Introduction
Vascular anomalies are biologically and clinically distinct group of entities.[1],[2] These vascular anomalies require a multidisciplinary team for diagnosis and treatment plan involving conservative, interventional and surgical treatment.[3] Diagnostic imaging plays a pivotal role in providing structural and functional information required for treatment planning.[4],[5]
Studies have demonstrated that CTA (Three dimensional Computed Tomographic Angiography) with three-dimensional (3D) reconstructions elucidates the vasculature and their relationship surrounding soft tissue and bones and moreover was found to have excellent spatial and temporal resolution.[6],[7] In our case, CTA revealed a buccal artery in the left maxillary alveolar region and an abnormal tangle of blood vessels arising from external carotid artery.
Case Report
A twenty seven year old male patient reported to our department of Oral Medicine and Radiology, complaining of discoloration with swelling in the left side of the face and bleeding gums in maxillary left front and back teeth region since two years. Thorough history did not reveal any pain, but had mild discomfort during mastication. Though the discoloration was present since birth, patient noticed swelling of the affected region and also increase in size of the gums to present size since two years. There was history of spontaneous bleeding from the gums of considerable amount, which he noticed on waking up in the morning. There was no history of fever, headache, trauma, seizures, nausea. Past medical history revealed that patient was given intralesional steroids (Kenocort-forty milligrams) and Beta blockers (Propranolol-fifty milligrams) for three months by a plastic surgeon. After treatment though patient observed mild regress in the size of swelling and also bleeding within the oral cavity, it recurred after stoppage of treatment.
Clinical Examination
General physical examination did not reveal any other abnormality, except for that on extra oral examination, there is reddish purple discoloration of the left side of the face with gross facial asymmetry extending superioinferiorly from upper margin of the orbit to the level of the corner of mouth , mediolaterally from midline of the nose to the temple region ending anterior to the hair line (Fig 1,2). On palpation the skin over the swelling was relatively warm without visible pulsations and there was blanching on application of pressure.
 | Fig 1 - Front View
 |
 | Fig 2 - Lateral View Showing Reddish Purple Discolouration Of Left Side Of The Face
|
Intra oral examination revealed generalized enlargement of gingiva labially, bucally and palatally involving entire left upper quadrant involving marginal and attached gingiva , which had a reddish pink hue (Fig 3,4). There is also reddish purple discoloration of the mucosa involving soft and hard palate till the midline on the left side and also buccal mucosa opposite to Maxillary left central incisor, lateral incisor,canine, first and second premolars and first, second and third molars (Fig 5,6). Generalised calculus deposits were noticed .The gingival swelling was soft in consistency with blanching and bleeding was observed from gingiva on palpation. Deep pockets were noticed with bleeding on slight provocation and there was generalized gingival recession and Grade III mobility of Maxillary first and second premolars, first ,second and third molars and Grade II mobility of Maxillary left central incisor, lateral incisor and canine were noted.
 | Fig 3 - Swollen, Erythematous Marginal And Attached Gingiva Extending To Muco Gingival Junction Superiorly & Extending To Middle Thirds Of Crowns Of Left Upper Quadrant Inferiorly.Generalised Moderate Stains And Calculus Deposits
|
 | Fig 4 - Swollen, Erythematous Marginal And Attached Gingiva Extending To Muco Gingival Junction Superiorly & Extending To Middle Thirds Of Crowns Of Left Upper Quadrant Inferiorly.Generalised Moderate Stains And Calculus Deposits
|
 | Fig 5 - Labial Mucosa & Buccal Mucosa Showing Reddish Discoloration In Left Upper Quadrant And Hard Palate & Soft Palate Showing Reddish Discoloration On Left Side
|
 | Fig 6 - Labial Mucosa & Buccal Mucosa Showing Reddish Discoloration In Left Upper Quadrant And Hard Palate & Soft Palate Showing Reddish Discoloration On Left Side
|
On further enquiring patient did not give any pain or loss of visual acuity in left eye. Based on the inspectory and palpatory findings, it was provisionally diagnosed as Sturge Weber syndrome type II. Vascular anomalies with similar features were considered asdifferential diagnosissuch as Klippel- trenaunay syndrome, PHACES syndrome.
Investigations
Conventional radiographs such as IOPA and OPGrevealed generalized interdental horizontal bone loss and PA view did not reveal any intracranial calcifications (Fig 7,8,9,10,11).
