Thirty subjects who were age and sex matched with that of experimental subjects were selected. They were divided into two groups. Group I consisted of thirty subjects who had no intra oral mucosal lesions and Group II thirty subjects who had intra oral mucosal lesions.
Procedure:
A detailed history of the patient and through clinical examination was done and findings were recorded as per the proforma. Fasting blood samples were collected from peripheral veins (Brachial vein) using sterile disposable needles and syringes and then transferred to sterile plastic test tubes in which blood was allowed to clot. Then the samples were centrifuged at 2500 rpm/min for 5 minutes and serum samples, which were obtained, were stored in the refrigerator (5-8°C) until the estimation was done. The serum samples were then subjected to quantitative determination of Copper and Zinc by Inductively Coupled Plasma – Optical Emission Spectrometry.
Under local anesthesia, an incisional biopsy was taken in relation to the lesion which included an area of normal adjacent mucosa and sent for histopathologic examination. The slides were stained with H and E stain to evaluate the presence of dysplastic changes, if any. Classification and staging of oral leukoplakia were determined as per[6],[4].
Micronutrient Analysis Using Inductively Coupled Plasma – Optical Emission Spectrometer
Samples were introduced into the spectrometer at about 10 ml/min by using a peristaltic pump with 0.79 mm (i.d.) manifold tubing and an ISIS autosampler. Emission wave lengths monitored and photomultiplier settings were as follows: Zn, 213.856 nm and 115; Cu, 324.754 nm and 95. After an 80-second delay, the signals were integrated twice for 4 seconds each in the ratio intensity mode for the analyte signal vs. the yttrium internal standard signal. Background correction and spectral overlap correction were not used. The estimation of micronutrients present in the sample was displayed in the computer.
Statistical Methods used in the study:
i. Mean
ii. Chi Square Test
iii. ANOVA
iv. Student Newman Keuls test
Results
Analysis of samples collected in the study as per the methodology described in the above paragraphs yielded the following results:
Serum level of copper was elevated in stage 4 leukoplakia, as compared with stage 1 and stage 2 leukoplakia. Serum level of copper in subjects with leukoplakia was significantly elevated when compared with serum level of normal subjects. Serum level of zinc was elevated in stage 4 leukoplakia when compared with stage 1 and stage 2 lesion. The serum level of zinc was significantly elevated in subjects with leukoplakia when compared with serum levels of zinc in normal subjects. Serum copper zinc ratio was not statistically significant among different stages of leukoplakia. Serum copper zinc ratio was significantly elevated in subjects with leukoplakia when compared with normal subjects (Figure 1).
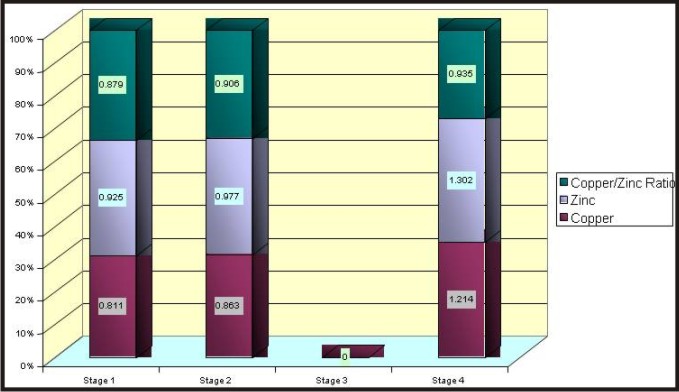 | Different Stages Of Leukoplakia
 |
A serum level of copper was significantly raised in leukoplakia greater than 4 cm in size and it subsequently decreased with decrease in size of the lesion. A similar association was seen when correlating levels of zinc with size of the lesion. In case of copper zinc ratio, there was no statistical significance when correlating with size of the lesion (Figure 2).
