Introduction
An unexpected loss of anterior tooth is an appalling event for the patient having a comprehensive blow on the psychology as well as the overall personality of the individual.[1] Tooth avulsion or exarticulation is the loss of tooth following trauma.[2] “When the tooth is removed from its socket, consequence of a trauma, and the surrounding structures as periodontal ligament and neurovascular bundle injure, the situation is named as tooth avulsion.”(World Health Organization’s classification system modified by Andreasen).[3]
There has been an increase in the occurrence of avulsion due to increase in road traffic accidents, followed by fall and sport injuries.[4] Most susceptible group is children between 7-14 years[5] as the alveolar bone is resilient conferring minimal resistance to extrusive forces.[6]
It is well established that the clinical prognosis of an avulsed tooth/teeth depends upon the promptness and immediate management by dental practitioner.[7] The success rate of reimplanted teeth is reported to be very low, which is 4 to 50 %.[8] However, immediate reimplantation is not always possible due lack of knowledge from parents/tutors at the moment of accident[9], person’s conscious state, informed consent issues, and lack of confidence in strangers gathered at site of accident.[10] If managed pertinently the avulsed tooth with viable periodontal ligament when reimplanted can maintain functionality for some years.[11] This overview expounds the aspects for the clinical success and prognosis of exarticulated teeth in dental practice.
Factors affecting success rate of replanted teeth:
Age : Progression of root resorption in teeth with extended extra-oral periods is age related. In patients 8-16 years old at the time of avulsion, the rate of resorption is higher compared to 17-39 years old patients.[12] Since most avulsions occur before the patient’s facial growth is complete, it is critical to maintain the tooth and surrounding bone until facial growth is complete and a relatively uncomplicated permanent restoration can be made.[5]
Mechanical damage during replantation:
In the processes of avulsion and replantation, maximal damage occurs to the convex buccal and lingual root surfaces, where physical contact occurs with the bone socket during rotary movement.[6]
Timing of pulp extirpation:
