Introduction
In the past, extraction was the only option available to children suffering from tooth ache. With the passage of time and evolution of paediatric endodontic, there has been a paradigm shift towards maintenance and preservation of tooth in an infection free state.[1]
Pulp treatment of deciduous and young permanent teeth has seen revolutionary changes with the advancements made both in technique and materials. [2], [3]
Preservation of primary teeth till the eruption of permanent teeth is desirable since they help to determine the shape of dental arches, maintain the space between teeth, prevent detrimental tongue and speech habits, preserve aesthetics and maintain chewing function.[4]
The aim of pulp therapy in the primary dentition is to retain the primary tooth as a functional part of the dentition for mastication, phonation, swallowing and the preservation of the space required for the eruption of the permanent tooth.[5]
Endodontic treatment can be done in both primary and permanent teeth. Pulpectomy is preferred treatment in primary teeth. The thin, tortuous and branching path of the pulp filaments in the primary molar precludes the possibility of complete removal of all radicular pulp. Therefore in a primary molar partial pulpectomy is termed over RCT.[6],[7]
Traditional cleaning and shaping techniques employing hand instruments have a variety of steps, depend on the clinician’s skill, and are often complex and time consuming. Recently, nickel titanium instruments has been introduced because of their superiority, compared to traditional stainless steel endodontic files with regard to elasticity and resistance to torsional fracture.[8]
Various systems of rotary instruments are available i.e.; Protaper, Hyflex file systems. Protaper instruments have a convex triangular cross-section which is claimed to reduce the contact area between the file and dentin.[9], [10], [11], [12] The patent progressive taper and advanced flute design provides flexibility and efficiency to achieve consistently successful cleaning and shaping results.[13] Protaper system consist of one file as an orifice opener (SX), two shaping files (S1, S2) and five finishing files (F1-F5). A crown down technique is recommended for protaper instruments, in which larger files are used before smaller ones and canals are prepared with a coronal to apical approach.[14]
Recently, a new Nitinol file system with controlled memory (CM) has been introduced (HyFlex rotary file). The purpose of this new rotary file is to simplify root canal treatment and to optimize cleaning and shaping of the canal. This system also offers precise apical finishing, leaving the structural integrity of the root intact after endodontic therapy.[15]
This study has been undertaken with the purpose to evaluate the cleaning efficiency of rotary NiTi files (Protaper, HyFlex) and manually used K-files in primary and permanent root canals. Moreover, another purpose was to assess the time taken for preparing primary and permanent root canals by both rotary and manual techniques.
Materials and methods
The present study was conducted at the Department of Pedodontics and Preventive Dentistry, Himachal Institute of Dental Sciences, Paonta Sahib (H.P) with the objective to assess the difference in the cleaning efficiency and instrumentation time of manual K-files, rotary ProTaper and HyFlex in the cleaning of root canals in primary and permanent molars.
The study was conducted on thirty primary and thirty permanent teeth. The primary molars indicated for extraction, but with at least two-third roots remaining were chosen for the study. Examples of such teeth are as follows:
Infected primary molars with considerable bone loss.
Over retained primary molars with altered root resorption pattern.
Primary molars with distal and palatal root resorbed more than the other, due to the altered path of eruption of its successor.
Infected primary molars with chronic recurrent infection.
 | Sample Teeth
 |
Collection of teeth and their storage:
Freshly extracted teeth were washed under running water and all the soft tissue was scrapped off with a hand scaler to remove the tissue remnants attached to it and teeth were then stored in formalin in different containers.
Selection of Root canals for the study:
The distribution of root canals is done with the purpose of maintaining standardization of using both techniques of root canal cleaning in root canals and to obtain simplicity while analyzing the root canals for the presence of dye after clearing of the teeth.
Method of root canal preparation:
• Coronal access cavity was prepared with a large round bur. As the pulp chamber was reached, roof of the pulp chamber was removed to gain access to the root canals. All the overlying dentin was removed with tapered bur to achieve a straight line access into the root canals.
• The pulp chamber and root canals were irrigated profusely with saline to remove the debris.
• Then a # 10 sized K-file was introduced into each root canal to determine the patency of the root canal. If the patency could not be established in either of the canals, then the tooth was replaced with another one of the same arch.
