Introduction:
Due to extractions and loss of teeth and periodontal structures there is lack of stimulation leading to a continuous ridge resorption, leading to a poor denture foundation. In order to delay bone resorption post extraction or loss of teeth, preventive measures that emphasize the importance of any procedure that can delay or eliminate future prosthodontic problems are being encouraged. Moreover it is further emphasized the alveolar bone with its overlying mucosa was never intended to receive the full force of complete denture. The overdenture is a logical method for the dentist to use. This article presents a clinical case report of fabrication of mandibular overdenture retained by magnets. The method is new and innovative and also economical and time saving.
Case Report:
A 65 year old femalewas referred to the Department of prosthodontics at School of Dental Sciences. Krishna Institute of Medical Sciences Deemed University, Karad. Maharashtra, India. Requesting replacement of missing natural teeth. Clinical examination revealed partially edentulous maxillary and mandibular arch with few remaining natural teeth which were periodontally weak. After adjuvant radiographic evaluation (Fig 1), teeth with hopeless prognosis were removed. Periodontally favourable maxillary right first premolar, maxillary left first premolar ,maxillary left second molar , mandibular left first premolar, mandibular left first molar , mandibular right canine and mandibular right second molar were left intact to later on serve as overdenture abutments.
 | Figure:1 - Pre Operative Orthopantamograph
 |
Maxillary abutment teeth (14,24,27) received cast copings with posts, while Mandibular left first premolar(34), mandibular right canine(43) served as abutments in fabrication of mandibular magnet retained overdenture and the mandibular molars (36,47) served as support.
Clinical Procedure
a) 1. Preparation of mandibular root components: See Figures (2,3,4,5)
Abutment teeth (34 and 43) were endodontically treated and decoronated 2mm above free gingival margin , the surface of the teeth were smoothened and rounded to eliminate sharp margins with diamond rotary instruments (Mani, INC), followed by removal of twoR09;thirds of the root canal filling material with custom rotary drill instruments (Peasow reamer; Dentsply, York, Pennsylvania, USA)and Dyna Spiral Drill (Dyna Dental Magnet System , Netherlands)(stainless steel) to prepare the post space. The Dyna Seat Drill (Dyna Dental Magnet System , Netherlands)(stainless steel) for the final preparation of the post space so as to seat the post along with the keeper (Dyna EFM Alloy KeeperØ 4,8mm) (Dyna Dental Magnet System , Netherlands). The magnetic keeper attachments were then cemented on to the prepared roots with Glass Ionomer Cement (GC Co., Tokyo, Japan).
 | Figure:2 - Post Endodontic Treatment Of Abutment Teeth
|
 | Figure:3 - Post Space Preparation Of Mandibular Abutments
|
 | Figure:4 - Cemented Keeper Attachments
|
 | Figure:5 - Dyna Direct Dental Magnets,Custom Drills,Keeper Attachments
|
a) 2. Preparation of maxillary root components: See Figure (6)
Endodontically treated maxillary abutment teeth (14,24,27) were decoronated 2 mm above the free gingival margin. Post space preparation was carried out by removal of twoR09;thirds of the root canal filling material with a rotary drill instrument (Peasow reamer; Dentsply, York, Pennsylvania, USA) for cast copings with post extending upto 5mm in the root canal system. Elastomeric impression with polyvinyl siloxane impression materials (Aquasil, Dentsply International Inc., USA) to record the margin area and root post was successfully made and definitive cast (Ultrarock, type IV dental stone; Kalabhai Karson Ltd, Vikhroli (W), Mumbai, India)was fabricated. Indirect inlay wax (DFS-Diamon GmbH, Ländenstr. 1, D-93339 Riedenburg) was used to make impression of post space to fabricate the copings with posts (length of 5mm.) followed by cementation using glass ionomer cement. (GC Co., Tokyo, Japan).