Timing of pulp extirpation (PE) of a replanted avulsed tooth depends on tooth maturity and, if immature, the extraoral time. Unless the tooth is immature and has been replanted almost immediately, PE is generally recommended within 7 to 14 days13-17 or 10 days post-replantation.[13] Extra-alveolar duration: Extra-oral dry storage for more than 60 minutes subjects the success rate of replanted tooth to a minimal[18] leading to tooth loss.[19] Teeth that are replanted within 5 minutes after avulsion have best prognosis.[20] Damage to PDL by dehydration & direct mechanical trauma affects the viability of cells, worsening the prognosis of replanted tooth[21] with the probability of resorption increasing by 29% for every additional 10 minutes of dryness.[22]
Storage media:
An extra-alveolar time always exists before the patient arrives at the dental office leading to desiccation of the root surface, increasing the risk of loss in vitality of the PDL cells.[6] As dry storage is detrimental to the PDL viability, the avulsed tooth must be prevented from drying by use of storage media of appropriate pH, osmolality & efficacy. (Table 1) Tap water, saline, saliva and Gatorade[9] are inappropriate storage media due to their non-physiological pH & osmolality.[23] Milk and HBSS have the best results using the multiparametric assay, corroborating their use in cases of tooth avulsion.[9] Coconut water[24], green tea extract[25] & ricetral[2] are comparable to HBSS and milk in maintaining PDL viability. Propolis, a recent development is an appropriate medium for avulsed tooth and can maintain the viability upto 6 hours.[6] (Table 2)
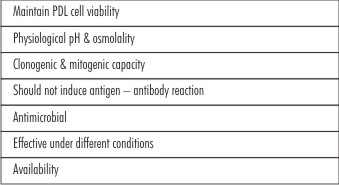 | Table 1 : Ideal Properties Of Storage Media
 |
 | Table 2 : Different Storage Media
|
Splinting - type and duration:
semi-rigid or flexible fixation permits physiological jiggling movements of the teeth as functional stimuli which assists PDL healing. As compared to previous recommendations of 6 weeks (essentials of traumatic injury) splinting for up to 2 weeks & splintitng for 1 week may be adequate for periodontal healing.[26] (Table 3) Recent guidelines recommend splinting for up to 2 weeks when extraoral dry time is less than 60 min, and for 4 weeks for both immature and mature teeth when extraoral dry times exceed 60 min.[26]
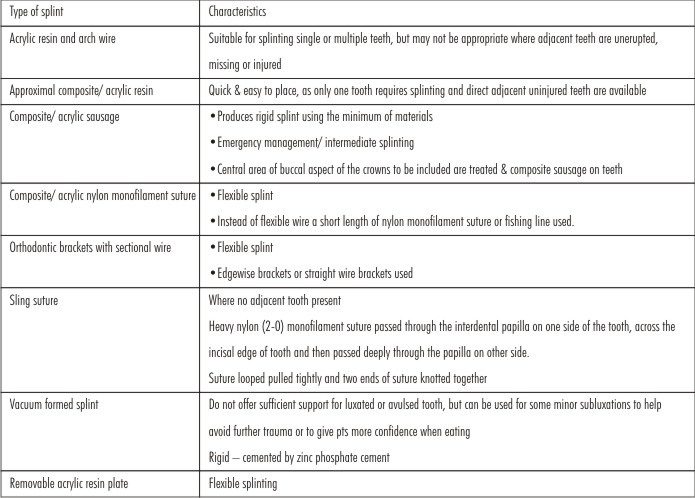 | Table 3 : Splints For Avulsed Teeth
|
The splint should be replaced if undue mobility persists after 10 days.[13] The active term of splinting in dentistry is defined as the joining of two or more teeth into a rigid unit by means of fixed or removable restorations or devices.[27] Splints may be classified as temporary, provisional, or permanent and may be either fixed or removable. (Table 4) Treatment modalities of avulsed teeth Reimplantation refers to the insertion and temporary fixation of completely or partially avulsed teeth that have resulted from traumatic injury. In reimplantation complete reestablishment of vitality of periodontal fibers is the prime objective. The percentage of success of tooth reimplantation has been observed to be low, ranging from 4 to 50%.[28]