• Working length determination: As the # 10 file was introduced into the root canal, the tip was visualized using magnifying glass. The final working length was established 1mm short of this recorded length.
• Then the teeth were mounted in the dental plaster, to carry on with an unbiased procedure for cleaning the root canals. Care was taken to mount the teeth only till their CEJ, exploring their crown portions only.
• India ink dye was then injected in each root canal by using Insulin syringe. The ink was reapplied at least three to four times into the root canals.
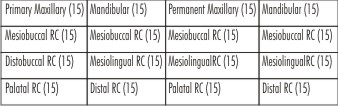
The root canals were then divided into four groups:
Group I: Twenty teeth [10 primary (5 maxillary & 5 mandibular) teeth] and [10 permanent (5 maxillary & 5 mandibular) teeth] with forty root canals were instrumented with K-files up to # 30 file and then stepped back to # 35 and # 40 file.
Group II: Twenty teeth [10 primary (5 maxillary & 5 mandibular) teeth] and [10 permanent (5 maxillary & 5 mandibular) teeth] with forty root canals were instrumented with ProTaper.
Group III: Twenty teeth [10 primary (5 maxillary & 5 mandibular) teeth] and [10 permanent (5 maxillary & 5 mandibular) teeth] with forty root canals were instrumented with Hyflex.
Group IV: Sixty root canals were chosen as Control group and not instrumented. For control group, distal and palatal root canals in mandibular and maxillary teeth which were not instrumented with either technique were chosen and injected with India ink dye.
• In groups I, II and III the root canals were instrumented by only one operator, to eliminate the variations caused by individual efficiency and knowledge of cleaning of root canals by the techniques.
• After each instrument change, each root canal was irrigated with saline solution in 3ml quantity.
• The instrumentation time in each root canal was measured by a stop watch during each technique. The time for instrumentation was recorded by trained operator as the first file got into the canal until the instrumentation finished.
• The instrumented teeth were then taken out of the mounting and coronal pulp chamber and apical ends were sealed with a sticky wax. This helped to eliminate the errors that could have been caused by the action of the clearing agent (i.e. Methyl salicylate) or others chemicals used for processing on the dye removal from the root canals.
Method of decalcification of teeth:
The teeth were decalcified in 10% nitric acid solution. The teeth were observed timely and the acid was renewed every 24 hours to maintain its efficiency in decalcifying the teeth. Freshly prepared acid was always used for the renewal.
The teeth were kept in acid till they were completely.
Method of Dehydration of teeth:
• Once teeth were completely decalcified, they were washed under running water for eight hours, till the acid completely got washed away from the tooth surface.
• Then the teeth were kept in freshly prepared 70% alcohol for sixteen hours and the solution was changed after eight hour.
• Then the teeth were kept in 90% alcohol for 3 hours and the solution was changed after every one hour.
• After that, the teeth were kept in absolute alcohol for 3 hours and the solution was changed after every one hour.
Method of Clearing of teeth:
• After decalcification and dehydration, the teeth appeared more opaque or whitish in colour. Then they were kept in methyl salicylate, till they started appearing transparent and clear.
• It took nearly 2-3 hours for teeth to get completely cleared.
• The teeth then onwards remained in the methyl salicylate solution at all times; to avoid any change of loss of their transparency.
Analysis of the root canals:
After the teeth appeared clear, they were observed under a Stereomicroscope (Alco, India) at 10X magnification. Each root canal was inspected carefully for the removal of India ink from the cervical, middle and apical thirds. The removal of the dye was analyzed from all the walls of the root canal and scored.
Scoring criteria given to each root canal are: (By Silva LA) [16]
Score 0: Total cleaning (No ink remaining in any part of root canal)
Score 1: Almost complete ink removal (Traces of ink found in some areas)
Score 2: Partial ink removal (Ink found on some walls in some areas)
Score 3: No ink removal (Appreciable amount of ink present)
Statistical Analysis:
1. The data obtained was subjected to statistical analysis using SPSS (Statistical package for social Sciences)
2. The scores obtained were analysed with Chi-Square test
3. The time taken for instrumentation was statistically analysed with t-test.
Results
The present study revealed that there is a statistically significant better cleaning efficiency of K-file and Hyflex in middle third and K-file in apical third between the primary and permanent teeth.