 | Figure:6 - Maxillary Post Space Preparation Followed By Elastomeric Impression And Cast Post Ceentation
|
b) Preparation of Denture component:See Figures (7,8,9,10)
Preliminary impression of maxillary and mandibular arches were made using irreversible hydrocolloid impression material (Imprint, DPI, Mumbai, India) and cast prepared in dental plaster (Kalabhai Karson Pvt Ltd, Mumbai, India). Acrylic custom tray (DPI-RR Cold Cure, DPI,Mumbai,India)with wax spacer (Modelling Wax No 2, Deepthi Dental Products of India Pvt Ltd) was fabricated. An additional wax spacer of the dimension of denture magnet, about 3mm in diameter & 2 mm in thickness was placed over the root face on preliminary cast. Border moulding was done with low fusing compound (DPI Pinnacle Tracing Stick, DPI, Mumbai, India), wax spacer removed, relief holes were made with no 8 round bur and tray kept ready for definitive impression. Denture component magnet was placed facing the cemented root component magnet and definitive impression of maxillary and mandibular arches were made using Zinc oxide Eugenol impression paste (DPI Impression Paste, DPI, Mumbai). Set impression was removed from patient's mouth and inspected for defects (Fig 11). The denture magnet which got embedded within the impression was removed and master cast prepared in dental stone. The jaw relation was recorded and complete denture trial was done. Esthetics, phonetics, retention, stability and comfort were re-evaluated at the trial stage. Complete denture was then fabricated by conventional material and methods (DPI Heat Cure denture base resin, DPI, Mumbai). Finished complete dentures were tried in patient's mouth and kept ready for insertion
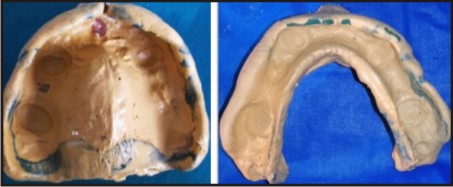 | Figure:7 - Maxillary And Mandibular Definitive Impressions.
|
 | Figure:8 - Jaw Relation Record
|
 | Figure:9 - Complete Denture Trial
|
 | Figure:10 - Complete Denture Insertion
|
 | Figure:11 - Dental Keeper And Denture Magnet
|
The tissue surface of mandibular complete denture which contained the cavity corresponding to the denture magnet was slightly enlarged and undercut created with inverted cone bur (SS Whit, New Jersey, U.S.A)to freely accommodate the magnet. Denture magnet (WR Magnet S5, Dyna Dental Magnet system, Netherlands) which were circular in shape and measure 3mm in diameter and 2 mm thick wereplaced facing the root magnet. Autopolymerising acrylic resin (DPI-RR Cold Cure,Mumbai, India) was mixed and placed into the cavity and complete denture inserted into patient's mouth and patient asked to occlude with minimal force to avoid displacement of magnets[13]. Complete denture was later removed from mouth, excess acrylic flash trimmed and removed. Finally finished and polished prosthesis was inserted into patient's mouth. Post insertion dos and don’ts & instructions concerning oral hygiene measures, follow up regimens and maintenance of abutment teeth were given to the patient.
Discussion:
In this article, fabrication of overdenture using magnets was discussed. Basically there are two types of magnetic systems namely open field and closed field systems.[1],[2],[3] Open field system involves two cylindrical magnets, one embedded in the denture and the other cemented to the root canal treated teeth which are decoronated at 1-2mm above the gingival margin.Initially, the repellent force of like magnetic poles were harnessed from open-field Al Ni Co alloys embedded in the base of upper and lower denture. However, this approach achieved little popularity because these open-field magnet systems corroded easily and their attractive force was weaker (mean of 2 N or less) than that of mechanical attachments used to retain dentures, such as ball or bar attachments. Inthe past couple of decades there has been introduction of alloys of the rare earth elements samarium (SmCo) and, more recently, neodymium (NdFeB) in closed-field systems. Rare-earth alloys produce a stronger and more stable magnetic force than was previously available because they have high magnetization and high resistance to demagnetization In the closed field system, the magnetic assembly consists of magnet with protective stainless steel end plates embedded in the denture and a ferromagnetic alloy (magnetisable keeper) cemented into the root. Also in closed-field systems, the magnetic field or flux is contained within the magnet–keeper unit and yields a much greater attractive force per unit size than is possible with open-field systems. The magnetic force permeates the closed-field system with much less resistance than occurs in the surrounding air. Therefore, the strength of magnetism or the “density of flux” is concentrated between the north and south poles of the magnet.