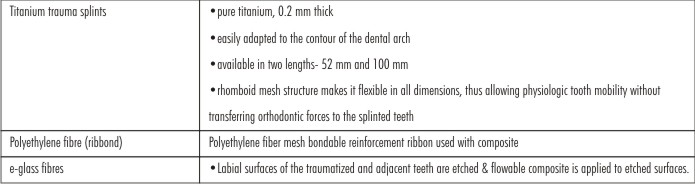 | Table 4 : Splints For Avulsed Teeth (Contd.)
|
Management:
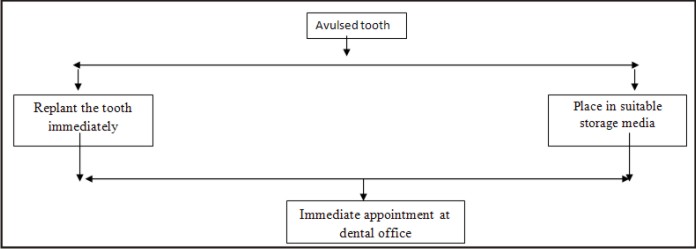
1. At the site of accident (Figure 1, 2)
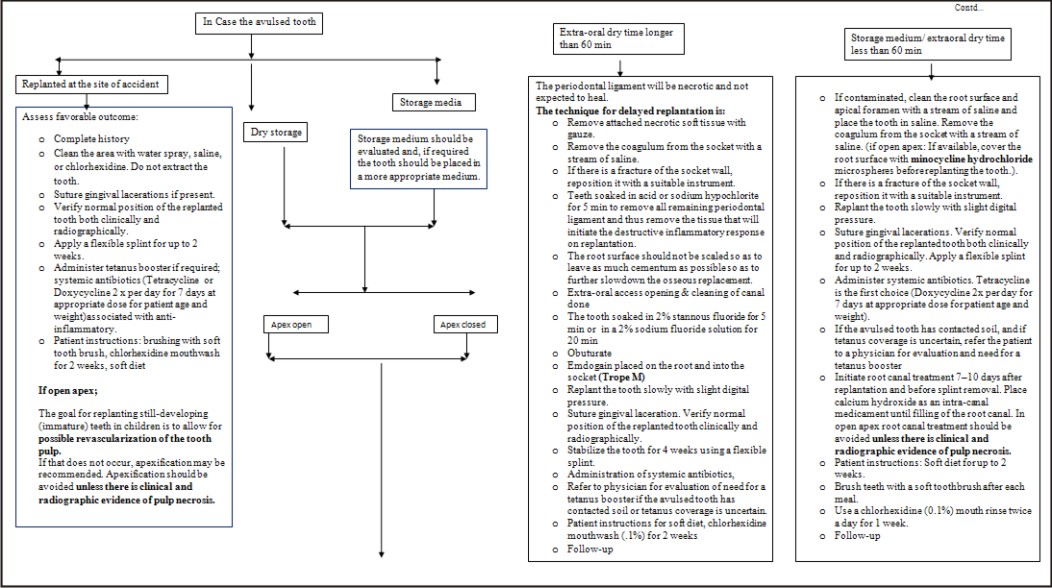
2. Management at dental office (Figure 3)
3. Follow up (every 2 weeks)
• Check for pain, discomfort, swelling
• Take radiographs
• Remove splint
• Check for excessive mobility
• If teeth demonstrate considerable mobility – patient should be warned to be careful with eating etc At this point of treatment, if the tooth/teeth are completely symptomless and there is no radiographic evidence of any pathology, such as external or internal resorption, etc. an appointment can be made to carry out a final RCT. If the apices of the affected tooth are open, the usual procedures to achieve a hard tissue barrier are carried out Some authors prefer to treat the teeth with calcium hydroxide for at least 9-12 months before the final root canal filling is placed.[29]
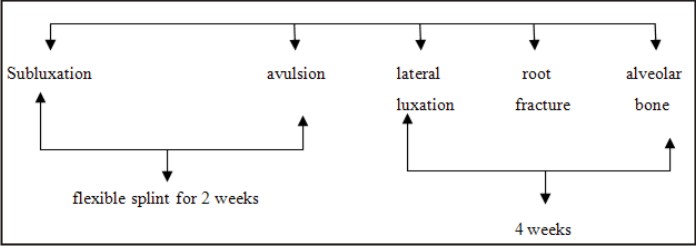 | Fig:1 Duration of splints
|
 | Fig:2 Management at site of accident
|
 | Fig 3: Management of avulsed tooth when at dental office in different circumstances
|
Conclusion
Dental practitioner will occasionally face the task of replantation of avulsed teeth & need to be aware of newer developments to maximize the success of the procedure. Search for what to do when such an emergency emerges in a clinic is utmost importance. The successful long-term survival of replanted teeth is very satisfying for the dental practitioner and generates goodwill in the community.
References:
1. Bodh M, Namdev R, Jain M, Dutta S. A Conservative And Biological Approach For Rehabilitation Of Anterior Edentulous Space Using Natural Tooth Pontic (Ntp) And Fibre Reinforced Composite – A Case Report. Indian J Dent Scien. October 2014;4(6):35-37
2. Rajendran P, Nettiyat OOmmen Varghese, Varughese JM, Murugaian E.Evaluation, using extracted human teeth, of Ricetral as a storage medium for avulsions – an in vitro study. Dent Traumatol 2011; 27: 217–220
3. Glendor U, Halling A, Andersson L, Eilert-Petersson E. Incidence of traumatic tooth injuries in children and adolescents in the county of Vastmanland, Sweden. Swed Dent J 1996;20:15–28
4. Adil NF, Ahmed SS, Jindal MK, Arshad SH. Delayed replantation of avulsed teeth. J Indian Soc Pedod Prevent Dent 2007;(s):s17-19
5. Trope M. Avulsion of permanent teeth: theory to practice. Dent Traumatol 2011 Aug;27(4):281-94.
6. Malhotra N. Current developments in interim transport (storage) media in dentistry: an update. Br Dent J 2011;211(1):29-33.
