Introduction
Dentigerous cyst is the most common type of developmental odontogenic cyst was formerly known as follicular cyst[1]. Inflammatory dentigerous cyst is a type of dentigerous cyst which occurs in mixed dentition stage. The term inflammatory follicular cyst was given by Main for those dentigerous cysts which showed area of inflammation in their lining[2]. These inflammatory dentigerous cysts are reported to occur in the first and early part of the second decades of life. There occurrence was found to be more in males, and there did not appear to be any racial predilection[3].
Dentigerous cyst of inflammatory origin occur mostly in immature teeth as a result of inflammation from a non-vital deciduous tooth or another source of infection from teeth treated with pulpotomy or pulpectomy and spread inflammation to involve the underlying tooth follicle[4]. The relation between persistent and prolonged inflammation of a primary tooth and development of a dentigerous cyst involving the permanent successor has been extensively discussed. Histological evidence for this cyst suggests that inflammatory exudate induced by an infection spreads to dental follicle, causing separation of reduced enamel epithelium from the enamel leading to development of dentigerous cyst.[5] The aim of the present article is to report a rare case of dentigerous cyst of inflammatory origin in a male child patient with with grossly decayed primary teeth, involving unerupted maxillary first premolar.
Case Report
A six year old boy (Figure 1) reported to the Department of Pedodontics and Preventive dentistry, Himachal dental college, Himachal Pradesh with a chief complaint of painless swelling in left maxillary posterior region since 6 months. On general examination the patient was healthy with no significant past medical history. Patient had previously visited a private dental clinic for the same where he was prescribed antibiotics and referred to our college. On extra oral examination, facial asymmetry was noted on left upper side of the face, with no sinus or active discharge of pus.
 | Figure 1
 |
On intraoral examination a bony swelling (Figure 2) caused by bulging of cortical bone, extending over buccal vestibule of 63,64,65 was seen. The swelling was ill defined , firm in consistency, painless on palpation, and measured about 2x2cm without any bruit or pulsation. Swelling was associated with grossly carious left deciduous first molar(64).
 | Figure 2
|
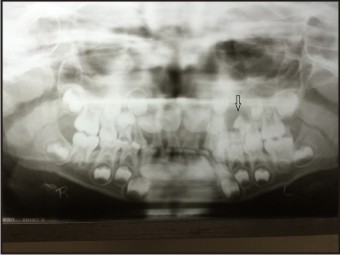
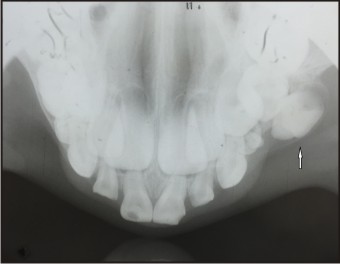
OPG (Figure 3) showed unilocular radiolucent lesion with well corticated margins in inter-radicular region of maxillary deciduous left first molar(64). This radiolucency also involved the unerupted left first premolar(24), which was displaced bucally and distally below the maxiallry deciduous second molar. Occlusal radiograph (Figure 4) showed expansion of buccal cortical plate with displaced and rotated unerupted first premolar. With the above findings the case was diagnosed provisionally having a dentigerous cyst. Fine needle aspiration cytology was conducted and it was found of benign lesion containing straw colored cystic fluid with inflammatory and benign cells. On the basis of radiographic and FNAC report final diagnosis of dentigerous cyst was made.
 | Figure 3
|
 | Figure 4
|
Treatment consisted of an preventive approach to preserve the developing 1st premolar(24). Therefore, marsupialization of the lesion was planned through the extracted socket of grossly decayed deciduous 1st molar (which was done under L.A) to create a window allowing continuous drainage of the cystic content. Prior to surgery, routine blood and urine examinations were carried out, the results were within normal limits. The cyst cavity was packed with sterile iodoform gauze to achieve homeostasis and to prevent hematoma formation. The iodoform gauze was changed after a week. The patients were advised to maintain good oral hygiene and a chlorhexidine mouth rinse was prescribed. Follow-up after 3 month revealed that there was slight occlusal movement of the developing tooth bud, with apparent reduction in the radiolucency.