DYNA WR Magnets[4], [5], [6], [7], [8], [9], [10]
The main advantage of this system over the conventional magnetic systems was that there is no need for activation, Permanent stable retention, no impression or laboratory auxiliary elements, Parallelism is less necessary, Biocompatibility, rebasing procedure is the same as for a standard denture, very easy dental hygiene for the patient ,vertical load of the post elements, time saving, simple and very economical method. The procedure of crown decoronation, preparation of cavity to accommodate magnets, making impression of the prepared cavity, preparing working casts, modifying and cementing root component magnet and making definitive complete denture impression can be completed in one appointment on a short time span. More over by placing denturecomponent magnet over the keeper while making definitive impression creates an exact negative depression on the tissue surface of complete denture. These procedures eliminate the chance of alignment error between the approximating surfaces of both (right and left) magnets.
Shaping the magnet encapsulation in hardened surgical steel or titanium grade 5 and the use of latest laser lasing techniques (CAM Lathing machines) prevents any undesired leakages & makes them wear resistant.
General Contraindications
• Severe bruxism : When using the magnets for bruxers anyway, space must be created in such a way that only direct contact between magnet and keeper is realized when maximum bite forces are applied. It may be easily controlled by using fit checker material.
• Lack of patient motivation : careful considerations should be made while selecting and handling patients. Patients carrying a negative attitude towards the treatment can never be satisfied and appreciative of the dentist’s efforts.
• Poor dental hygiene : Because abutment teeth are easily accessible the patients are usually able to undertake adequate home care procedures for the maintenance of optimum state of health of the abutment teeth. Nevertheless certain patients with poor dexterity may have difficulty in doing so.
In a study conducted by Shannon and Cronin[17] concluded that frequent application of low concentration stannous fluoride to exposed dentin as home care measure is highly beneficial in controlling caries incidence. In addition a combination approach utilizing two agents, first APF, followed by SnF2 at follow-up visit provides outstanding results. They recommended as a follow up to apply 0.5% APF solution for 2 minutes followed by a 2 minute application of fresh 0.4% SnF2 at regular office visit. This recall should be done every 3 months along with periodontal evaluation and needful treatment.
As a home care measure the patients with poor dexterity can use power driven brushes to ensure thorough cleaning of teeth followed by 0.4% stable water free SnF2 gel. Also frequent motivation and education must be provided to the patient for thorough cleaning of the overdenture.
If despite the above mentioned suggestions oral hygiene cannot be maintained then the treatment may lead to failure.
• Insufficient inter-occlusal space: When an overdenture is made, especially with internal attachments, the available interocclusal distance of a standard denture usually cannot be compromised. The placement of an attachment, the artificial teeth and the necessary acrylic to retain the attachment and artificial teeth over the natural tooth should be within the parameter of available inter ridge distance.The encroachment of the interocclusal distance can jeopardize the whole purpose of the treatment with compromised esthetics and function.
A word of caution needs to be mentioned while fixing denture magnets with auto- polymerizing acrylic resin. The force needed to separate magnets was designated as breakaway load expressed in terms of grams. The value of breakaway load is inversely proportional to the distance of separation and inclination between the magnets.[11], [12]. Patient was instructed to apply minimal occlusal or bite force while fixing denture magnet as more pressure would displace magnets inwards which in turn decrease the breakaway force when the denture was later on inserted in patient's mouth. This was justified by the fact of REAL-EFF (resiliency and like effect). The force required for the Dyna Direct Magnet system used in the current case was 500gms according to the manufacturer.