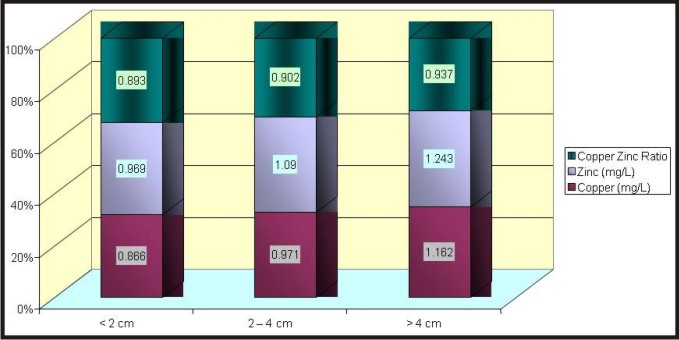 | Different Size Of Leukoplakia
|
The study further revealed that serum level of copper was significantly raised in non homogenous leukoplakias as compared with homogenous leukoplakia. A similar association was seen when correlating level of zinc with type of leukoplakia. In case of copper zinc ratio, there was no statistical significance when correlating with type of the lesion (Figure 3).
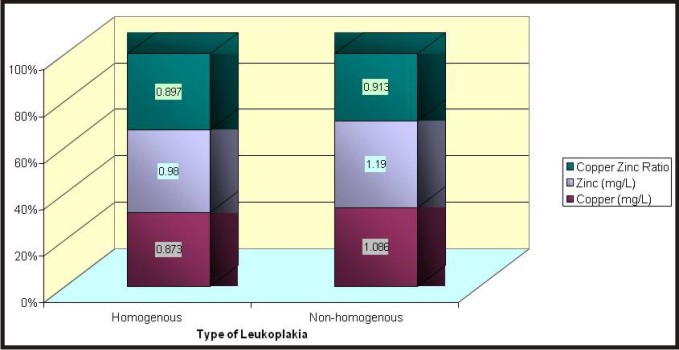 | Different Types Of Leukoplakia
|
Further, the serum level of copper was significantly raised in leukoplakia with moderate dysplasia and it subsequently decreased in mild dysplasia and in lesions with no dysplasia. A similar association was seen when correlating levels of zinc with grade of dysplasia. In case of copper zinc ratio, there was no statistical significance when correlating with grade of dysplasia. (Figure 4).
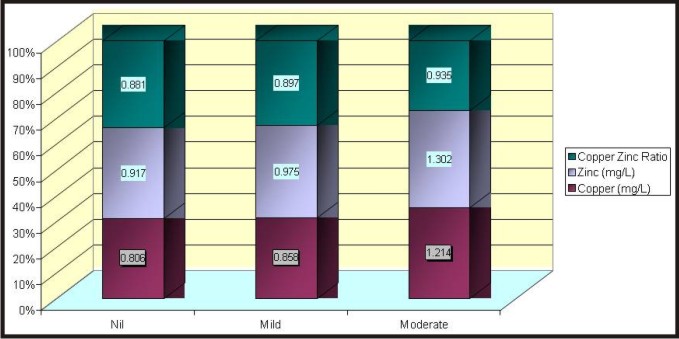 | Different Grades Of Dyaplasia
|
Discussion
In the present study, serum level of copper was elevated in stage 4 leukoplakia, as compared with stage 1 and stage 2 leukoplakia (p value = 0.001). Serum level of copper in subjects with leukoplakia was significantly elevated when compared with serum level of normal subjects (p value = 0.001). The serum level of copper was statistically significant (p value = 0.001). Jayadeep et al[7] in his study has stated that serum copper level was elevated in oral leukoplakia. He has suggested that the raise in serum copper might be due to increased turnover of the ceruloplasmin in the serum of cancer patients and patients with leukoplakia. Ceruloplasmin, a copper carrying globulin with essential oxidase activity is a late acute phase reactant and is synthesized in parenchymatous liver cell. He also pointed out from the earlier studies that elevated level of serum ceruloplasmin was present in chronic smokers, head and neck cancers, Hodgkin and non-Hodgkin lymphoma, carcinoma of lung and gastrointestinal tract. Jha[8], in his study on oral carcinoma, has stated increased serum copper levels (p value = < 0.05). He stated that the increase in serum copper level was related to the stage of the disease. He has also stated that mechanism involved in alteration of serum copper levels in cancer patients was not clear. The raise in serum copper was possibly due to an increase in serum cuproenzyme, ceruloplasmin consequent to decreased catabolism of this enzyme in cancer patients. He stated elevation of serum copper to be a non specific finding and has been found in multiple sclerosis, myocardial infarction, liver disease and schizophrenia. RK Viyas[9], in his study, has stated that concentration of copper was significantly increased (p value = <0.05). M Shifrine[10] had discussed from his study that serum copper was markedly elevated (p value = 0.001) in patients with osteosarcoma. GL Fischer[11] observed increased serum copper levels in patients with osteosarcoma and was positively correlated with the extent and activity of the disease. IlA Shah Reddy[12] has described serum copper level to be a nonspecific but fairly reliable indicator of disease activity in Hodgkin’s disease. He also found serum copper level to be slightly increased in patients with active disease, with a clear separation between those patients in remission and those with active disease in his study. He also stated that the mechanism of serum copper level elevation was not known although it has been shown that 96% of copper in normal serum was bound to the enzyme ceruloplasmin and he has noted in his study that both serum copper level and ceruloplasmin levels were elevated. GB Toke[13] reported that the raise in serum copper was possibly due to increase in serum cuproenzyme, ceruloplasmin consequent to decreased catabolism of this enzyme in cancer patients. He also found elevated levels of serum copper in subjects with myocardial infarction.