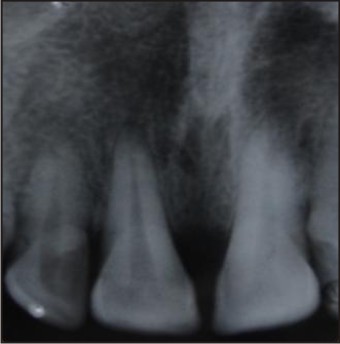 | Fig 7 - Iopa & Opg Revealed Generalized Horizontal Interdental Bone Loss
|
 | Fig 8 - Iopa & Opg Revealed Generalized Horizontal Interdental Bone Loss
|
 | Fig 9 - Iopa & Opg Revealed Generalized Horizontal Interdental Bone Loss
|
 | Fig 10 - Iopa & Opg Revealed Generalized Horizontal Interdental Bone Loss
|
 | Fig 11 - Pa View Did Not Reveal Any Intracranial Calcifications
|
Patient was subjected to specialised radiographic procedure i.e CT angiography of head and neck vessels. With serial, axial angiogram sections from neck to skull base using intravenous contrast were obtained. CT scan of the brain did not reveal any abnormalities (Fig 12). Coronal section MIP(maximum intensity projection) and volume rendered images showed abnormal tangle of blood vessels medial to pterygopalatine fossa supplied by tortuous, hypertrophied external carotid artery and the lumen of the vessels is clear without any thrombus and are of normal volume. Mild soft tissue enhancement was noticed on left side cheek region (Fig 13,15,16,17). 3D volume rendered images illustrated hypertrophied buccal artery, branch of external carotid artery on the maxillary alveolar bone on left side (Fig 14). Complete blood picture revealed Hemoglobin (Hb %), RBC, WBC, Differential count and Clotting time, Bleeding time within normal limits. Ophthalmic evaluation reported normal findings. Based on the clinical and radiological examination findings a patient is diagnosed with having Sturge Weber Syndrome type two.
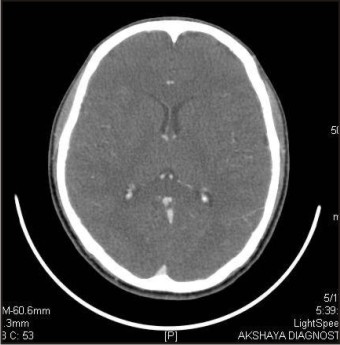 | Fig 12 - Ct Axial Section Of Brain Study Revealed Normal Findings
|
 | Fig 13 - Ct Coronal Section Shows Abnormal Tangle Of Blood Vessels Medial To Pterygo Palatine Fossa Supplied By Tortuous, Hypertrophied External Carotid Artery And Mild Soft Tissue Enhancement On Left Cheek Region
|
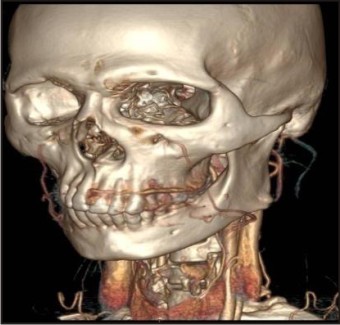 | Fig 14 - Hypertrophied Buccal Artery, Branch Of External Carotid Artery Is Seen On Buccal Surface Of Maxillary Alveolar Bone. (Feeder Vessel : Maxillary Artery )
|
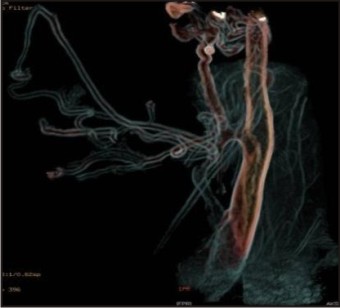
 | Fig 15 - Ct Angiography Volume Rendered Images Revealed Abnormal Tangle Of Blood Vessels Medial To Pterygo Palatine Fossa Supplied By Tortuous, Hypertrophied External Carotid Artery
|
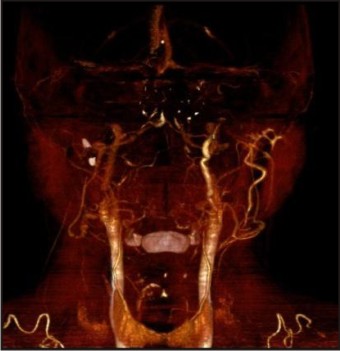 | Fig 16 - Ct Angiography Volume Rendered Images Revealed Abnormal Tangle Of Blood Vessels Medial To Pterygo Palatine Fossa Supplied By Tortuous, Hypertrophied External Carotid Artery
|
 | Fig 17 - Vessels Are Clear Without Any Occlusions And Thrombus Formation
|
Since the patient is concerned about bleeding from the gums and esthetics, a tailored treatment plan is considered in this case. As port wine stain is a low flow vascular malformation, treatment typically offered only for symptomatic lesions. Patient is reassured of benign nature of the lesion The first phase of treatment includes control of local etiological factors by scaling and root planning and by local hygiene measures with control of local hemorrhage under antibiotic coverage, followed by sclerotherapy and cryosurgery for the vascular lesion is planned.
