INTRODUCTION
Bio-aerosols are airborne particles that are living (bacteria, viruses and fungi) or originate from living organisms. Bio- aerosols are ubiquitous, highly variable, complex, natural or man –made in origin. The sampling and analysis of airborne microorganisms has received attention in recent years due to concerns with mould contamination in indoor environments the threat of bioterrorism and the occurrence of associated health effects, including infectious diseases, acute toxic effects, allergies and cancer [1-3]. Bioaerosols contribute to about 5-34% of indoor air pollution [4,5]. Bacterial cells and cellular fragments, fungal spores and by-products of microbial metabolism, present as particulate, liquid or volatile organic compounds may be components of bio-aerosols.[6] air, contains significant number of microorganisms, acting as a medium for their transmission or dispersal. Inhalation, ingestion and dermal contact are the routes of human exposure to airborne microorganisms, inhalation being the predominant. The particles in a bio- aerosol are generally 0.3 to 100 u m in diameter; however, the respirable size fraction of 1 to 10 u m is of primary concern. [7] bio-aerosols ranging in size from 1.o to 5.0 u m generally remain in the air, whereas larger particles are deposited on surfaces[8]. Exposure to bio-aerosols unlike exposure to chemicals do not gave threshold limits to assess health impact/ toxic effects, due to the
complexity in their entity, variations in human response to their exposure and difficulties in recovering microorganisms that can pose hazard during routine sampling. [9] While their role in various industrial settings has been well studied,
[1] the role of these airborne microorganisms in healthcare settings is poorly understood. Increasing incidences of nosocomial and occupational diseases due to bio-aerosol exposure [10-13] indicate the need for a thorough knowledge in this respect.Bio-aerosols in dental clinics are produced by airoter, scalars, three ways syringe, air polisher and suction, which are mixer of saliva In this article, an overview of bioaerosols, their sources and possible health effects,
various sampling methods and a characterization of common airborne agents is presented.
Factors influencing bio-aerosols
The transport and the ultimate setting of a bio aerosol are affected by its physical properties and the environmental parameters that it encounters. [14] The physical characteristics are size, density, and shape of droplets or particles, the
environmental factors include magnitude of a relative humidity and temperature, which determine the capacity to be airborne. [14] Bioaerosols generated from suspensions undergo desiccation, whereas those generated as dusts or
powders partially rehydrate.[15] The presencemoulds indicated a problem with water penetration or high humidity. [16]
Sources of Bio-aerosols in Indoor and Outdoor Environments
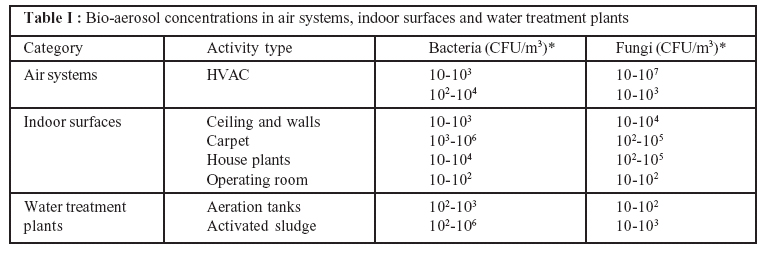
Bio-aerosols originate from any natural or man-made surface and each source gives rise to an entirely unique assemblage of bio-aerosols. Bioaerosols concentrations in air systems, indoor surfaces and water treatment are highlighted in Table I. [17] Deterioration of building materials, offensive odour and adverse human health effects
are associated with microbial contamination of indoor environments.Buildings
The presence of undesirable bio-aerosols is often associated with sick building syndrome (SBS) and building related illnesses (RBI). Sources include furnishings and building materials; fungal contamination within wall, ceiling, and floor
cavities by movement of cells, spores and cell fragments via wall openings and gaps at structural joints. [17] Lack of fresh air due to increased insulation of buildings, poorly maintained or operated ventilation systems, poorly regulated
temperature and relative humidity levels contribute
 |
 |
to the presence and multiplication of bio-aerosols. [18] In developing countries, inadequacies in the buildings, design and improper ventilation may contribute to poor indoor air quality. Healthcare Facilities The microbial load in dental indoor air is highly influenced by the number of occupants, their activity and the ventilation. [19] Occupants are a potential source of microoganisms as they shed the microoganisms from the skin squames and the respiratory. Ventilation causes dilution thus reducing the microbial load. Sinks, wash-basins and drains, nebulisers, humidifiers, and cooling
towers are the potential sources of gram negative bacilli, which colonise on the moist surfaces. Dressings and bedding also can be the sources of airborne microorgaisms. [19] Sweeping of floors and changing of bed linens also can cause suspension of bio-aerosols in air. [19] Fungal spores gain entry into the hospital buildings through ventilation ducts with inadequate filtration. Since exposure levels are high, this may be an issue in the immunocompromised patients.