7. Kargul B, Welbury R. An audit of the time to initial treatment in avulsion injuries. Dent Traumatol. 2009 Feb;25(1):123-5.
8. Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors. Factors related to periodontal ligament healing. Endod Dent Traumatol 1995; 11:76-89.
9. Silva EJ, Rollemberg CB, de Souza Coutinho-Filho T, Zaia AA. A multiparametric assay to compare the cytotoxicity of soy milk with different storage media. Dent Traumatol 2013;29(4):319-22.
10. Andreasen FM, Andreasen JO. Textbook and color atlas of traumatic injuries to the teeth, 3rd ed. Copenhagen: Munksgard, 1994:383-425.
11. Jovanovska M. Delayed tooth replantation after traumatic avulsion. Stomatološki vjesnik 2014;3 (1)
12. Petrovic B, Marković D, Peric T, Blagojevic D. Factors related to treatment and outcomes of avulsed teeth. Dent Traumatol 2010 Feb;26(1):52-9.
13. Gregg TA, Boyd DH. UK National Clinical Guidelines in Paediatric Dentistry. Treatment of avulsed permanent teeth in children. Int J Paed Dent 1998;8:75–81.
14. Flores MT, Andreasen JO, Bakland LK. Guidelines for the evaluation and management of traumatic dental injuries. Dent Traumatol 2001;17:193–6.
15. Trope M. Clinical management of the avulsed tooth. Present strategies and future directions. Dental Traumatol 2002;18:1–11
16. Ram D, Cohenca N. Therapeutic protocols for avulsed permanent teeth: review and clinical update. Pediatr Dent 2004;26:251–5.
17. Flores MT, Andersson L, Andreasen JO, Bakland LK, Malm- gren B, Barnett F et al. Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teeth. Dent Traumatol 2007;23:130–6.
18. Curzon MEJ, Duggal MS, Fayle SA, Toumba KJ. Handbook of dental trauma: a practical guide to the treatment of trauma to the teeth. Oxford: Wright, 1999:p80-98.
19. Veloso HHP, Sampaio FC, Guedes OA. Interdisciplinary treatment of an avulsed permanent tooth in patient with incomplete facial growth. Dental Press Endod 2011 Oct-Dec;1(3):65-70.
20. Munavalli A N, Sachhi R J, Kambale S S, Bandekar S D. Maintaining vitality of immediately reimplanted avulsed tooth: Two-year follow-up case report. J Indian Soc Pedod Prev Dent 2013;31:113-7
21. Bryson EC, Levin L, Banchs F, Trope M. Effect of minocycline on healing of replanted dog teeth after extended dry times. Dent Traumatol 2003;19:90-5.
22. Khalilak Z, Shikholislami M, Mohajeri L. Delayed Tooth Replantation after Traumatic Avulsion: A Case Report Iran Endod J 2008 Summer; 3(3): 86–89.
23. Bazmi BA, Singh AK, Kar S, Mubtasum H. Storage media for avulsed tooth- A review. Indian J Multidiscip Dent 2013;3:741-749
24. Moreira-Neto JJ, Gondim JO, Raddi MS, Pansani CA. Viability of human fibroblasts in coconut water as a storage medium. Int Endod J 2009 Sep;42(9):827-30.
25. Ghasempour M, Moghadamnia AA, Abedian Z, Amir MP, Feizi F, Gharekhani S. In vitro viability of human periodontal ligament cells in green tea extract. J Conserv Dent 2015 Jan-Feb; 18(1): 47–50.
26. Hinckfuss SE, Messer LB. Splinting duration and periodontal outcomes for replanted avulsed teeth: a systematic review. Dent Traumatol 2009 Apr;25(2):150-7.
27. Ansari I, Maria R, Virang B, Parverkar P. Splinting : A Review NJDSR 2014;2(1)
28. Mittal N, Swain G.Management of traumatically avulsed tooth by reimplantation. Guident 2014
29. Andreason JO, Andreason FM. Essentials of Traumatic Injuries to the Teeth: A Step-by-Step Treatment Guide, Second Edition. 2nd ed. Munksgaard: Wiley, 2008:p113-132.
|