Introduction:
The mandibular premolars have a high flare up and failure rate because of extreme variations in root canal morphologies.[1] A study at the University of Washington in 1955 assessed the failure rates of non-surgical root canal therapy (NSRCT) in all teeth and reported mandibular 1st premolar to have failure rates at about 11.45%; which may be due to variations in root canal morphology and difficult access to additional canals.[2] In majority of cases, mandibular 1st premolar usually possess one canal and one foramen (70%), while two canals exit in two foramina in 1.5% cases. Three canals exit in three foramens is reported at about 0.5% cases.[3]
Literature also has reported very less regarding cases of three rooted mandibular 1st premolars. According to Cleghorn, the incidence of three rooted mandibular 1st premolar is 0.2%.[2] Vertucci showed incidence of three canals is 0.5%, Pinder and Kuttler reported at 0.9%, whereas Zillich and Dowson reported 0.4% .[4], [5], [6]
This case reports the management of such a three rooted mandibular 1st premolar with single canal in each root with the help of CBCT for correct endodontic diagnosis and management.
Case Presentation
A 32 year old male reported to us with the chief complaint of pain in his lower left back tooth region of 1 week duration. Pain was recurrent accompanied with pus discharge occasionally. Patient reported to be on over the counter pain relieving medication during acute stages of the condition.
Patient was otherwise normal. General examination revealed submandibular lymphadenopathy on left side. On clinical examination, the tooth 34 (FDI notation) showed carious lesion and revealed tenderness to percussion. Vitality testing and Periapical radiographs was advised further. A provisional diagnosis of chronic periapical abscess was given.
Investigations
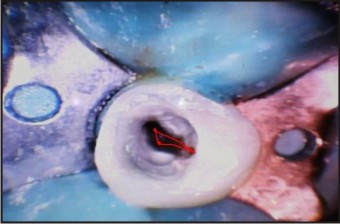
There was no response for vitality test like electric pulp test and heat test with gutta-percha. On radiographic examination there was presence of radiolucent lesion surrounding the apex of tooth 31. Closer observation of the root showed hazy root canal outline arising a question of presence of multiple roots (Fig 1). To ascertain accurate number and configuration of root canal morphology, CBCT was advised to ensure better reliability of success. CBCT images revealed mandibular 1st premolar to possess 3 separate root canals with 3 exiting foramina (Fig 2). Confirmatory diagnosis of Mandibular 1st premolar bearing 3 root canals and 3 foraminas with periapical abscess was obtained.
 | Fig 1 : Iopa X-ray Of 36 Involving Furcation Area
 |
 | Fig 2 : Intr Oral View After Extraction Of 36 & 37 Had Not Completely Erupted
|
Treatment & Follow Up
The area was anaesthetized with 1:80,000 lignocaine with adrenaline. Under rubber dam isolation, access cavity was prepared to locate the three canals - mesio-buccal, disto-buccal and lingual (Fig 3). All the three canals were negotiated with 10 number k file and working length was determined (Fig 4). The canals were cleaned and shaped with manual hero shapers till 30 - 4% and irrigation with 2.5% sodium hypochlorite and 17% EDTA followed by final irrigation with 0.9% saline. The master cones were selected (Fig 5), canals were dried with paper points and obturated with guttapercha and seal apex sealer, (Sybron Endo, Glendora, CA, USA). (Fig 6). The patient was periodically checked clinically and a four months follow up radiograph (Fig 7) has shown signs of reduction in periapical rarefaction, on comparison with initial pre-treatment radiograph (Fig 1).
