|
|
|
| Ameloblastomatous Coc: A Rare Histologic Entity |
Tamanna 1 , Susmita Saxena 2 , Pooja Aggrawal 3 , Preeti Sharma 4
1 Sr.Lecturer , Dept. of Oral Pathology - Himachal Dental College
2 Professor , Dept. of Oral Pathology - Esic, Rohini, New Delhi
3 Reader , Dept. of Oral Pathology - Subharti Dental College, Meerut
4 Reader , Dept. of Oral Pathology - Subharti Dental College, Meerut
|
| Address For Correspondence |
Dr. Tamanna, 183/7, Upper Samkheter,
Near Khatri Sabha Mandi H.P |
| Abstract |
| Introduction: Calcifying odontogenic cyst is an uncommon developmental odontogenic cyst first described by Gorlin in 1962. It is considered as an extremely rare cyst and accounts for only 1% of jaw cysts reported. Because of its diverse histopathology, there has always been confusion about its nature as a cyst, neoplasm or hamartoma. Here, we present a case of calcifying odontogenic cyst with ameloblastic proliferation- an extremely rare histological variant. Case Report: A 21 year old male reported to the Department of Oral Pathology and Microbiology, Subharti Dental College, Meerut with the chief complaint of swelling in left lower jaw. Biopsy report was suggestive of COC for which he was treated. Patient reported again, one year later, with the recurrence of the swelling in the same site. Radiographic examination revealed multilocular cystic lesion in the left posterior part of the mandible with impacted 3rd molar and expansion of the buccal cortical plate. Histopathological Features: Microscopic features showed proliferating islands of thin odontogenic epithelium. At places, superficial region of epithelium showed ghost cells and calcifications, with condensed and hyalinized connective tissue with few inflammatory cells. Treatment: The lesion was surgically removed. No recurrence has been recorded in the ensuing 12 months. |
|
| Keywords |
| Calcifying odontogenic cyst, odontogenic epithelium, ghost cell |
|
| Full Text |
Introduction:
The Calcifying odontogenic cyst (COC) was first reported as a separate pathologic entity by Gorlin et al in 1962. In 1971, the WHO classification defined COC as “a non-neoplastic cystic lesion in which epithelial lining shows a well defined basal layer of columnar cells, an overlying layer often many cell thick and that may resemble stellate reticulum and masses of ghost epithelial cells that may be in the epithelial cyst lining or in the fibrous capsule[1].
According to Shear, it accounts for only 1% of jaw cysts reported. As the number of reports increased, it was proposed that COC was indeed a heterogeneous group of entities with distinct histopathologic findings. In agreement with the new classification of WHO 2005, the term “Calcifying cystic odontogenic tumor” (CCOT) has been replaced with COC and is described as an uncommon developmental lesion that demonstrates histopathologic diversity. Because of its diverse histopathology, there has always been confusion about its nature as a cyst, neoplasm or hamartoma[3]. Odontogenic tumors such as ameloblastoma have been reported to be associated with CCOT. Here, we present a case of calcifying odontogenic cyst with ameloblastic proliferation- an extremely rare histological variant.
Case Report:
A 21 year old male reported to the Department of Oral Pathology and Microbiology, Subharti Dental College, Meerut with the chief complaint of swelling in the left lower jaw, extending from the body of the mandible to the ramus of the mandible, gradually increasing in size. Initially swelling was non tender but gradually became tender. Intraorally, obliteration of buccal vestibule was seen in the first and second molar region. Also lingual cortical plate expansion was seen in the third molar region. Radiographically; unilocular radiolucency in left ramus of the mandible, involving impacted third molar, along with resorption of second molar was evident. On the basis of clinical and radiographic examination, a provisional diagnosis of ameloblastoma / dentigerous cyst was given and incisional biopsy was advised. Microscopic examination of the biopsied specimen showed proliferating islands of thin odontogenic epithelium, with basal columnar cell and stellate reticulum. At places, superficial region of the epithelium showed ghost cells while surrounding capsule was condensed and hyalinized. The histopathological features were suggestive of COC. Marsupilization was done and patient was recalled after 15 days but patient did not turned up.