Modes of Transmission
Bio-aerosols can be transmitted either at long distance beyondthe patient room environment, or withing short distance. Small particle aerosols (e.g., generated during endotracheal intubation) are transmitted to persons in the immediate area near the patient. Virsues like Severe Acute Respiratory Syndrome (SARS), influenza and norovirus are transmitted from patients primarily by contact and/or droplet routes, while airborne transmission occurs over a limited distance. [20]
Legionella may be derived from the environment, [21] others include contaminated food, water, medications (e.g. intravenous fluids) or through vectors. [22] Aspergillus spp. Can be transmitted from patients or the environment. [22, 23]
Obligate airborne pathogens produce an infection that, under natural conditions, is initiated only through aerosols deposited in the distal lung tissue such as Mycobacterium tuberculosis, preferential airborne pathogen can naturally
initiate infection through multiple routes but are predominantly transmitted by aerosols deposited in distal airways, e.g., measles virus and variola (smallpos) virus, opportunistic airborne pathogens naturally cause disease also initiate infection through the distal lung and may use fine-particle aerosols as and efficient means of propagating in favourable environments. Individuals are exposed to an array of bioaerosols in a single day that may interact in complex ways to cause airway inflammation and infection. Smaller cells and spores become trapped within lung tissue and are not easily expelled posing greater health risks. [24] The clinical expression of airway disease is influence by a combination of components of bioaerosols and the dose and duration exposure (environment), as well as intrinsic differences in the host response to bio- aerosols (genetic polymorphisms). [25] Many of the components of bio-aerosols are pathogen-associated molecular
patterns (PAMPs) that bind specific recognition molecules and activate innate immune pathways. The most frequently detected PAMPs in bioaerosols are endotoxin, peptidoglycan and â-(1 3) –glucans. [26] Health Effects Biological hazards to man arise from exposure to high concentrations or unfamiliar form of bioaerosols and three major groups of diseases
associated with bio-aerosol exposure are infectious diseases, respiratory diseases and cancer. [1] Current knowledge is unclear regarding risk to cancer whether these excess risks occur from exposures to biological agents or are due to
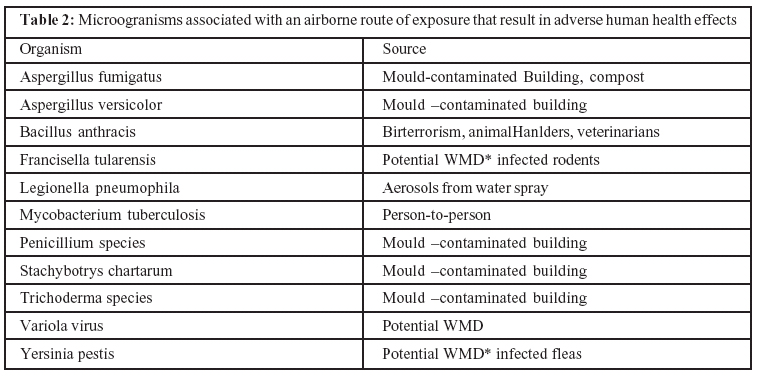
[16] various chemicals used in these industries. [2] Table 2 highlights the microorganisms associated with an airborne route of exposure that result in adverse human health effects. [3] Infectious Diseases Infectious diseases arise from viruses, bacteria, fungi, protozoa and helminthes and involve the transmission of an infectious agent from a reservoir to a susceptible host through airborne transmission. Bacterial diseases Various bacterial diseases such as legionellosis and tuberculosis are linked to cause significant public health concern due to their low infectious dose. [4]
 |
|
Tuberculosis: The transmission of tubercle bacilli occurs through the inhalation of aerosolized bacilli in droplet nuclei of
expectorated sputum-positive tuberculosis patients during coughing, sneezing and taking.