In the present study, serum level of zinc was elevated in stage 4 leukoplakia when compared with stage 1 and stage 2 lesion (p value = 0.001). The serum level of zinc in subjects with leukoplakia was significantly elevated when compared with serum levels of zinc in normal subjects (p value = 0.001). However, these findings were not consistent with the study by Jayadeep[7] who has stated in his study that a significant decrease in serum zinc level was reported in patients with leukoplakia and cancer when compared with normal patients. The decreased level of zinc in serum might be due to the increased utilization of zinc by tumor cells. It has also been reported that tobacco smoking may indirectly affect the zinc status because the cadmium present in the tobacco will compete with zinc for intestinal absorption. He suggested that the decrease in zinc levels might be due to the presence of high amount of cadmium in the tobacco. Low serum zinc has also been reported in hepatitis, cirrhosis and myocardial infarction. Reduced serum zinc was also found in oral sub mucous fibrosis. GBToke[13], in his study, has observed an increase in serum zinc in patients with head and neck tumors and he stated that zinc homeostasis was not so well regulated as copper homeostasis, hence zinc levels were non specific. Jha[8] has stated the serum zinc was generally decreased as compared to control group (p<0.05) and that alteration in serum zinc level was related to the stage of the disease. The possible mechanism was not clear and would probably be due to increased metabolic requirement of zinc by cancer cells since the DNA polymerase activity of zinc is particularly important in cell proliferation encountered in growing cell tumor. Infection and tissues damage that are often associated with oral carcinoma also play a significant role in hypozincaemia. R K Vyas[9] described a decrease in concentration of zinc as compared to control group. A decrease in serum zinc may be due to inadequate dietary zinc, anorexia, vomiting or various drugs. In addition, leukocyte endogenous mediator released from leukocytes during inflammation redistributes the body zinc from the serum to liver and may produce a drop in serum zinc. M. Shifrine[10], in his study, has stated that the zinc level was low in patients with metastasis than those with primary tumors only. He also stated that the zinc levels for the tumor free groups were nearly normal and lower but not significantly different than the group with primary tumors only. Ila Shah Reddy[12] has described in his study that no statistically significant changes in the zinc concentration was found in patients with cancer when compared with normal patients.
In the present study, serum copper zinc ratio was not statistically significant among different stages of leukoplakia. Serum copper zinc ratio was significantly elevated in subjects with leukoplakia when compared with normal subjects (p value = 0.001). This was in concordance with the study done by A. Jayadeep[7] in which he showed that copper zinc ratio was elevated in oral leukoplakia. Jha[8] described in his study that serum copper zinc ratio showed a significant elevation in patients with oral carcinoma when compared with healthy controls and its value increased significantly with advancing stage of the disease (p<0.05).GL Fisher[11] described in his study that serum copper zinc ratio was found to be significant in patients with osteosarcoma when compared with normal patients. GBToke[13] suggested that since zinc homeostasis was not well regulated as copper homeostasis, the copper zinc ratio can be considered as a more reliable index of the status of these elements in cancer of digestive tract.
In the present study, the serum level of copper was significantly raised in leukoplakia greater than 4 cm in size and it subsequently decreased with decrease in size of the lesion. (p value = 0.013). A similar association was seen when correlating levels of zinc with size of the lesion. (p value = 0.019). In case of copper zinc ratio, there was no statistical significance (p value = 0.410) when correlating with size of the lesion. These findings have not been reported in the literature.