Patient reported again one year later with the recurrence of the swelling in the same site with buccal cortical plate expansion [Fig 1]. Radiographic examination revealed multilocular radiolucency in the left posterior part of the mandible extending from the left body of the mandible to the ramus of the mandible with impacted third molar [Fig 2]. Microscopic features showed disrupted epithelial lining of variable thickness, showing basal columnar cells with palisading arrangement and superficial cells showing minute degree of keratinzation[Fig 3]. Supporting connective tissue showed loosely arranged collagen fibres with less cellularity. Few odontogenic islands and strands were seen within the connective tissue[Fig 4]. Patchy distribution of inflammatory cells and areas of hemorrhage and degeneration were seen. Well defined cystic lining was present with ghost cells and calcifications and diagnosis of calcifying odontogenic cyst with ameloblastomatous proliferation was made. The lesion was surgically removed. No recurrence has been recorded in the ensuing 12 months.
 | Fig 1. Swelling In The Left Lower Jaw, Extending From The Body Of The Mandible To The Ramus Of The Mandible.
 |
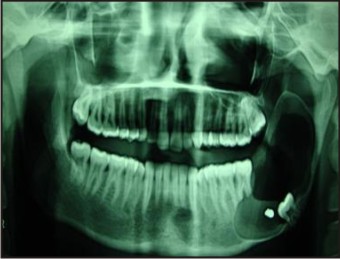 | Fig 2. Multilocular Radiolucency In The Left Posterior Part Of The Mandible Extending From The Left Body Of The Mandible To The Ramus Of The Mandible With Impacted Third Molar
|
![Fig 3. Homogeneous Eosinophillic Areas Resembling Ghost Cells With Large Keratinzing Areas And Areas Of Concentric Calcifications [H & E X 10]](article-image-5626-FIG_3._HOMOGENEOUS_EOSINOPHILLIC_AREAS_RESEMBLING_.jpg) | Fig 3. Homogeneous Eosinophillic Areas Resembling Ghost Cells With Large Keratinzing Areas And Areas Of Concentric Calcifications [H & E X 10]
|
![Fig 4. Cystic Spaces Lined By Tall Columnar Cells With Lumina Containing Eosinoplillic Material Along With Stellate Reticulum Like Cells [H & E X 10]](article-image-5627-FIG_4._CYSTIC_SPACES_LINED_BY_TALL_COLUMNAR_CELLS_.jpg) | Fig 4. Cystic Spaces Lined By Tall Columnar Cells With Lumina Containing Eosinoplillic Material Along With Stellate Reticulum Like Cells [H & E X 10]
|
Discussion:
The calcifying odontogenic cyst represents a heterogeneous group of lesions that exhibit a variety of clinicopathologic and behavioral features. Calcifying odontogenic cyst occurs either as an intraosseous or extraosseous lesion, with the intraosseous form being predominant. In the new classification of WHO (2005), the term calcifying cystic odontogenic tumor (CCOT) has been replaced with calcifying odontogenic cyst (COC) that constitutes a benign cystic neoplasm that presents an epithelium similar to an ameloblastoma, with ghost cells which may display calcification[2].
COC is an uncommon lesion accounting for 1%of jaw cysts; the ameloblastomatous COC is even less common[3]. Hong et al reported 92 cases of COC, out of which 11 cases (14%) were ameloblastomatous COC. Aithal et al and Iida et al also documented single case reports of ameloblastomatous COC[2][3].
Prior to separation of this entity by Gorlin et al, it was often misdiagnosed as some form of ameloblastoma[2]. Attempts were made by Praetorius et al, Hong et al and Buchner to classify the COC based on the dualistic concept as against the earlier monistic concept. However, the question concerning the nature of COC seemed to be solved by Toida more recently, who classified COC into a cyst and a neoplasm. The neoplasm is divided into benign and malignant types, and the terminology-calcifying ghost cell odontogenic tumor (CGCOT) is used for benign neoplasm type. The CGCOT may appear to be either cystic or solid in architecture. The cystic variant of CGCOT and the solid one may be named ‘cystic CGCOT’ and ‘solid CGCOT’, respectively. Thus, the lesion showing cystic architecture and an extensive intramural ameloblastoma like proliferation may be classified as the cystic CGCOT[3].