Anthrax: The transmission occurs due to inhalation of the spores of Bacillus and outbreaks are often linked to bioterrorism that are spread through intentionally contaminated mail, apart from occupational exposures.
Illness due to endotoxins: Endotoxins are thelipopolysaccharides (toxins )of gram negative bacterial cell wall these are potent pyrogens, capable of causing fever in very low concentration. 43 High exposure to endotoxins is often associated with nausea and diarrhea .
Fungal diseases
Airborne fungi causing respiratory infection and allergic reaction include Paecilomyces, Mucor and Cladosporium . Symptoms include persistent cold, watering eyes, prolonged muscle cramps and joint pain etc. Illness due to to mycotoxin are absorbed by the intestinal lining, airways and skin; toxic effects follow exposure to toxins on the surface of the mould spores.
Viral diseases
Viruses are readily transmitted by airborne route, and include SARS virus, enteric viruses of intestinal origin produced at sewage treatment facilities, RSV, Hantavirus from rodent faeces,varicella –zoster virus, measles, mumps and rubella viruses.
Diseases caused by parasites and actinomycetes
Free –living amoebae like Acanthamoeba and Naegleria fowleri get aerosolized from natural and artificially heated waters, and cause repiratory
illness and meningoencephalitis. Actinomycetes such as Streptomyces and alge cause allegry, inflammatory reaction and hypersensitivity pneumonits
Respiratory Diseases
Many of the BRI are respiratory diseases and include asthma, hypersensitivity pneumonitis and multiple chemical sensitivity studied respiratory diseases associated with bio-aerosol exposure. Hypersensitivity pneumonitis or extrinsic allergic alveoli’s (EAA) is an inflammatory airways disease caused by an unusual immune response to antigens like fungi (Farmer’s lung ), bird excreta (pigeon breeder’s disease ), and microbial containments in grain dust . Organic Dust toxic Syndrome (ODTS) within hours of a high dose inhalation of endotoxin, fungal spores and mycotoxins which may lead to chronic obstructive pulmonary disease (COPD). Cancer Established biological occupational carcinogens are the mycotoxins .Aflatoxin fromAspergillus flavaus is capble of causing liver canser. [65-66] while Ochratoxin A is a possible human carcinogen. Exposure to aflatoxin and ochratoxin occurs by ingestion, but can also occur by inhalation in industries such as peanut.
Role of Bio –aerosols in Dental care Setting
Dental clinics are a high risk area for both patients and staffs; air –quality management are ensured to be free of airborne infection agents. Adequate air changes and installation of filtration equipment are a necessity; proper air–conditioning systems can significantly reduce airborne
concentrations of fungi during surgery. When the levels of airborne bacteria are reduce in operating rooms (OR), contamination of wounds of wounds is substantially reduced.