Conclusion
Through this study, we were able to come to a conclusion that during the pathogenesis of oral leukoplakia, the level of serum copper and zinc was elevated in different stages of leukoplakia. The serum copper, zinc and copper zinc ratio was also elevated in subjects with leukoplakia when compared with normal subjects with and without habits. However, the exact mechanism for these changes to occur remains unclear. Although the degree of dysplasia has significance in assessing the malignant transformation potential, patients with mild dysplasia or even without evidence of dysplasia are at risk for malignant transformation. Intraexaminer reproducible agreements in diagnosis of dysplasia are also difficult to achieve. Therefore, the development of biologic markers becomes extremely important in diagnosis, prognosis and treatment parameters. Thus, estimation of serum levels of copper, zinc and copper zinc ratio has a diagnostic value in assessing the extent and prognosis of the disease. To confirm the involvement of these factors in oral carcinogenesis, a study on a large sample size with rigorous follow-up over extended periods is essential. Since the presence of elevated levels of serum copper, zinc and copper zinc ratio implies a higher risk of malignant transformation, we as dental professionals should identify and treat leukoplakia and take adequate measures to counsel and educate the patient about the ill effects of smoking and alcohol consumption.
Reference
1. Indraneel Bhattacharyya, Donald M. Cohen, Sol Silverman JR. Red and white lesions of the oral mucosa. Burket’s Oral Medicine - Diagnosis and Treatment. 10th ed. Elsevier Science; 2003. 85, 101-5.
2. Richard N. Kniseley, Velmer A. Fassel, Constance C. Butter. Application of industrial coupled plasma excitation sources to the determination of trace elements in microliter volumes of biological fluids. Clinical Chemistry 1973; 19(8): 807-812.
3. James J. Sciubba. Oral cancer and its detection: History-taking and the diagnostic phase of management. J. Am Dent Assoc 2001; 132: 12s-18s.
4. Lenore Kohlmeier, Niel Simonsen, Kathleen Mottus. Environmental health issues. Environmental Health Perspectives Supplements 1995; 103: s8.
5. Tiejian WU, Christopher T. Sempos, Freudenheim, Paula Muti, Ellen Smit. Serum iron, copper and zinc concentrations and risk of cancer mortality in US adults. Ann Epidemiol 2004; 14: 195-201.
6. Axell T, Pindborg JJ, Smith CJ, Van Der Waal I. Oral white lesions with special reference to precancerous and tobacco related lesions: conclusions of an international symposium held in Uppsala, Sweden May 18-21, 1994. J Oral Pathol Med. 1996; 25: 49 –54.
7. Jayadeep A.K., Raveendran Pillai, Kannan S, Nalanikumar K.R., Babu Mathew, Krishnan Naiar et al. Serum levels of copper, zinc, iron and ceruloplasmin in oral leukoplakia and squamous cell carcinoma; Journal of experimental clinical cancer research 1997; 16(3): 295-300.
8. Jha I.N., Singh H.B. Narendra Prasad. Serum copper / zinc ratio in oral carcinoma. Indian Journal of Medical Research. 1985; 81: 602- 6.
9. Vyas RK, Gupta AP, Abha Gupta and Aeron AK. Serum Copper, Zinc, magnesium and calcium levels in various human diseases. Indian Journal of Medical Research. 1982; 76: 301-4.
10. Shifrine M, Fisher GL. Ceruloplasmin levels in sera from human patients with osteosarcoma. Cancer. 1976; 38:244-8.
11. Fisher GL, Byers VS, Shifrine M, Levin AS. Copper and zinc levels in serum from human patients with sarcomas. Cancer. 1976; 37: 356-63.
12. Ila Shah Reddy, Prem kilanani and Carter R. Bishop. Serum copper levels in non-hodgkin’s lymphoma. Cancer. 1980; 45: 2156-9.
13. Toke GB and Dhamne BK. A study of serum copper, serum zinc and copper / zinc ratio as a diagnostic and prognostic index in case of head, neck and face tumors. Indian Journal of Pathology and Microbiology. 1990; 33(2):171-4.
|