It is well known that the epithelial lining of the COC has the ability to induce the formation of dental tissues in the adjacent connective tissue wall and the odontoma is a commonly associated odontogenic tumor. Some reports showed that COC often coexists with other odontogenic tumors, such as ameloblastoma, ameloblaststic fibroma, ameloblastic fibro-odontoma, etc[4].
The classification advocated by Hong et al has two categories for COC associated with ameloblastoma: the ameloblastomatous cystic variant and the neoplastic variant associated with ameloblastoma. The former is characterized by a unicystic structure in which the lining epithelium shows unifocal or multifocal intraluminal proliferative activity that resembles ameloblastoma arising from COC (ameloblastoma ex COC)[5].
However, it may be difficult to distinguish ameloblastomatous COC from ameloblastoma arising from COC (ameloblastoma ex COC). An ameloblastomatous COC represents areas similar to simple unicystic type along with intraluminal and intramural ameloblastomatous proliferation, which are usually plexiform in pattern but can be follicular. The ameloblastoma like proliferation typically lacks Vickers and Gorlin criteria of ameloblastoma like cells and they also show occasional ghost cells and calcifications within proliferations[2].
On the other hand, ameloblastoma ex COC designates an ameloblastoma arising from the cyst lining epithelium of COC, shows ameloblastic proliferation within the cystic wall without ghost cell and calcification. Vickers and Gorlin criteria for ameloblastoma-like cells can be easily identified[2].
Ameloblastomatous COC microscopically resembles unicystic ameloblastoma except for ghost cells and calcifications within the proliferative epithelium. Ameloblastomatous COC occurs intraosseously as seen in our case. This subtype of COC is distinct from true ameloblastoma arising in COC[6].
In the present case, although the basal cells showed ameloblastic proliferative activity, they did not completely meet the histopathologic criteria of early ameloblastoma as suggested by Vickers and Gorlin. Hence, the case has been diagnosed as ameloblastomatous COC and has been placed into the category ‘cystic calcifying ghost cell odontogenic tumor (CGCOT) as suggested by Toida[7].
In the study by Hong et al, only 2 of 92 COCs were ameloblastomtous ex COC and 11 were amelobastomtous COCs[2]. Up to now, none of the cases showed aggressive growth and invasion into the surrounding tissue[8].
Because of the rarity of ameloblastomatous CCOT, determination of the most common age, sex and location of this lesion is difficult. According to the case reports in the literature, it seems that most of the patients are between 10 to 30 years old, and the tumor tends to involve the posterior region of the mandible[8]. In our case, patient was of 21 years old and lesion was involving posterior mandibular region. Also, as far as the sex of the patient is concerned, no difference was observed. Our case appeared radiographically as a multilocular lesion involving impacted left third molar with resorption of the second molar root.
Histopathologically, our case has been diagnosed CCOT due to the ghost cells in the ameloblastomatous epithelial islands, and it fits into the category of cystic CGCOT, as suggested by Toida, CCOT type III (ameloblastomatous). Since, only 12 months have passed from the surgery of the reported case, and the short follow up time, no real conclusion would be drawn regarding the recurrence. Moreover, there are no complete reports about treatment and recurrence of this lesion, because of the limited follow up information. In this regard, Buchner suggested that if COC was associated with an ameloblastoma, its behavior and prognosis would be that of ameloblastoma rather than COC[6].
In none of the articles on ameloblastomatous CCOT, a special method such as IHC study or ultrasonic study was performed, but immunohistochemically, there was no difference in amelogenin or CK19 expression among COC with various histological features; there was only a slight difference in bcl-2 and Ki-67 expression[9].
Keeping in mind the above distinguishing features of different types of COC, we classified this lesion as ameloblastomatous COC- a rare entity.
Authors with year Clinical Features Histopathological Features
Aithal et al.
(2003) Age: 28-years
Sex: Female
Clinical presentation: Painless swelling in the left posterior region of the mandible.
Intraorally,well-defined bony hard, non tender swelling of 2.5 × 2.0 cm with smooth surface in relation to mandibular first and second premolars extending to the floor of the mouth. The mucosa overlying the lesion was intact.
Radiographic findings: Multilocular radiolucency in the left mandibular posterior region extending from the mesial surface of the canine to that of the second molar.
Ghost cells in the cystic epithelium and juxtaepithelial hyalinization in some areas. Odontogenic epithelium in the form of rosettes and acanthomatous ameloblastic islands in the connective tissue lining of the cyst.