To summarize, it would be fair to explain that this complete overdenture would be more retentive in patient's mouth as soon as it is inserted. These magnets are wholly biocompatible in the human body and by itself exert no deleterious effects in human tissue. Inert magnetic field is harmless to human body. This can also be safely used for patients with cardiac pacemaker but magnets must not be brought closer than 1 cm to the pacemaker during trial procedures [13], [14], [15], [16]. On the other hand, magnets may interfere with some mechanical devices. Concerns have been raised about using MRI (Magnetic Resonance Imaging) with patients wearing dentures with magnets (Prof. Dr. PF van der Stelt, University of Amsterdam 1987). It is evident that patients have to remove the denture before such examination. In most cases it is a sufficient contra measure, though when examining the area of head and neck it is a must to remove root-caps, direct keepers & / the medical abutments, especially when no distortion of the image is allowed. Leaving the magnets in the mouth should not pose a direct danger for the patient but the images achieved as a result of such examination will be greatly distorted and magnets will be destroyed.[18]
Conclusion:
The use of over dentures is not a new concept. It is one that has become increasingly more popular as the emphasis on prevention in dentistry has grown. Its usage is limitless and should be encouraged. To date, most failures have been the result of poor case selection and inadequate supervision to control maintenance. As more is learned about overdentures, success rates will improve.
Aknowledgements:
School Of Dental Sciences. Krishna Institute of Medical Sciences University, Karad. Maharashtra
References:
1. Akaltan F, Can G. Retentive characteristics of different dental magnetic systems. J Prosthet Dent. 1995 Oct; 74(4) : 422-7
2. Bormes T. Magnets myth and magic Trends Tech. Contemp Dent Lab 1998 Apr; 5(3): 42-7
3. Freedman H. Magnets to stabilize dentures. J Am Dent Assess. 1953:47: 288-97
4. Dyna dental engineering BV design: dyna – direct magnetic attachment system
5. Gendusa NJ. Magnetically retained overlay dentures. Quintessance Int. 1988; 19:265-71
6. Gillings BR. Magnetic retention for complete and partial overdentures. Part1. J Prosthet Dent 1981; 45: 484-91
7. Gillings BR, Samant A. Overdentures with magnetic attachments. Dent Clin North AM 1990 Oct; 34(4) : 683-709
8. Gillings BR. Magnet Overdentures, Aust Prosthodont J. 1993:7:13
9. Highton Caputo AA. Magnetically retained partial denture. Quintessence 1988; 19: 889-94
10. Davis DM, Packer ME, Mandibular Overdentures stabilized by Astra Tech implants with either ball attachments or magnets; 5 year results. Int J Prosthodont. 1999 May-Jun; 1993: 222-9
11. Gillings BR. Magnetic retention systems for overdentures. Aust Soc Prosthet Bull 1976; 6-9
12. Gillings BR. Magnetic retention for overdentures, part II. J Prosthet Dent 1983; 49: 607-18
13. Barnothy MF, Biological effects of magnetic fields, New York Plenum Press,1964,PP 29-306
14. Drago CJ. Tarnish and corrosion with the use of intra oral magnets. J Prosthet Dent. 1991 Oct; 66(4): 536-40
15. Evans RD, Mc Donald F. Effect of corrosion products (Neodymiun Iron Boron) on oral fibroblast proliferation. J Appl Biomater. 1995; 6(3):199-202
16. Hiller H, Weissberg N, Horowitz G, Ilan M. The safety of dental mini magnets in patients with permanent cardiac pacemakers. J Prosthet Dent. 1995 Oct; 74(4) : 420-21
17. Shannon IL, Cronin RJ Jr: Chemical protection of tooth surfaces in patients with overdentures, in Brewer AA, Morrow RM (eds): Overdentures. St Louis , CV Mosby, 1975, pg 237-247.
18. 1603-01.04 Dyna Magnet Manual GB pg 1-40
|