Discussion
Vascular anomalies were earlier classified based on clinical behaviour and endothelial cell characteristics into two major characteristics, that is hemangiomas and vascular malformations. Recently this classification has been modified and adopted by Mulliken and Young who founded the international society for the study of vascular anomalies based on the depth of the lesion and flow characteristics which elucidates the nature of the vascular anomaly. The associated syndromes pose a challenge to us due to vulnerability of excessive bleeding, sometimes whichcan be life threatening.[2],[3] Though the present case is Sturge Weber Syndrome type two without any intra cranial lesions, the severe gingival enlargement on the affected side associated with severe periodontal disease is a major concern to be addressed cautiously. Accurate classification of vascular malformations can be difficult, but important because treatments and prognosis vary based on the type of lesion.
Diagnosis is based on combination of clinical features with a imaging strategies in the assessment of vascular lesions such as Doppler Ultrasound ,Computed Tomography(CT)/CTA, Magnetic Resonance Imaging (MRI) / Magnetic Resonance Angiography(MR Angiography), Digital subtraction angiography (DSA).[7] Doppler scanning visualizes soft tissue lesions and determines flow characteristics, but it is not useful in detection of lesions involving bone. MRI characterizes soft tissue tumor architecture, but is limited when it involves bone. MR Angiography is semi invasive and accurate and reveals the soft tissue abnormality and its relationship to the adjacent soft tissues but is poor in detection of calcifications and bone abnormalities. Longer imaging time leading to motion and pulsation artifacts, inability to depict true lumen of vessels in areas of turbulence were major disadvantages that was considerably dealt with by the introduction of contrast enhanced dynamic 3D MR Angiography.[8] Though bone and soft tissue densities are well appreciated in conventional CT scan but vascular lesions are poorly visualized, due to a slow image acquisition rate. CT angiography is minimally invasive/semi-invasive technique. CTA is superior to US and MRI in spatial and temporal resolutions and 3D formatting, better defining the gross total anatomy and the relationship to important structures in the head and neck both soft tissue and bones.DSA is invasive, traumatic, relatively high cost and carries a small risk of neurologic morbidity and stroke.[1],[14],[15]
In our case the patient had port wine stain on left side of the face with gross gingival enlargement in left side of maxilla. CT Angiography with 3D reconstruction with volume rendering had unleashed underlying feeder vessel buccal artery and also an associated abnormal tangled blood vessels medial to pterygopalatine fossa at the junction of superficial temporal artery and maxillary artery and External carotid artery was hypertrophied, tortuous which is a very unique feature of its own to be found in this patient. So volume rendering had played a remarkable role in identification of vessels , characterization of the gross anatomy and also their relation to adjacent structures.
Sturge Weber Syndrome is sporadic neurocutaneous disease characterized by focal port-wine stain, glaucoma, and choroidal hemangioma and lepto meningeal angiomas most often involving occipital and parietal lobes. Our patient had Sturge Weber Syndrome type two condition , as he did not have lepto meningeal angiomas or glaucoma.[9],[11]
Computed tomographic angiography is used to visualize blood vessels that have been opacified by contrast material. This include Circle of Willis ,Carotid arteries , Subclavian arteries , Thoracic & abdominal aorta , Renal vasculature, Abdominal viscera vasculature, Lower limb arteries ,Venous structures (major veins and dural venous sinuses) .Contraindications include Pregnancy, Unstable vital signs, Allergic patient, Kidney problems, Severe diabetes. CTA obtains images in seconds, careful timing of intravenous contrast administration with directed imaging results in capture of contrast within the vascular lesions, as well as feeder vessels and draining veins.Volume-rendered reformatting is helpful in categorizing clinically significant vascular head and neck lesions, resulting in excellent resolution and high diagnostic value.[10]
In particular, 3D CTA might allow accurate differentiation of hemangiomas from Arteriovenous malformations and of lymphangiomas from other types of lesions. MIP (Maximum intensity projection) and surface rendering helps to create 3D angiogram images from the CT data. But these methods have short comings as they show only small fraction of available data. Hence, a new technique was developed that is volume rendering which displays a volume of data entirely. It allows to provide vessel depth information and to display multiple overlapping vessels. CTA for arterial studies , scanning will begin twenty to twenty five seconds after the start of contrast material injection and the scan duration was twenty two to thirty seconds. Once the scanning is done the 2D scan images they are edited with volume rendering software to produce 3D images. Voxels of a particular vessel varies based upon the distribution of intensities. This computer generated algorithm is reviewed by a skilled operator and adjusted as required to obtain anatomical details.[12],[13]
CTA for arterial study in this case was performed with a eight row detector CT scan, scanning was begun nine seconds after the start of contrast material injection with contrast flow rate of four milliliters/second and the scan duration was 8.7 seconds. Once the scanning is done, the 2D scan images they are edited with volume rendering software to produce 3D images. Voxels of a particular vessel varies based upon the distribution of intensities. This computer generated algorithm is reviewed by a skilled operator and adjusted as required to obtain anatomical details.
