Introduction
Complete denture wearers may be one of the most neglected dental patients. With complete dentures, insufficient denture retention is a powerful determinant of patients satisfaction.[1] Several factors and complex interactions affect the retention and stability of CD in the oral cavity, including atmospheric pressure, intimate adaptation with hard and soft tissues, presence of thin film of saliva between prostheses and tissues. Denture retention is compromised if any of these factors are compromised. Patients with complete dentures require unique considerations due to their compromised oral anatomy and systemic conditions and medications that further affect denture retention, all of which reduce the patient’s ability to successfully wear their prosthesis.[2]
The most common complaint of complete denture patients is diminished function of the prostheses for a variety of reasons. The various contributing factors include warping or breakage, V- shaped palatal vault, atrophy of the bony tissues, altered salivary flow, neuromuscular inco-ordination, temporo-mandibular dysfunction, trauma and others. Amongst these, the most deleterious factors is the atrophy of the alveolar ridge, which may result in poor retention of the prostheses.
Residual ridge resorption is a lifelong condition that plaques the CD patients after exodontias and subsequent denture placement. Alveolar ridge resorption compromises denture retention and stability, rendering denture loose and non-serviceable to the patient.[3] Though, retention in such cases can be enhanced by placing basal implants but it is not always valid, as in cases of elderly and medically compromised cases. The non–surgical alternatives that can be employed to enhance the denture retention include denture adhesive pastes, powders, and pads.
Denture adhesives merely reduce the amount of lateral movements that occur while dentures are in contact with basal tissues. This benefit can mislead a patient into ignoring his or her need for professional help when dentures actually become ill-fitting.[4] Patient response to the use of these materials is not universally positive. Some patients object to the "grainy" or "gritty" texture of powder or to the taste or sensation of semi-dissolved adhesive materials that escape from under the denture.[5],[6] Others object to the difficulties encountered in removing adhesive from the denture and the oral tissues and the cost of the material. Denture adhesive products are frequently regarded as an impediment to a dentist's ability to evaluate accurately the health of a patient's oral tissues.[7],[8]
Patents on suction cup dentures were issued to J.Spyer and R.S.Ingalls in 1885.[9] These patents covered multiple projections on the tissue (basal) surface of dentures. A patent was issued in 1907 to G. W. Morgan for suction cavities in a soft rubber sheet. Dr. Arthur C Jermyn, originally from Rochester, New York, resurrected the idea of suction cup-retained dentures with research that began in 1952. In his research and clinical studies, Dr. Jermyn noted that the unique alteration in the denture intaglio increased the surface area covered by the suction cups, distributing even pressure and greatly enhancing denture retention. Jermyn in 1967 depicted a technique for specific cases where implant treatment was either inappropriate or had already failed. The technique depicted in this paper has been traced from that originally described by Jermyn in 1967.[10]
This clinical report presents a patient who was successfully treated by prostheses lined with a heat-cured, soft polymer material containing multiple small suction cups covering the basal seat area.
Case Report
The patient, a 65-year-old male in excellent health, presented with a history of ill fitting previous denture which he got made 5 years back. Past medical history revealed that patient is diabetic since past 9 years. Past dental history revealed extraction of his remaining teeth 6 years due back to periodontal reasons. Since then patient is denture wearer but is unhappy with the retention of the existing dentures.Intraoral examination revealed completely edentulous severely resorbed maxilla and edentulous favourable mandibular residual ridges. Patient also had a poor experience of gagging on impression making during clinical procedures for the previous denture. Hence, considering the chief complaint of the patient, mucostatic preliminary impression was made with hydrocolloid impression material, single step border molding was carried out with polyether impression material followed by final impressions with fast setting light body impression material to prevent gagging and multiple suction cups were providedon intaglio surface to aid in retention. Single step border molding with final impressions was preferred as it saved time, hence, there was little chance for the patient to gag. The expectation of this prostheses was explained to the patient.
Technique
1. Preliminary Impressions: The preliminary impressions of the maxillary and mandibular arches were made with irreversible hydrocolloid (Zelgan, Dentsply India Pvt .Ltd.)
2. Secondary Impressions And Jaw Relations: The primary casts were obtained over which special trays were fabricated using auto-polymerizing resin (DPI Dental products, India) keeping them 2mm short of the sulcus. One step border molding for maxillary arch was carried out using heavy body polyether impression material (ImpregnumTM Penta Soft Heavy Body, 3M ESPE) and the definitive impression was made using fast setting light body polyether impression material (ImpregnunTM Penta Soft Light Body, 3M ESPE).
Mandibular arch border molding was done in a conventional manner. Master casts were constructed and were indexed in the land area. Maxillary and mandibular occlusal rims were fabricated and jaw relation procedures were carried out in conventional manner.
