Introduction:
The zygomatico-maxillary complex (ZMC) plays a key role in the structure, function, and aesthetic appearance of the facial skeleton. Because of its prominent position, the zygoma is the most common mid-facial bone fractured.[1], [2], [3]
Surgical intervention is not usually taken up unless a functional or esthetic impairment in the form of reduced mouth opening and depression of the cheek prominence is encountered. There are several techniques for the reduction of the fractured zygomatic complex, including the Gillies temporal approach,[4] hook elevation,[5] and the upper buccal sulcus technique.[6] Others include the intranasal transantral approach,[7] reduction through the sigmoid notch,[8] and the modified lateral coronoid technique.[9] Elevation of the zygoma may also be accomplished through a bicoronal or lateral eyebrow incision.
The intraoral approach for zygomatic fracture reduction was first described in 1906 by Lothrop,[10] who elevated fractured zygoma through a fenestration in the canine fossa, elevating the lateral antral wall, and the zygomatic complex, with a blunt instrument. The upper buccal sulcus technique was originally described by Keen in 1909,[6] and has been used successfully for many years,[11] even as an outpatient technique under local anesthesia.[12] However, in a survey of practicing fellows of the British Association of Oral and Maxillofacial Surgeons, the Gillies temporal approach method was used in 74% of cases of severely displaced zygomatic fractures.[13]
The purpose of this article is to describe certain modifications made to the intraoral approach to allow better access to the zygomatic buttress and the choice of the fixation method for these so as to achieve best possible results with minimal surgical morbidity.
Technique:
To access the zygomatic buttress intraorally, local anaesthesia is achieved by a posterior superior alveolar nerve block is administered in to the affected side and the area is also infiltrated with local anaesthetic solution. For palatal side, greater palatine block is administered. A horizontal incision of around 2 cm length is made by using a no. 15 blade in the upper buccal sulcus, extending from canine to first molar area. The mucoperiosteal flap is reflected to expose the underlying fracture. With conventional approaches, only the buttress can be exposed up till its attachment to the body of maxilla or at the zygomatico-maxillary suture. In the modification of the incision, a 1 cm long vertical incision is given in the periosteum starting from the base of the zygomatic buttress and carried upwards along the buttress. The periosteum is then reflected sideways to expose the ascending limb of the buttress. With this modification, complete buttress up to the anterior part of the zygomatic arch can be exposed. After attaining adequate access, the zygomatic bone and arch can be elevated using conventional methods. For fixation, we recommend use of a 4-6 hole L-plate rather than a straight plate as discussed later.
 | L-plate Fixed At The Zygomatic Buttress (Right Side)
 |
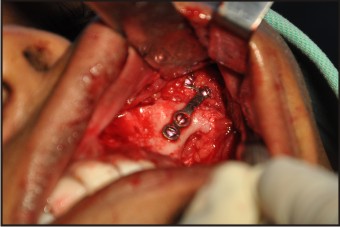 | L-plate Fixed At The Zygomatic Buttress (Left Side)
|
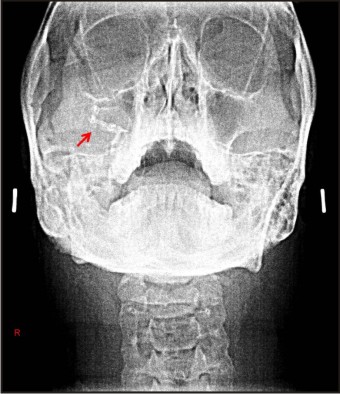 | Pns View Showing L-plate Fixed At The Zygomatic Buttress
|
Discussion:
Various approaches for reduction and fixation of zygomatic fractures include the Gillie’s temporal approach, the hemicoronal and bicoronal approaches, as well as a stab incision over the zygomatic arch region. The major limitation of the Gillie’s temporal approach is that old or comminuted fractures cannot be reduced with this technique. Also, the reduced fracture cannot be fixed with this technique.[14] The hemicoronal and bicoronal approaches are extensive approaches, requiring general anaesthesia, as well as consume a lot of surgical time. The stab incision over the zygomatic arch region leaves behind an unaesthetic scar.
The intraoral methods, though aesthetically acceptable, do not provide adequate visibility and access to the fractured site, up to the zygomatic arch region.[14] The current modification to intra oral incision overcomes this limitation of the intraoral approaches in terms of access to fractures of the anterior part of the zygomatic arch. The same can be fixed using this technique in a very convenient manner. Moreover, if the incision is extended anteriorly, the infraorbital rim fractures can also be reduced with the same approach, without giving any additional incision for the same.