Bio–aerosol Evaluation
The purpose of bio-aerosol sampling is to verify their presence in air and in most cases no single sampling method can collect, identify andquantify all of the bio-aerosol components existing in a particular environment. When sampling in indicated it is advisable to sample before, during, and after the sampling area is occupied, including times when the heating, ventilating, and air conditioning system is activated and inactivated. Dental clinic represent a unique ssemblage of indoor microflora as bio-aerosol in indoor air, which may be a source of nosocomial infection. In order to evaluate the quality of indoor air in hospitals, passive and active sampling methods can be used. Wherever higher concentration of
bacteria and fungi are found, active sampling techniques like filter and impinger methods can be used in addition to passive sampling to determine the concentrations and composition of bio-aerosols. Areas such as ICUs, OTs and Oral
Surgery wards where indoor air qualities are of concern can be targeted. The choice of the sampling method in terms of air flow rate and the duration of sampling, is based upon the extent of the loads of bio-aerosols, however there are no
internationally accepted recommendation on sampling flow rate and media used for sampling. Most bio-aerosols sampling devices involve techniques that separate particles from the air stream and collect them in or on a pre-selected
medium. Some of these are:-
(1) Environmental Sampling for Bio-aerosol
(2) Gravitation or setting method
(3) Impingement method
(4) Filtration method
(5) Surface sampling
Analysis for Detection of Microorganisms and Microbial Constituents
Detections of Microorganisms Viable microorganisms include culture and non-culturable. During sampling, only culturable microorganisms are enumerated and identified, leading to an underestimation of bio-aerosol concertations. Therefore estimation of both culturable and non culturable organisms using appropriate microscopy to identify bacteria and fungi(using gram staining for bacteria and lactophenol cotton blue and calcofluor white for fungi) and classical microbiology techniques such as observation of growth characteristics, cellular or spore morphology, and biochemical tests for identification is essential. After sample collection, colonies of bacteria and fungi are grown on culture media at a defined temperature over a 3 -7 day period and then identified. Detection of microbial constituents Endotoxin assay: Samples are collected from air by filter method, using polycarbonate capillary pore membrane filters. After sampling, it is
extracted by sonication and then analysed for the presence of endotoxins by limulus amebocyte.
Data Interpretation for Bio-aerosols
Threshold limit values (TLV) for bio-aerosols are referred to air concentrations of substances under conditions to which people are repeatedly exposed day after day without adverse health effects. There are no established guidelines
specifying the threshold limit values for interpreting environmental measurements of bioaerosols because bio-aerosols do not comprise of single entity. Human response to bio – aerosols range from innocuous effects to serious diseases
depending on the exposure and the susceptibility of human beings to it ( e. g., genetic factors, age personal habits medication). Also, little is known about the minimum dose needed to pose a hazard. While there are no internationally accepted guidelines. Recommendations have been made by World Health Organization (Indoor air quality: Biological contaminants), Federal-Provincial Advisory Committee on Environmental and Occupastional Health, Canada (Indoor Air Quality in Office Buildings: A Technicasl Guide) and NASA standard NhB540.2. Though ACGIH (American Conference of
Governmental Industrial Hygienists) hadpublished numerical guidelines earlier, it currently does not support any existing numerical criteria for interpreting data on biological agents from source or air samples in non-manufacturing
environments. Control Measures for Reducing Bio-aerosols In order to reduce bio-aerosol loads in indoor environments, certain control measures can be followed. These include, proper identification and elimination of the microbial source in occupational and house-hold settings, maintenance of equipment, humidity control, natural ventilation, use of filters in ventilation, and air cleaning by the use of disinfectants and biocides. Periodicaluse of disinfectants and biocides is one of the methods to ensure controlled bio-aerosol concentrations. Air in the operating rooms and other critical areas like isolations rooms can be disinfected by fumigation using various microbicidal agents. Bacillocid is the most commonly used commercially available surface and environment disinfectant that has very good cleansing property along with bactericidal, eridical, sporicidal and fungicidal activity. It is either sprayed or mopped liberally allowing as contact time of 30 minutes and provides complete asep0sis within 30 – 60 minutes. It does not require cleaning with detergent or carbolic acid or formalinfumigation. It does not require shutdown of the disinfected areas such as operating rooms for 24 hours.
CONCLUSIONS
In the context of healthcare settings, bioaerosols can cause occupational hazards and nosocomial infection. Modern built environmentcan be a potential source of bio-aerosols. Bioaerosols monitoring in hospitals can be used for
tracking of nosocomial infections, (HAI). This will also serve as a tool to measure biosafety while handling biohazard us materials. The complexity of these bio-aerosols requires a multisciplinary approach. There is heightened awareness
regarding the study of bio-aerosols and its impact on human health and quality of indoor air and environment in the West. In the context of as developing country, there is a need for increased awareness for targeted surveillance for infection control.