 | Fig 3a : Band Adaptation On 35 & 37
|
 | Fig 3b : A Wire Frame Work
|
 | Fig 3c : Fabricated Interim Space Maintainer
|
 | Fig 4 : Post Operative Veiw , Cemented Space Maintainer
|
 |
|
Discussion
Anatomic variations in mandibular premolars make endodontic treatment a challenging one. Trope et al did a study on anatomic variations in mandibular premolars based on race and found that the prevalence of more than one canal is predominant in Afro-Americans than Caucasians.[7]
The Washington study in the year 1955 showed that the failure rate was more in mandibular premolar treatment in the range of 11.45%. This is because of more variations existing in the root canal anatomy.[2] According to Cohen, these teeth have a high flare-up and failure rate.[1] Serman et al did a radiographic analysis in the presence of multiple root canals on mandibular premolars and found that 18.1% of premolars have more than one canal in which first premolars were involved in 15.7% and second premolars in 7%.[8]
Kartal et al had done a study in a Turkish population and found that presence of two or three canals in mandibular premolars in the same root was around 9.62% and having more than one canal at the apex was 23.49%.[9] Cleghorn et al have reported an incidence of a three-rooted mandibular first premolar at just 0.2% .[2]
Failure to locate the extra canals is one of main reason for the endodontic treatment failure. Hoen and Pink did a study which stated that 42% of missed root canals required retreatment.[10]
Hence proper understanding of the root canal anatomy is essential for the successful endodontic treatment. A good pre-operative radiograph is mandatory to know the root canal anatomy. Even though it is two dimensional, at least two radiographs are needed with 15-200 angulation either in mesial or distal direction. This helps in identification of presence of extra root or canal most of the times. [11]
However, Martinez-Lozano et al. recommend up to 40° mesial horizontal angulation which will be more effective in identifying the extra canals. A shift of 15 –200 in the vertical axis is effective in identifying the extra canal only in mandibular first premolar.[12],[13]
Recent advancement in imaging techniques like CBCT which is three dimensional imaging helps in understanding and identifying the complex pattern of roots, and as well as the canal anatomies. This technique also overcomes the routine problem of distortion of two dimensional radiographic images which makes endodontic treatment outcome more predictable and successful.
This case report emphasises the advantage of using CBCT in selective cases, to identify and confirm the presence of additional roots, canals and the extent of peri-radicular lesion too in diagnosis and completion of the endodontic procedure satisfactorily.
Conclusion
Literature shows that variations in the root canal anatomy can always be expected when diagnostic radiographs reveal images which differ from routine ones, in terms of image parameters. Such situations can be identified with other advanced imaging modalities as CBCT which are available and affordable today. It is also important that the practitioners should be aware of such diagnostic modalities to refer the patients and be updated in interpretation of the resulting images. However the referring endodontists should be absolutely selective in the use of such techniques, considering the radiation exposure in especially in younger age groups and other medically vulnerable situations like pregnancy (13).
This case will be followed up with further clinical evaluation to ascertain the treatment outcome.
Learning Points/Take Home Messages:
• Mandibular 1st premolar possesses varying morphology which is a risk factor in prognosticating a case.
• CBCT is a good adjunct to traditional diagnostic aids.
• Good understanding of root canal morphology is necessary for ensuring better success; in this aspect CBCT enables this.
References:
1. Kenneth M. Hagreaves, Stephen Cohen. Cohen’s Pathways of the Pulp. 10th ed. St. Louis: CV Mosby, 2011:204.
2. Blaine M. Cleghorn, William H. Christie, Cecilia C. S. Dong. The Root and Root Canal Morphology of the Human Mandibular First Premolar: A Literature Review. J Endod 2007;33(5):509-516.
3. Suresh Chandra, Gopi Krishna. Grossman’s Endodontic Practice. 12thed. India: Wolters Kluwer Health, 2010:205.
4. Vertucci FJ: root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58(5):589-599.
5. Pineda F, Kuttler Y: Mesiodistal and Buccolingual roentgenographic investigation of 7275 root canals. Oral Surg Oral Med Oral Pathol 1972; 33(1):101-110.
6. Zillich R, Dowson J. Root canal morphology of mandibular first and second premolars. Oral Surg Oral Med Oral Pathol 1973;36(5):738–44.
7. Trope M, Elfenbein L, Tronstad L: Mandibular premolars with more than one root canal in different race groups. J Endod 1986;12(8):343-345.
8. Serman NJ, Hasselgren G: The radiographic incidence of multiple roots and canals in human mandibular premolars. Int Endod J 1992;25(5):234-7.
9. Kartal N Yanikoglu F: The incidence of mandibular premolars with more than one root canal in a Turkish population. J Marmara Uni Dent Fac 1992;1(3):203-10.
10. Hoen MM, Pink FE. Contemporary endodontic retreatments: An analysis based on clinical treatment findings. J Endod 2002;28(12):834–6.
11. Balakasireddy K, Pavan Kumar K, Gijo John, et al. Cone Beam Computed Tomography Assisted Endodontic Management of a Rare Case of Mandibular First Premolar with Three Roots. J Int Oral Health 2015;7(6): 107–109.
12. Martínez-Lozano MA, Forner-Navarro L, Sánchez-Cortés JL. Analysis of radiologic factors in determining premolar root canal systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88(6):719–22.
13. Shawn Adibi, Wenjan Zhang, Tom Servos, et al. J Dent Education 2012;76(11):1437-1442.
|