INTRODUCTION
The success of root canal therapy depends upon the knowledge of root canal anatomy, the method and quality of instrumentation, the type of irrigant used and the three dimensional obturation of the root canal.7 During instrumentation a superficial layer of about 1 to 2 μm thickness and penetration depth of 40 μm in the dentinal tubule is formed11. This layer which consists of inorganic dentinal tissue and organic pulpal tissue along with microorganisms is termed
as smear layer8. Due to its loose bounding nature and permeability to bacteria along with its dissolving nature, it has been an issue of controversy over its presences in the root canal during obturation 4, 12. Its presences act as a natural barrier and its removal leads to bacterial invasion of the dentinal tubules in case the apical seal fails1, 4. Were as its presence on the root canal wall acts as an immediate physical barrier and interfere with the adhesion and penetration of the root canal sealer5, 6, 16, 22.
Today it is believed that instead of completely removing the smear layer, modifying it is beneficial. Many materials have been used for this purpose. Recently, the use of 30% potassium oxalate and 4% Titanium fluoride has been put
forward for this purpose 2, 11. In this study we hypothesize that the use of 4% Titanium Fluoride modifies the smear layer
and increases its sealing ability. So the aim was to evaluate the sealing ability of 4% Titanium Fluoride modified smear layer to the root canal wall using SEM.
MATERIALS AND METHOD
Twenty extracted maxillary central incisors were used in the study. Teeth were extracted from healthy patients who were advised extraction due to prosthetic and periodontal reasons. The samples were stored in formalin till further use. Access opening was made using a No.4 carbide round bur. Working length was established 1mm short of the apex and cleaning and shaping was carried out till 60 size K file following standard endodontic technique as described by Grossman. The samples were then divided into two groups. Group A experimental group with a sample strength of 10
and Group B control group with 10 samples. For Group A 4% titanium fluoride (TiF4) was freshly prepared by dissolving 3.4 gms of TiF4 in 100 ml of demonized distill water. And irrigation was carried out in all the 10 samples for group B
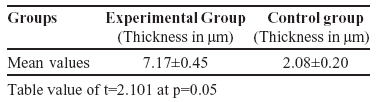
samples were left unirrigated to serve as control. All the teeth were grooved longitudinally on the facial and palatal surfaces, with a safe sided diamond disc and later were split half carefully using a chisel and mallet. The specimens prepared on the safe side of disc were used for the study. All the selected specimens were dehydrated by using ascending grades of ethanol. The specimens were then vacuum dried and were sputter coated with gold for examination under SEM. The samples were photographed under SEM and thickness of smear layer was measured at three different levels i.e. minimum, intermediate and maximum using computer software. Length of smear plug inside the dentinal tubule was measured and statistical analysis was carried out using tukey t test.Results Average of the thickness of the smear layer in the experimental group was found out to be 7.17±0.45 μm, were as in the control group the average thickness was 2.08±0.20 μm. The data obtained reviled that the thickness of smear layer increases with the use of 4% TiF4 for 1 min.