The cleaning efficiency of three instruments (Kfile, ProTaper and Hyflex) in coronal 1/3rd, middle 1/3rd and apical 1/3rd of primary teeth and permanent teeth revealed that Hyflex performed better in all the segments but did not show any statistical significance. Instrumentation time taken with ProTaper was longer in both maxillary (8.132 min SD=0.790) and mandibular permanent teeth (8.592 min SD=1.722) whereas Hyflex took shorter instrumentation time for preparing both maxillary (6.992 min SD=1.026) and mandibular permanent root canals (6.916 min SD=0.663).
In primary teeth, Hyflex took shorter instrumentation time for preparing both maxillary (4.026 min SD=0.245) and mandibular root canals (3.890 min SD=0.665).
When comparing Manual K-file with ProTaper instruments in terms of instrumentation time, K file took lesser time in both primary and permanent root canals than ProTaper but their difference is not statistically significant.
Instrumentation time between K-file and Hyflex techniques revealed significant difference between two instrumentation techniques in primary root canals but no difference in permanent teeth.
Time taken during instrumentation between ProTaper and Hyflex techniques revealed significant difference between two instrumentation techniques in primary and permanent root canals.
Discussion
Endodontic therapy is a sequence of treatment for the infected pulp of a tooth which results in the elimination of infection and the protection of the decontaminated tooth from future microbialinvasion.[17] The cleaning and shaping is an important part of this treatment[18] and this step determines the success of the successive step.
Over the years the varieties of instruments and techniques have been proposed for root canal preparation. Changes have evolved in the instrumentation of root canals in the metallurgy, instrument taper and the method of use of the endodontic instruments.[19]
Carbon steel files were used earlier and after that the era of stainless steel files evolved that brought in files that were more flexible and less brittle than carbon steel files.[20] However presently flexible nickel-titanium files dominate the field of endodontic instrumentation.
The literature suggests that chemical means as the effective adjunct of cleaning of root canals in primary teeth, as the mechanical instrumentation could be injurious to the succedaneous tooth bud in cases of over instrumentation of root canals beyond the apex.[19], [21]
Recent literature suggests that the value of mechanical cleaning cannot be overlooked and the chemo-mechanical means is the most effective way to debride the root canals in primary and permanent teeth.[19] The chemical means are used in conjunction with mechanical debridement, to disinfect and remove necrotic material within the somewhat inaccessible canals, rather than “shaping” of the canals.[22]
In the mandibular teeth, only the mesial root canals were prepared with K-file, ProTaper and Hyflex. This was done as the distal roots in mandibular molars shows maximum variation in the occurrence of single and two canals.[23] The literature suggests that 93.33% mandibular 1st primary molars have 2 mesial canals and 2 distal canals, whereas, 100% mandibular 2nd primary molars show 2 mesial canals and 53.3% have 2 distal canals. Also mandibular primary molars show maximum angulation in the mesial root (34.4-36.2 degrees) [23], [24] The difference in the angulation of mesiobuccal and mesiolingual canals is not great.
In the maxillary teeth, only mesiobuccal and distobuccal roots were instrumented with the techniques. These two roots have found to show similar curvature of their root canals, whereas the diameter and angulations both are variable for the palatal roots.[24], [25]
The control groups in the study were prepared in order to confirm the proper penetration of India ink into the root canals of primary and permanent teeth, because of their hour glass shape. All the uninstrumented root canals, i.e. mandibular distal root canals and maxillary palatal root canals were treated as ‘controls’. The ink injection method used in the study followed the methodology given by Silva A B Lea et al.[16]
In the present study, ProTaper and Hyflex was used in the Crown down approach. Davis et al (2002)[91] stated that flaring the coronal portion of the root canal before instrumenting the apical region was beneficial as it increases mechanical efficiency of the instrument and provide better access to the apical portion. Roland et al (2002) and Peters et al (2003) [26], [27] stated that coronal preflaring reduced the risk of stress and binding along the canal wall that could contribute to instrument failure and separation.