3. Teeth Arrangement And Try-In: Prosthetic teeth arrangement was done and try- in was accomplished after final wax up of the trial dentures.
4. Special Laboratory Procedure I-Modifying The Maxillary Master Cast: The master cast was prepared by drilling trephine holes, with help of trephine (Fig.1a), that were placed approximately 1.5 mm apart, and had depth of 1 mm and a diameter of 2 mm. The trephine holes covered the entire denture bearing surface of the maxillary arch except 2mm of the denture borders, frenal attachment areas and posterior palatal seal area.(Fig.1b) The holes should be drilled with a definite planned outline. The hould be Compressed Against The Soft Tissues
5. Dewaxing: The temporary denture base was then sealed down on the master cast with wax and flasking and deawaxing procedure was carried out in traditional manner.
6. Special Laboratory Procedure Ii-Modified Laboratory Technique For Maxillary Denture Fabrication: After dewaxing, a 1.5 mm thick wax spacer was adapted over the entire fitting surface of the maxillary cast. This was done so as to prevent the acrylic resin from penetrating the trephine holes and also provided adequate space for the addition of Molloplast- B (Detax Karl Huber GmbH, Ettingen , Germany), later in the procedure (Fig.1c). The teeth were covered with heat cure acrylic resin in dough stage and cellophane sheet was used to seperate it from the wax spacer (Fig.1d). Flask was bench pressed for one hour at two bar pressure. After one hour, flask was re-opened (Fig.1e) and adhesive for Molloplast-B was applied to the surface of the un-cured acrylic resin (Fig.2a) and then Molloplast-B was placed over the surface of the acrylic resin (Fig.2b). The flask was closed again together and curing was done using traditional laboratory protocols. The denture was carefully retrieved, finished and polished so as to avoid tearing of Molloplast- B (Fig.2c)
7. Mandibular Denture Fabrication: After de-waxing of the mandibular try-in, packing & curing and finishing was carried out in conventional manner.
8. Denture Insertion:Denture insertion was done and was checked for retention, stability and occlusion. Patient was instructed for home care and maintenance of prosthesis.
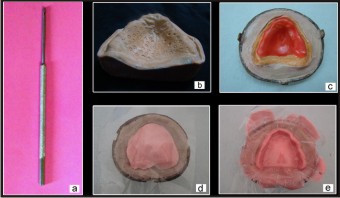 | Figure 1: (A) Trephine, (B) Master Cast With Trephine Holes, (C) Adaptation Of Wax Spacer, (D) Teeth Covered With Heat Cure Acrylic Resin And Cellophane Sheet Placed Over It, (E) Flask Re-opened After One Hour.
 |
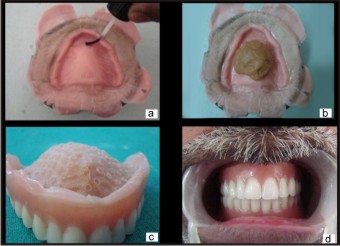 | Figure 2: (A) Adhesive Application For Molloplast- B, (B) Molloplast-b Placed Over Heat Cure Acrylic Resin, (C) Retrieved And Finished Denture., (D) Inta-oral View Of Denture
|
Discussion
Multiple suction cup denture provided retention, stability, and comfort for complete denture wearers, particularly those with significant resorption of their alveolar ridges. Precise trefine holes had to be carefully prepared in the master cast with a special trephine drill. The holes were made 2 mm in diameter, approximately 1 mm deep, and had walls with a 12.5a02;taper. They were spaced 1 to 1.5 mm apart, and prepared perpendicular to the palatal and ridge surfaces (Fig 3)[10]. Drilling the holes is the most sensitive part of this technique. The holes must be drilled perpendicular to the mucosal surface so that the hole core is not broken.
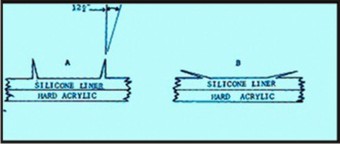 | Figure 3: Mechanics Behind Functioning Of Suction Cups
|
During his research, Dr. Jermyn did biopsy of many patients with multiple suction cup denture. He found focal areas of slight inflammation where a hole had been drilled too deeply. Holes of proper depth did not displace tissues to the point where the suction cups caused inflammation or pathology.[10]
It is well documented fact that suction cups whether single or multiple aid in retention of prostheses. The fundamentals behind increased retention is that whenever suction cups adhere to the mucosa, air inside the suction cups is released thus creating a negative pressure inside the cups. It is this difference in pressure that creates increased retention. The use of a single suction cup for maxillary denture retention is an obsolete concept as its long term usage causes pathological changes (mucosal ulceration and pathological perforations) in the tissues denture. Studies have revealed no demonstrable cell changes as long as suction cups are not too deep. The field of concern here is performance of Molloplast -B . A six-year retrospective follow-up study on complete dentures with Molloplast- B linings showed that common problems were fracture, bleach deterioration, liner separation and yeast deterioration[11]. Some authors[12], recommend that bleach be used to disinfect the denture every night in order to reduce the micro-organism count. A laboratory study[13] has shown sodium hypochlorite to be the most effective disinfectant, being more effective than either microwave radiation or leaving the denture dry overnight.