One point fixation is advocated in this approach using a L-plate. The zygomatic buttress is the most rewarding site for plate fixation in most zygomatic fractures.[15] According to Lee et al[16], one plate along the zygomatico-maxillary buttress provides enough stability in most cases. The advantages of one point fixation over two-point and three-point fixation are the reduction of surgical time, less scars and less hardware used.[17], [18] A 4-6 hole L-plate is used instead of a straight plate as it provides two-dimensional stability by preventing rotation of the zygoma. On the other hand, a single straight two-hole or four-hole plate may result in rotation of the zygoma, necessitating fixation at another site.
This technique allows complete visualization of the zygomaticomaxillary buttress, access to the anterior part of the zygomatic arch to facilitate reduction and provide adequate fixation in this otherwise inaccessible anatomic region. The possibility of direct visualization and manipulation of these areas via intraoral approach definitely adds to success especially in terms of morbidity when compared to transfacial surgical approaches. Additionally avoidance of facial scar, minimal surgical time, simplicity of the technique and feasibility under local anaesthesia are other benefits of the approach.
References:
1. Ozkaya O, Turgut G, Kayali MU et al. A retrospective study on the epidemiology and treatment of maxillofacial fractures. Ulus Travma Acil Cerrahi Derg. 2009 15(3): 262
2. Shankar AN, Shankar VN, Hegde N et al. The pattern of the maxillofacial fractures. J Cranio Maxillofac Surg. 2012; 40: 675-679
3. Bogusiak K, Arkuszewski P. Characteristics and epidemiology of zygomaticomaxillary complex fractures. J Craniofac Surg. 2010; 21: 1018-1023
4. Gillies HD, Kilner TP, Stone D. Fractures of the malarzygomatic compound: with a description of a new X-ray position. Br J Surg. 1927; 14: 651-656.
5. Poswillo D. Reduction of the fractured malar by a traction hook. Br J Oral Surg. 1976; 14: 76-79.
6. Keen WW. Surgery, its principles and practice. Philadelphia: WB Saunders. 1909: 1906-1921.
7. Rowe NL, Williams JLl. Maxillofacial Injuries, 2nd edn. Edinburgh: Churchill Livingstone. 1994: 515-521.
8. Harding RL, Herceg SJ. Simple method for reduction of fractures of zygoma. Plast Reconstr Surg. 1968; 42: 176-177.
9. Quinn JH. Lateral coronoid approach for intraoral reduction of fractures of the zygomatic arch. J Oral Surg. 1977; 35: 321–322.
10. Lothrop HA. Fractures of the superior maxillary bone caused by direct blows over the malar bone. A method for the treatment of such fractures. Boston Med Surg J. 1906; CLIV (1): 8-11.
11. Apfelberg DB, Lavey E, Maser MR, Lash H. Upper buccal sulcus approach to reduction of zygomatic fractures. J Trauma. 1977; 17: 847-849.
12. Schnetler JFC. A technique for reducing fractures of the zygomatic complex under local anaesthesia. Br J Oral Maxillofac Surg. 1990; 28: 168-171.
13. McLoughlin P, Gilhooly M, Wood G. The management of zygomatic complex fractures - results of a survey. Br J Oral Maxillofac Surg. 1994; 32: 284-288.
14. Zachariades N, Mezitis M, Anagnostopoulos D. Changing Trends in the Treatment of Zygomaticomaxillary Complex Fractures: A 12-Year Evaluation of Methods Used. J Oral Maxillofac Surg. 1998; 56: 1152-1156.
15. Dierks EJ, Harper GA. The 4 cardinal bends of the zygomatico-maxillary buttress: A technical note. J Oral Maxillofac Surg. 2009: 67: 1149-1151.
16. Lee EI, Mohan K, Koshy JC, Hollier LH. Optimizing the surgical management of zygomaticomaxillary complex fractures. Seminars Plast Surg. 2010; 24 (4): 389-397
17. Makowski GJ, Sickels JEV, Antonio S. Evaluation of results with three-point visualization of zygomaticomaxillary complex fractures. Oral Surg Oral Med Oral Pathol. 1995; 80 (6): 624-628.
18. Kim ST, Go DH, Jung JH, Cha HE, Woo JH, Kang G. Comparison of 1-Point Fixation With 2-Point Fixation in Treating Tripod Fractures of the Zygoma. J Oral Maxillofac Surg. 2011: 69(11): 2848-2852.
|