The results showed that total dye removal from the interior of the root canals and consequent complete cleaning were not achieved by any of the instrumentation techniques. The results of this study are in agreement with the result of Tan BT et al (2002)[28] who observed that both the manual and rotary techniques do not allow complete root canal cleaning in permanent teeth. In addition, the results were in agreement with the results of Ahluqist M et al 2001[29] that compared the two techniques of canal preparations, and concluded that manual technique produced cleaner root canal walls than the rotary ProFile technique.
Some studies have reported the advantages of manual instrumentation over rotary files regarding root canal wall preparation. Barbizam JV et al 2002[30] who compared manual K-file and rotary profile instrument neither of the techniques was completely efficient in cleaning the apical thirds of the roots, but manual technique showed more efficient cleaning in mesial-distal flattened root canals than rotary technique. However, others have reported better results with rotary NiTi systems (Guelzow A et al 2005).[31]
In the present study, the results showed increased instrumentation time taken with the use of ProTaper (9.844 min in primary root canals and 16.724 min in permanent root canals) whereas it took lesser time with Hyflex (7.916 min in primary root canals and 13.908 min in permanent root canals) and it is statistically significant in both primary and permanent teeth. This was in contrast with the results obtained by Capar I D et al (2014)[32] in which Hyflex took lesser instrumentation time than the other files system, which was carried out in permanent teeth.
However, preparation time in primary teeth with K-file, ProTaper and Hyflex was shorter than in permanent teeth, possibly due to the shorter root length in primary teeth.
As per the results obtained in the study, considering the cost and time taken by rotary files in cleaning the root canals, their use can be questioned in primary teeth. But the combined use of manual and rotary files in the cleaning of root canals in primary molars can be considered a valuable and better option for the biomechanical preparation of root canals.
The study was worth doing in the extracted molars, as they provide more reliability of results compared with artificial resin canals.
Conclusion
Clearing of teeth can be used as an effective means of studying the cleaning efficiency of K-files, ProTaper & Hyflex files in root canals of primary & permanent molars. There was a statistically significant difference in the cleaning efficiency of K-file & ProTaper in the apical & middle thirds of the root canals between primary & permanent root canals. The difference in instrumentation time taken with K-file, ProTaper & Hyflex was higher for ProTaper in both primary & permanent root canals & least for Hyflex but found to be not significant.
References
1. Fuks AB.Vital pulp therapy with new materials for primary teeth: new directions and treatment perspectives. J Endod 2008;34(7 Suppl):s18-24.
2. Camp JH. Diagnosis dilemmas in vital pulp therapy: treatment for the toothache is changing, especially in young, immature teeth. Pediatr Dent 2008;30(3):197-205.
3. Bhatti N, Sroa R, Sikri VK. Evaluation of surface preparation and maintenance of canal curvature following instrumentation with hand ‘K’ file and three different Ni-Ti rotary systems: A radiographic and SEM study. Contemp Clin Dent 2010;1(2):88-93.
4. Caicedo R, Abbott PV, Alongi DJ, Alarcon MY. Clinical, radiographic and histological analysis of the effects of mineral trioxide aggregateused in direct pulp capping and pulpotomies of primary teeth. Aus Dent J 2006;51(4):297-305.
5. Vieyra JP, Enriquez FJJ. Instrumentation Time Efficiency of Rotary and Hand Instrumentation Performed on Vital and Necrotic Human Primary Teeth: A Randomized Clinical Trial Dent 2014;4(4):1-5.
6. Frankl SN. Pulp therapy in pedodontics. Oral Surg Oral Med Oral Pathol 1972;34(2):293-309.
7. Curzon MEJ, Roberts JF, Kennedy DB. Paediatric operative dentistry. 4th edition; page No. 143-44.
8. Zamiran S, Jahromi MZ, Fathi M, Moghaddam G. An in-vitro study on cleaning efficiency of Mtwo and BioRace rotary nickel-titanium instruments. Health 2013;5(12): 2045-50.
9. J Crumpton LB, McClanahan S. Endodontic rotary nickel titanium instruments systems. Clin Update 2003;25(8):15-7.
10. Kim JW, Park JK, Hur B, Kim HC. Comparison of shaping ability using various Nickel-Titanium rotary files and hybrid technique. J Kor Acad Cons Dent 2007;32(6):530-41.