DISCUSSION
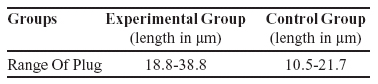
An important determinant of the success or failure of conventional endodontic therapy is the presence or absence of microleakage at the obturating material and the canal wall interface. The deterrent present between them is smear layer3, 7, 12, 14. Smear layer is a nonhomogeneous, non adherent, granular structure which is formed during instrumentation3. It is typically 1-2μm thick and penetrates the dentinal tubules to a depth of 7-40 μm8. Smear layer acts as a natural barrier to bacteria and bacterial products to entre from root canal into the dentinal tubules4. A success rate of 95% has been achieved in endodontic treatments without the removal of smear layer3. Also removal of smear layer has also been advocated by few others owing to its loose binding nature and solubility by bacteria12. But it is practically not possible to remove the smear layer completely due to the anatomical complexity of the root canal. Different materials like citric acid and potassium oxalate has been used without much success11, 13. Today the concept has shifted to modify smear layer instead of removing it or leaving it as it is. Material like TiF4 forms tenacious titanium rich coating on Enamel/Dentin/Cemental surface after a brief application period and this coating is stable and acid resistat10, 15, 17, 18, 21. This makes titanium fluoride a favorable material for modifying smear layer. The photomicrographs of the study samples reveled that there is massive thick layer of titanium dioxide on the root canal walls occluding the dentinal tubules along with a modified smear layer and smear plugs in the dentinal tubules. This can be explained by the fact that titanium is a polyvalent metal ion that has an inorganic complex binding ability which forms a tenacious TiO2 rich coating following the treatment with TiF4 on the tooth structure2, 10, 18, 19, 20. In the root canal walls bonding is carried in between hydroxyapatite or the sealers used and titanium due to its high affinity toward the oxygen atom present in the tubular structure or the oxide, carbonate, sulfate and borate groups of the sealers commonly used9, 19. Present study also revel an increase in the depth of penetration of the modified smear plug to about 18.8 - 38.8 μm. were as in the control group the depth of penetration ranged from10.5 – 21.7 μm only. This increase in the depth of
Table 1: Smear layer thickness
Table 2: Length of Smear plug
Average of the thickness of the smear layer in the experimental group was found out to be 7.17±0.45 μm, were as in the control group the average thickness was 2.08±0.20 μm. The data obtained reviled that the thickness of smear layer
increases with the use of 4% TiF4 for 1 min.
DISCUSSION
An important determinant of the success or failure of conventional endodontic therapy is the presence or absence of microleakage at the obturating material and the canal wall interface. The deterrent present between them is smear layer3, 7, 12, 14. Smear layer is a nonhomogeneous, non adherent, granular structure which is formed during instrumentation3. It is typically 1-2μm thick and penetrates the dentinal tubules to a depth of 7-40 μm8. Smear layer acts as a natural barrier to bacteria and bacterial products to entre from root canal into the dentinal tubules4. A success rate of 95% has been achieved in endodontic treatments without the removal of smear layer3. Also removal of smear layer has also been advocated by few others owing to its loose binding nature and solubility by bacteria12. But it is practically not possible to remove the smear layer completely due to the anatomical complexity of the root canal. Different materials like citric acid and potassium oxalate has been used without much success11, 13. Today the concept has shifted to modify smear layer instead of removing it or leaving it as it is. Material like TiF4 forms tenacious titanium rich coating on Enamel/Dentin/Cemental surface after a brief application period and this coating is stable and acid resistat10, 15, 17, 18, 21. This makes titanium fluoride a favorable material for modifying smear layer. The photomicrographs of the study samples reveled that there is massive thick layer of titanium dioxide on the root canal walls occluding the dentinal tubules along with a modified smear layer and smear plugs in the dentinal tubules. This can be explained by the fact that titanium is a polyvalent metal ion that has an inorganic complex binding ability which forms a tenacious TiO2 rich coating following the treatment with TiF4 on the tooth structure2, 10, 18, 19, 20. In the root canal walls bonding is carried in between hydroxyapatite or the sealers used and titanium due to its high affinity toward the oxygen atom present in the tubular structure or the oxide, carbonate, sulfate and borate groups of the sealers commonly used9, 19. Present study also revel an increase in the depth of penetration of the modified smear plug to about 18.8 - 38.8 μm. were as in the control group the depth of penetration ranged from10.5 – 21.7 μm only. This increase in the depth of penetration is well explained as when TiF4 is mixed with distilled water it reacts to form Hydrofluoric acid. This acid formed results in
etching of the dentinal tubules leading to increase in the penetration of the smear plugs18. Thus within the confirms of this study it can be conclude t hat 4% TiF4 when used as an irrigant modifies the smear layer to a composite and
resistant structure that occludes the dentinal tubules to deeper depth. This study strongly recommends the use of 4% TiF4 as an irrigant before obturating the root canals.