Iida et al.
(2004) Age: 17 years
Sex: Male
Clinical presentation: Bony swelling of the right mandibular body and facial asymmetry with slight pain on palpation at swollen area.
Radiographic findings: Well-defined multilocular radiolucency from the right lower second molar to the right ramus with remarkable bony expansion toward buccal and lingual sides. Involvement of the entire ramus and coronoid process. The lesion contained the unerupted lower second molar dislocated inferiorly to a position below the first molar. Pressence of odontogenic epithelium with many masses of ghost cells with calcification, and solid parts showing ghost cells and ameloblastomatous proliferations seen in the connective tissue of the cyst wall.
Present case Age: 21 Years
Sex: Male
Clinical presentation: Bony swelling in left lower jaw, extending from the body of the mandible to the ramus of the mandible with facial asymmetry, gradually increasing in size. Initially swelling was non tender but gradually became tender.
Intraorally obliteration of buccal vestibule was seen in the first and second molar region with buccal cortical plate expansion in the third molar region.
Radiographic findings: multilocular radiolucency in the left posterior part of the mandible extending from the body to the ramus of the mandible with impacted third molar. Disrupted epithelial lining of variable thickness, with ghost cells and calcifications, ameloblastomatous proliferations seen in the connective tissue.
Supporting connective tissue shows loosely arranged collagen fibres with less cellularity.
Conclusion
In agreement with the new classification of World Health Organization (WHO) 2005, calcifying odontogenic cyst (COC) or calcifying cystic odontogenic tumor (CCOT) is an uncommon developmental odontogenic lesion that demonstrates histopathologic diversity. Odontogenic tumors such as ameloblastoma have been reported to be associated with CCOT. In accordance with new classification of WHO and recent studies, our case is classified in the less common type of CCOT; CCOT type III; and in this variant only few cases have been reported. Our case did not show any evidence of recurrence after treatment till date, but there is no doubt that careful post operative observations are necessary for COCs which are associated with an ameloblastoma.
References:
1. Gorlin RJ, Pindborg JJ, Odont, Clausen FP, Vickers RA. The calcifying odontogenic cyst- a possible analogue of the cutaneous calcifying epithelioma of Malherbe. An analysis of fifteen cases. Oral Surg Oral Med Oral Pathol 1962; 15: 1235-1243.
2. Hong SP, Ellis GL, Hartman KS.Calcifying odontogenic cyst. A review of ninety-two cases wit reevaluation of their nature as cysts of neoplasms, the nature of ghost cells, and subclassifcation. Oral Surg Oral Med Oral Pathol 1991; 72: 56-64.
3. Aithal D, Reddy BS, Mahajan S, Boaz K, Kamboj M. Ameloblastomatous calcifying odontogenic cyst: a rare histologic variant. J Oral Pathol Med 2003; 32: 376-78.
4. Ledsema- Montes C, Gorlin RJ, Shear M, Prae Torius F, Mosqueda A, Altini M, et al. International collaborative study on ghost cell odontogenic tumors: calcifying cystic odontogenic tumor, dentinogenic ghost cell tumor and ghost cell odontogenic carcinoma. J Oral Pathol Med 2008; 37: 302-308.
5. Iida S, Ueda T, Aikawa T, Kishino M, Okura M, Kogo M. Ameloblastomatous calcifying odontogenic cyst in the mandible. Dentomaxillo Radiol 2004; 33, 409-412.
6. Buchner A. The central (intraosseous) calcifying odontogenic cyst: an analysis of 215 cases. J Oral Maxillofac Surg. 1991; 49: 330- 339.
7. Toida M. So-called calcifying odontogenic cyst; a review and discussion on the terminology and classification. J Oral Pathol Med. 1998; 27; 49-52.
8. Mashhadi Abbas F, Moshref M, sargolzaie S, kargahi N. Ameloblastomatous calcifying cystic odontogenic tumor: A rare histologic Variant. Shiraz Uniz dent J. 2009; 9(1): 45- 48.
9. Yoshida M, Kumamoto H, Ooya K, Mayanagi H. Histopathological and immunohistochemical analysis of calcifying odontogenic cysts. J Oral Pthol Med. 2001; 30: 582- 588.
|
|
|
|
|
|
|