11. ES Hong, Park JK, Hur B, Kim HC. Comparison of shaping ability between various hybrid instrumentation methods with ProTaper. J Kor Acad Cons Dent 2006;31(1):11-19.
12. Vahid A, Roohi N, Zayeri F. A comparative study of four rotary NiTi instruments in preserving canal curvature, preparation time and change of working length. Aust Endod J 2009; 35(2): 93-7.
13. Azar MR, Safi L, Nikaein A. Comparison of the cleaning capacity of Mtwo and ProTaper rotary systems and manual instruments in primary teeth. Dent Res J 2012; 9(2): 146-51.
14. Caicedo R, Clark SJ. HyFlex CM rotary files: an excellent innovation for endodontic treatment. Endodontic practice 4(6).
15. Wu MK, Wesselink PR. Efficacy of three techniques in cleaning the apical portion of curved root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79(4):492-6.
16. Silva LA, Leonardo MR, Filho PN, Tanomaru JMG. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child 2004;71:45-7.
17. Cohen Stephen, Burns C Richard. Pathways of the pulp. 9th ed, Mosby.
18. Pedrazzi V, de Oliveira- Neto JM, Sequeira P, Fedorowicz Z, Nasser M. Hand and ultrasonic instrumentation for orthograde root canal treatment of permanent teeth. J Appl Oral Sci 2010;18(3):268-72.
19. Musani I, Goyal V, Singh A, Bhat C. Evaluation and comparison of biological cleaning efficacy of two endofiles and irrigants as judged by Microbial Quantification in primary teeth- an in-vivo study. Int J Clin Pediatr Dent 2009;2(3):15-22.
20. Abhilesh, Menusdar R, Vivekandhan, Subbiyat, Sukumaran VG.Cutting efficiency, surface change and hardness: EZ Fill safe sider instruments vs K files. Indian J Multidisciplinary Dent 2011;1(2):110-14.
21. Forrester DJ, Wagner ML, James F.Pediatric dental medicine. Lea and Fabringer Co, Philadelphia, 1981, 324–340.
22. Ingle IJ, Bakland KL. Endodontics. 4th ed, “Pediatric Endodontics”. Kopel HM, Chap 19, 857.
23. Madan N, Rathnam A, Shigli AL, Indushekar KR. K-files vs profiles in cleaning capacity and instrumentation time in primary molar root canals. J Indian Soc Pedod Prev Dent 2011;29(1):2-6.
24. Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod 2004;30(8):559-67.
25. Zoremchhingi, Joseph T, Varma B, Mungara J. A study of root canal morphology of human primary molars using computerised tomography: an in vitro study. J Indian Soc Pedod Prev Dent 2005;23(1):7-12.
26. Roland DD, Andelin WE, Browning DF, Hsu GH, Torabinejad M. The effect of preflaring on the rates of separation for 0.04 taper nickel titanium instruments. J Endod 2002;28(7):543-5.
27. Peters OA, Peters CI, Schonenberger K, Barbakow F. ProTaper rotary root canal preparation: assessment of torque and force in relation to canal anatomy. Int Endod J 2003;36(2):93-9.
28. Tan BT, Messer HH. The quality of apical canal preparation using hand and rotary instruments with specific criteria for enlargement based on initial apical file size. J Endod 2002;28(9):658-64.
29. Ahlquist M, Henningsson O, Hultenby K, Ohlin J. The effectiveness of manual and rotary techniques in the cleaning of root canals: a scanning electron microscopy study. Int Endod J 2001;34:533-37.
30. Barbizam JVB, Fariniuk LF, Marchesan MA, Pecora JD, Sousa-Neto MD. Effectiveness of manual and rotary instrumentation techniques for cleaning flattened root canals. J Endod 2002;28(5):365-6.
31. Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J 2005;38(10):743-52.
32. Capar ID, Arslan H, Akcay M, Ertas H. An in vitro comparison of apically extruded debris and instrumentation times with ProTaper universal, ProTaper next, Twisted file adaptive, and Hyflex instruments. J Endod 2014;40(10):1638-41.
|