REFERENCES
1. Akpata E S, Blechman H. bacterial invasion of pulpal dentinal wall in vitro. J Dent Res 1982; 61(2): 435-8
2. Buyukyilmaz T, Ogaard B, Rolla G. The resistance of titanium tetra fluoride treated human enamel to strong
hydrochloric acid. Europ J Oral Sci 1997; 105: 473-7
3. Czonstkowsky M, Wilson E G, Holstein F A. The smear layer in endodontics. Dent Clin Of North Amer 1990; 34(1):
13-25
4. Drake D R, Wiemmann A H, Rivera E M. Bacterial retention in canal walls in vitro: Effect of smear layer. J Endod 1994;
20(2): 78-80
5. Gencoglu N, Samani S, Gunday M. Evaluation of sealing properties of thermafil and ultrafil techniques in the absence
and presence of smear layer. J Endod 1992; 19(12): 599-603
6. Gencoglu N, Samani S, Gunday M. Dentinal wall adaptation of thermoplasticised gutta percha in the absence or presence of smear layer. A SEM study. J Endod 1933; 19(11): 558-562
7. Lester K S, Boyde A. scanning electron microscopy of instrmented, irrigated, filled root canals. Brit Dent J 1977; 43:
359
8. Mader C L,Baumgartner C, Donald D P. scanning electron microscope investigation of the smeared layer on root canal walls. J Endod 1984; 10(10): 477-83
9. Mc Cann H G. The effect of fluoride cmplex formation on fluoride uptake and retention in human enamel. Archs Oral
Bio 1969; 14: 521-31
10. Mundorff S A, Marguerite , Little F, Bibby B G. Enamel dissolution: II action of titanium Fluoride. J Dent Res 1972;
51(6): 1568-71
11. Pashley D H, Galloway S E. The effect of oxalate treatment on the smear layer of ground surface of human dentine. Archs Oral Bio 1985; 1985: 731-7
12. Pashley D H. Clinical consideration of microleakage. J Endod 1990; 16(2): 70-7
13. Seltzer S. basic considerations in endodontic procedures. Endodontology second Edition Pg. No. 256
14. Sen B h, Wesselink P R, Turkman M. The smear layer: a phenomenon in root canal therapy. Int Endod J 1995; 29:
141-8
15. Skartveit L, Tveit A B, Klinge B, Totdal B, selvig K A. in vivo uptake and retention of fluoride after a brief application
of TiF4 to dentin. Acta Odont Scand 1989; 47: 65-8
16. Timpawat S, Sripanaratanakul S. Apical sealing ability of glass ionomer sealer with and without smear layer. J Endod
1998; 24(5): 343-6
17. Tveit A B, klinge B, Totdal B, Selving K A. Long term retention of TiF4 and SnF2 after topical application on dentin
in dogs. Scan J Dent Res 1988; 4: 265-70
18. Tveit A B, Hals E, Isrenn R, Totdal B. Highly acidic SnF2 and TiF4 solutions: effect and chemical reactions with root
dentin in vitro. Caries Res 1983; 17: 412-8
19. Tveit A B, Totdal B, Klinge B, Nilvnus R, Selvig K A. Fluoride uptake by dentin surfaces and following topical
application of TiF4, NaF and fluoride varnishes in vivo. Caries Res 1985; 19: 240-7
20. Wefel J S, Harless J D. The effect of topical flupride agents on fluoride uptake and surface morphology. J Dent Res 1981; 60(11): 1842-8
21. Wei S H Y, Soboroff D M, Wefel J S. Effect of titanium tetrafluoride on human enamel. J Dent Res 1976; 55(3): 1568-
71
22. White R R, Goldman M, Lin R K S. The influence of the smeared layer upon dentinal tubule penetration by plastic filling materials. J Endod 1984; 10(12): 558-62 |