A study by Gedik and Kulak[14] demonstrated that alkaline peroxide-type denture cleaners have been found effective in the disinfection of silicone-based soft liners contaminated with C.albicans.
There is a conflict between the needs for effective disinfection and maintaining the properties of the materials. It would appear likely that the Molloplast- B would need to be replaced on a 3 - 5 year cycle on average.
Studies were made of tissues taken from several patients wearing these dentures in order to determine the presence and degree of pathosis. There was no demonstrable cell change, as long as the cups were not too deep. Where the cups were too deep, they caused a sore spot to develop.
Conclusion
This article describes a technique of incorporating multi- suction chambers in the tissue surface of the mandibulardenture to enhance the retention and stability. Not only this, chief complaint of patient regarding gag reflex was taken care of by making final impression in fast setting light body impression material and to overcome the problem of looseness of denture due to fast resorption pattern as the patient was diabetic, primary impressions were made with irreversible hydrocolloid. This technique solves many of the physiologic and psychologic problems associated with denture wearing, but this is no panacea for all denture troubles.When properly done, the use of these multiple suction cups canmake the difference between success and failure. When the patient desired and was unwilling for othertreatment modalities, the multi-cup denture liner offered a viable alternative to enhance denture retention.The follow – up was done for every 3 months till one year and no tissue changes and complaints were reported.The multi-cup denture liner, when properly placed, has offered a viable alternative to enhance denture retention when pre-prosthetic surgery may not have been feasible or desired by the patient.
References
1. Felon MR, Sherriff M. An investigation of factors influencing patient,s satisfaction with new complete dentures using structural equation modelling. J Dent 2008;36(6): 427-34.
2. Atwood DA. Reduction of residual ridges: A major oral disease entity. J Prosthet Dent 1971;26(3): 266-79.
3. McCartney JE.Prosthetic problems resulting from facial and intraoral changes in the edentulous patient. J Dent 1981; 9(1): 71-83.
4. Shay K. The retention of complete dentures by Kenneth Shay. Chapter 21: "Rehabilitation of the edentulous patient: fabrication of complete dentures based on statistics" pp. 400-411 [1994 stats] In: Zarb GA, Bolender CL, Carlsson GE, eds. Boucher's Prosthodontic Treatment for Edentulous Patients. 11th ed. St Louis, Mo: Mosby; 1997:400-411.
5. Shay K. Denture adhesives: choosing the right powders and pastes. J Am Dent Assoc. 1991;122:70-76.
6. Berg E. A clinical comparison of four denture adhesives. Int J Prosthodont. 1991;4:449-456.
7. Boone M. Analysis of soluble and insoluble denture adhesives and their relationship to tissue irritation and bone resorption. Compend Contin Educ Dent. 1984;4(suppl):S22-S25.
8. Tarbet WJ, Silverman G, Schmidt NF. Maximum incisal biting force in denture wearers as influenced by adequacy of denture-bearing tissues and the use of an adhesive. J Dent Res. 1981;60:115-119.
9. Spyer J, Ingalls RS, inventors. Dental plate. PUS paatent #310,233. January 6, 1885., United States Patent Office, Washington, DC/ / Spyer J, inventor. Dental suction-plate former. US pPatent #331,840., December 8, 1885.United States Patent Office, Washington, DC.
10. Jermyn A C. Multiple suction cup dentures.J.Prosthet.Dent 1967;18:316–325.
11. Schmidt W F Jr, Smith D E. A six-year retrospective study of Molloplast-B-lined dentures. Part II: liner serviceability. J.Prosthet.Dent 1983; 50:459-465.
12. Mahabob M N, Sambandan T, Kumar B S. Suction cup induced oronasal communication. JIADS 2010; 1:43–46.
13. Ryan J E, Twenty-five years of clinical application of a heat-cured silicone rubber. J. Prosthet. Dent 1991; 65: 658-660.
14. Gedik H , Kulak Özkan Y. Cleaning Efficiency Of Alkaline Peroxide Type Denture Cleansers On Silicone-Based Soft Lining Materials Colonized With Candida albican Balk J Stom, 2009; 13:35-40.
|