Color and opacity are assigned based on voxel composition gradient and volume rendered images can be viewed via a video loop. The 3D cues of the video loop help in casting transparent renderings. This volume rendering is particularly useful for visualizing larger vessels, multiple overlapping vessels and location of vessels related to tumor and other tissues.[12]
Conclusion
In this case, 3D CT Angiography helped us in identifying vascular lesions and feeder vessels on affected side of the patient. So Buccal artery a branch of maxillary artery was found to be feeder vessel,which can be manipulated with various conservative and surgical procedures to avoid any surgical hemorrhagic catastrophe and a unique presence of abnormal tangle of blood vessels medial to pterygopalatine fossa had given a cue to tailored treatment plan. Hence, the role of radiologist is reemphasized in dealing with such situations by virtue of available modern imaging modalities.
References
1. Mazroa JA, Elrakhawy MM. What can 3D CT angiography add in evaluation of facial vascular lesions?;The Egyptian Journal of Radiology and Nuclear Medicine .2012; 43: 67–75.
2. Lowe LH, Marchant TC, Rivard DC, Scherbel AJ. Vascular malformations: classification and terminology the radiologist needs to know. Semin Roentgenol. 2012;47:106–117.
3. Roche E, Muchart Lopez J. New approach of the classification of vascular anomalies. Phlébologie 2010; 63(3) :31-38.
4. Ernemann U, Kramer U, Miller S, Bisdas S, Rebmann H, Breuninger H .Current concepts in the classification ,diagnosis and treatment of vascular anomalies et al. European journal of radiology. 2010;75:2-11
5. Thomas J Vogl, Marc Harth, Petra Siebenhandl. Different imaging techniques in the head and neck: Assets and drawbacks.World J Radiol 2010;2(6):224–9.
6. McCafferty IJ, Jones RG. Imaging and management of vascular malformations. clinical Radiology . 2011; 66 : 1208-1218.
7. Kumamaru KK,Hoppel BE, Mather RT, Rybicki FJ.CT angiography current technology and clinical use. Radiol Clin North Am. 2010;48(2):213-235.
8. Gold L,Nazarian LN, Johar AS, Rao VM. Characterization of maxillofacial soft tissue vascular anomalies by ultrasound and color Doppler imaging: an adjuvant to computed tomography and magnetic resonance imaging. J Oral Maxillofac Surg. 2003;61(1):19–31.
9. MariaBL, Olson LL, Comi AM.Sturge-weber syndrome, current management in child neurology.Current management in child neurology .BC Deckner Inc: 3rd ed;2005. pg 470–475
10. Kuszyk BS, Heath DG, Noy DR, Bluemke DA , Urban BA, Chambers TP . CT Angiography with Volume Rendering: Imaging Findings.AJR1995;165:445-448.
11. Butchibabu K, Pradeep K, AshankMishra, Krishnanjaneya Reddy, Muralikrishna T, Vijaya Lakshmi, and Radhika C .Periodontal Management of Sturge-Weber Syndrome. Case Reports in Dentistry Volume 2013 http://dx.doi.org/10.1155/2013/517145.
12. Salgado R, Mulkens T, Bellinck P, Termote JL.Volume rendering in clinical practice. a pictorial review.JBR–BTR 2003; 86: 215-220.
13. Perkinsa Jonathan A, Sidhub Manrita, Manninga Scott C,Ghionib Victor, Szeb Raymond. Three-dimensional CT angiography imaging of vascular tumors of the head and neck. Int J Pediatr Otorhinolaryngol 2005;69:319–25.
14. Brouwer PA, Bosman T, Van Walderveen MAA, Krings T,Leroux AA, Willems PWA. Dynamic 320-section CT angiography in cranial arteriovenous shunting lesions. AJNR 2010;31:767–70.
15. Reinacher P, Reinges MH, Simon VA, Hans FJ, Krings T. Dynamic 3-D contrast-enhanced angiography of cerebral tumours and vascular malformations. Eur Radiol 2007;17( 6):52–62.
|