After 6 months, there was further occlusal movement of the developing tooth and there was a huge reduction in the radiolucency and formation of bone. (Figure 5)
 | Figure 5
|
After 12 months, there was further occlusal movement of the tooth and there was almost complete reduction in the radiolucency. The root formation of maxillary left 1st premolar progressed to one third. (Figure 6)
 | Figure 6
|
Discussion
Two types of dentigerous cysts have been reported in the literature i.e developmental and inflammatory types. Developmental type of dentigerous cyst is mostly formed around the crown of an unerupted tooth by accumulation of fluid either between the reduced enamel epithelium and the enamel or in between the layers of the enamel organ. This occurs as a result of pressure exerted by an erupting tooth on an impacted follicle which obstructs the venous outflow and thereby induces rapid transudation of serum across the capillary wall[6]. The other theory of origin of developmental type dentigerous cyst stated that the most likely origin of the dentigerous cyst is the breakdown of proliferating cells of the follicle after impeded eruption.[7]
Inflammatory dentigerous cyst (IDC) is a type of dentigerous cyst which is found in mixed dentition only. It develops when the inflammation present at the root apex of a non-vital primary tooth spreads to involve the follicle of the unerupted immature permanent successor.[8] In the differential diagnosis of IDC, an odontogenic keratocyst, unicystic ameloblastoma, radicular cyst must be considered. All the above mentioned lesions are rare in the first decade of life. Odontogenic keratocyst and unicystic ameloblastoma occur in the second and third decade of life. A radiograph does not differentiate between the various types of lesions as mentioned above which areassociated with the root of a nonvital or a vital primary tooth involving the crown of a developing permanent tooth. Therefore, FNAC and histopathologic examination of the cyst contents and lining is a must for final diagnosis and which was also performed in our case.
Marsupialization or decompression technique has been advocated by several authors for treating dentigerous cyst in young patients.[9],[10] In this conservative technique, creation of an accessory cavity helps to relieve intracystic pressure and accelerate the healing of the cystic lesion.[11] The permanent teeth generally erupt in the oral cavity with or without the need of orthodontic correction. However, the patient should be followed up until the complete eruption of permanent teeth in their designated location. The successful preservation and eruption of the affected teeth in this present investigation may be attributed to the active growth potential and remodeling of bone in children unlike in adults where jaw growth is completed.
Conclusion
Although marsupialization is an unconventional method of treating dentigerous cyst in adults, it is a very effective method in treating dentigerous cyst in children where there is always approximity with the developing tooth buds in the jaws. Follow-up of the patient is also very important and should be done until the complete eruption of permanent teeth in their right location in the oral cavity.as it is seen that if permanent teeth are left undisturbed within the follicle then as the cyst heals in due course of time, these permanent teeth erupt in the oral cavity.
References
1. Waldron CA. cysts and tumors. In: Oral and Maxillofacial pathology, Neville BW, Damm DD, Allen CM, Bouquot JE, (eds), Philadelphia: W.B. Saunders, 1995, p 493-540.
2. Main DMG. Epithelial jaw cysts: 10 years of the WHO classification. J Oral Pathol.1985; 14:1-7.
3. I. R. H. Kramer, J. J. Pindborg, andM. Shear, Histological Typing of Odontogenic Tumours, Springer, Berlin, Germany, 1992.
4. A. Benn and M. Altini, “Dentigerous cysts of inflammatory origin. A clinicopathologic study,” Oral Surgery, Oral Medicine,Oral Pathology, Oral Radiology, and Endodontics, vol. 81, no. 2, pp. 203–209, 1996.
5. Lustig JP, Schwartz-Arad D, Shapira A (1999). Odontogenic cysts related to pulpotomized deciduous molars: clinical features and treatment outcome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 87(4): 499-503.
6. Main DM. The enlargement of epithelial jaw cyst. Odontol Revy 1970; 21:21-9.
7. Toller PA. The osmolarity of fluid from the cyst of jaw. Br Dent J 1970;129:275-8.
8. Bloch JK. Follicular cyst. Dent Cosm 1928;70:708-11.
9. Martinez-Pérez D, Varela-Morales M. Conservative treatment of dentigerous cysts in children: A report of 4 cases. J Oral Maxillofac Surg 2001;59:331-4.
10. Berdén J, Koch G, Ullbro C. Case series: Treatment of large dentigerous cysts in children. Eur Arch Paediatr Dent 2010;11:140-5.
11. Bodner L, Woldenberg Y, Bar-Ziv J. Radiographic features of large cysts lesions of the jaws in children. Pediatr Radiol 2003;33:3-6.
|