Introduction
Success in endodontics has always been a challenge for the operator. Whenever a tooth in question requires endodontic therapy, the variation in root canal anatomy poses a great problem in realizing and managing the canal spaces. Mandibular premolars are one of the most difficult teeth to treat endodontically because of the variations in rootcanal anatomy. There are only a few endodontic publications citing an incidence of mandibular 2nd premolar
with 3 root canals.Knowledge of basic root and root canal morphology as well as possible variation in anatomy of the root canal system is important in achieving successful nonsurgical root canal treatment (NSRCT)[1]. This is followed by negotiation, cleaning and shaping and obturation of the entire canal system in 3 dimensions. Most mandibular second premolars have a single root. According to El-Deeb (1982)[3] the mandibular premolars may show wide variation in their root canal anatomy.The incidence of 2 or more roots is low at approximately 0.4%[5]. The incidence of 2 or more roots in the mandibular first premolar is 2.1%[2]. Zillich and Dowson[8] in 1973 have reported an incidence of 0.4% of mandibular second premolars with three canals. Vertucci[7] does not report any case of mandibular second premolar with three or more canals at the apex. The incidence of three roots is extremely rare (0.1%). Such anatomic variations are quite possible and shouldn’t be thought of as exceptional. The purpose of this article was to describe the successful endodontic treatment of mandibular 2nd premolar with 3 root canals.
Case Report
A 35 Yr old asthmatic male reported to our clinic with chief complaint of pain in “right lower back region”. The tooth was tender on percussion and painful on palpation. A preoperative radiograph of the involved tooth was done. It revealed distally carious pulp exposure (Fig No. I).
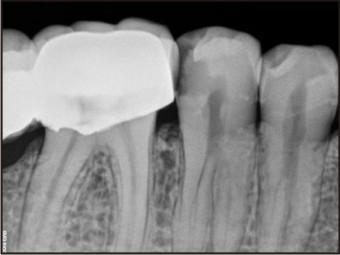 | Fig No. I
 |
Two- visit nonsurgical endodontic treatment was planned with Calcium hydroxide/Iodoform (MetaPex) as intracanal medicament. The access cavity preparation was established. Three canals were located, two buccally and one lingually. Gates Glidden drills were used in a crown down method to enlarge the main orifice to the level of trifurcation for a straight line access to all the three canals. The working length was established radiographically using Ingle’s method. The canals were conventionally instrumented using iRaCe (FKG DENTAIRE) 0.04 taper no 25 rotary files (Fig No. II) with RC Prep, irrigated with 5.25% Sodium Hypochlorite solution (Septodont) dried with sterile paper points and sealed with calcium hydroxide/Iodoform paste. The access opening was closed with Cavit (Dentsply). Antibiotics along with analgesics and anti-inflammatory drugs were prescribed for 3 days.The patient returned asymptomatic after 1 week, the canals were irrigated with 5.25% sodium hypochlorite to remove all the remnants of the calcium hydroxide, and then dried with paper points (Dentsply). Master cone was selected and the canals were filled with gutta-percha (4% META) and Resino-seal as resin based sealing agent (Ammdent). Access opening was sealed with glass ionomer cement (Fujji Type II). Post-operative radiograph was taken to confirm the quality of the filling and the tooth was subsequently crowned (Fig No. III).
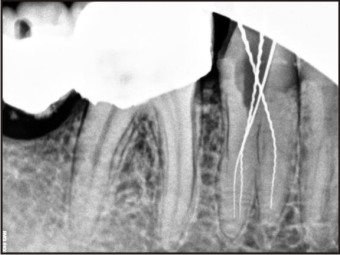 | Fig No. II
|
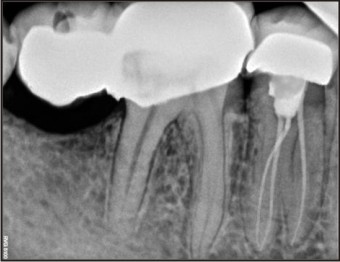 | Fig No. III
|
Discussion
The complex nature of root canal morphology of mandibular second premolar should not be underestimated. Good quality radiographs taken at two different horizontal angulations are very helpful in providing clues about the number of root canals a tooth can have[6]. Interpretation of the radiographs is equally important. The root canals may not be evident radiographically. Sudden narrowing or a disappearing pulp space may indicate the presence of another canal or canals. Careful interpretation of the PDL space helps in finding extra roots or canals[4]. However, because of the superimposition of roots, radiographic diagnosis of three canals is not possible in all the cases. In the present case, the radiographic features suggested the possibility of three canals. An optimum access cavity is absolutely necessary. Smaller K files (6, 8, 10) are initially used as they get deviated buccally or lingually as the main canal divides at the midroot level. So a good tactile sense is important and the files can be precurved appropriately before negotiating the canals. Despite the existence of complex dental anatomy, shaping outcomes with nickel titanium instruments are mostly predictable. Efforts should be made to locate the point where the root or the canals divide. The more apically a root canal divides, the more difficult is the case. Many authors who located orifices in pulp chamber of lower second premolar reported one orifice in the lingual side and two in the buccal side. It is assumed that careful observation and inspection of the pulpal floor and also pulpal wall is necessary to avoid the unexpected missing of orifices that may cause unsuccessful endodontic treatment.
References
1. Al-Attas H, Al-Nazhan S. Mandibular second premolar with three root canals : Report of a case. Saudi Dental Journal 2003;15(3), 145-147.
2. Cleghorn BM, Christie WH, Dong CCS. The root and root canal morphology of human mandibular second premolar: A literature review.
3. ElDeeb M.Three root canals in mandibular second premolars. Literature review and case report. Journal of Endodontics, 1982; 8:376-377.
4. Mittal N, Arora S. Endodontic treatment of mandibular second premolar with three root canals using operating microscope. Endod; 80-83.
5. Sikri VK, Sikri P. Mandibular premolars: aberrations in pulp space morphology.Indian J Dent Res 1994;5:9 –14.
6. Tyagi S, Arjun Das KP, Bhagwat SP. Endodontic Enigma- Mandibular Second Premolar with three root canals- A case report
7. Vertucci F. Root canal morphology of the mandibular premolars. JADA 1978;94:47-50.
8. Zillich R, Dowasn J: Root canal morphology of mandibular first and second premolar. Oral Surgery, 1973; 36:738-744.
|