REFERENCES
1. Douwes J, Thorne P, Pearce N, heederik D. Bio-aerosols Health Effects and Exposure Assessment: Progress and
Prospects. Ann occup Hyg 2003; 47:187-200.
2. O’Riordan TG, Smaldone GC. Respiratory medical societies and the threat of bioterrorism. Thorax 2004; 59:265-67.
3. Stetzenbach LD, Butter MP, Cruz P. Detection and enumeration of airborne biocontaminants. Curr Opin Biotechnol 2004;15:170-4.
4. Available at: http://www.pollutionisses.com/ Ho-Li/Indoor- Air-pollution.html. Accessed November 10, 2006.
5. Available at: http://www.airqualitydirect. com . /bio –aerosols htm . accessed September 02,2007
6. Stezenbach ld . airborne bacteria chapter 7 .in .. topley and Wilson ‘s microbiology and microbial Infections .. bacteriology -1,10th ed. Borriello ps ,murray pr, funke g, eds. (asm press ,Washington dc) 2005 ..185-194
7. Cox cs, wathes cm . bio-aerosols in the environment .in .. bioaerosols handbook .cox cs ,wathes cm, eds. (lewis publishers, boca ration fl) 1995..11-14
8. Mohr aj .fate and transport of microorganisms in air, chapter 74 , in .. manual of environmental microbiology 2nd ed . hurst cj , Crawford rl , Knudsen g , melnerney m, stezenbach ld, eds. (asm press ,Washington dc) 2002..827-38.
9. Macher j .ammann ha , burge ha, Milton dk , morey pr .(eds) chapter 1. in .. bio-aerosols ..assessment and control (amercian conference of governmental industrial hygienists ,Cincinnati) 1999..1-5.
10. Schaal kp.medical and microbiological problem arising from airborne infection in hospitals .j hosp infect 1991.,18(suppia a)..451-9.
11. Ayliffe ga.role of the environment of the operating suite in surgical wound infection rev infect dis 1991.,13(suppi .10)..s800 –s804 .
12. Eickhoff tc .airborne nosocomial infection .. a contemporary perspective . infect control hosp epidemiol 1994.,15..663-72.
13. beggs cb .the airbone transmission of infection in hospital buildings . fact or fiction\ indoor built environ 2003,12..9-
18
14. Stezenbach ld . introduction to aerobiology , chapter 72. in ..manual of environmental microbiology 2nd ed. Hurst cj,
Crawford rl, Knudsen g , mclnerney m, stetzenbach ld, eds. (asm press , Washington dc) 2002..801-813.
15. Cox cs .stability of airbone microbes and allergens, chapter 6 . in bio-aerosols handbook .cox cs, wathes cm, eds .(lewis publishers , boca raton fl) 1995..77-86.
16. Pasanen p, pasanen al, janunen m . water condensation promotes fungal growth in ventilation ducts. Indoor air
1993.,3..106-112.
17. Available at . indoor air quantity corporation .http../www. Germology ..com/bio-aerosols .htm .accessed janurary
25,2007.
18. Available at .. peosh indoor air quantity .http..//www.state. nj.us /health /eoh/peoeshweb /iaqdoc.. htm. Accessed January 25, 2007.
19. Ayliffe gaj , babb jr , taylor lj .(eds) infection and the spread of microorganisms , chapter 3. in .. hospital acquired infections .. principles and prevention 3nd ed. (Butterworth Heinemann publications, Oxford) 1999; 38-40.
20. Sawyer LA, Murphy JJ, Kaplan JE, Pinsky PF, Chacon D, Walmsley S et al. 25- to 30-nm virus particle associated withy a hospital outbreak of acute gastroenteritie with evidence ofr airbourne transmission, Am J Epidemiol 1988;127:1261-71. |