Introduction :
Root resorption causes root shortening and breaks the integrity of teeth and this is very important for successful orthodontic treatment. External apical root resorption is an iatrogenic consequence of orthodontic treatment, although it may also occur in the absence of orthodontic treatment. Orthodontics is probably the only dental specialty that actually uses the inflammatory process as a means of solving functional and aesthetic problems. The Orthodontist should realize the risk factors of root resorption and do everything to reduce the occurrence of root resorption. Histological and radiographic observations show that root resorption incident to orthodontic treatment occurs apically.[1],[2],[3]
In orthodontics many attempts have been made to model the reactions of teeth and their supporting tissues on application of orthodontic forces[4]. One of these methods is Finite element method.
In the last decade the application of finite element method has revolutionized dental biomechanical research .The technique has been described in detail in an early standard textbook by Zeinkiewicz(1977)[5]
The finite element method is a highly precise technique used to analyze structural stress. The finite element method provides the orthodontist with the quantitative data that can extend the understanding of the physiologic reactions that occur[6]
The finite element method is a numerical method of analysis that allows the study of stress distribution in biological system.[7]
This method offers accurate modeling of tooth and its surrounding structures with its complicated geometry. It makes it possible to analytically apply various forces at any point, in any direction and also quantitatively and qualitatively assess the distribution of such forces through the alveolar bone, periodontal ligament and tooth[6]
Such detailed information on the stresses and strains in tissue is difficult to obtain and accurately analyze by any other experimental technique because of the interaction of surrounding tissues which may distort the data obtained for any individual material response.[7] Hence, Finite element method was chosen in this study to study the effects of root morphology on stress distribution at the root apex under various orthodontic loadings
Review of Literature :
Levander E, Malmgren O[8] (1988) evaluated risk of root resorption during orthodontic treatment with fixed appliance in relation to resorption after initial treatment and found moderate risk of severe root resorption was found in blunt roots, typical resorption of teeth with apical bends involved the bent part of the root.
Oyama K et al1[9] (2007) studied effects of root morphology on stress distribution at the root apex using 3-D finite element models divided by deviated root shape (normal, short, blunt, bend, pipette shaped) when orthodontic forces are applied in a vertical (intrusive) and horizontal (lingual) direction to the tooth axis and found risk of root resorption.
Geramy A[10] (2007) carried out a 3-D finite element analysis with the goal to compare various types of apical third of the teeth while loaded with intrusive force on four 3-D finite element models - normal root morphology, needle form, short and sharp root. The model with needle form apex showed similar finding for cervical area but increased to about 2.8 times in the apical area of the normal model. The study made it clear that deviations in the apical area can cause different stress concentration and promote the chance of root resorption.
Field C[11] (2009) studied the initial mechanical response to orthodontic loading and to investigate the stress-strain responses of teeth to orthodontic loading. The results stated that disto-cervical region of root experiences the greatest stress corresponding to the orthodontic force application area. It also showed that maximum strains occurred at the alveolar crest and root apex in the PDL and are the sites of greatest deformation.
Aims :
To investigate and compare effect of deviated root morphology on stress distribution at the root apex when intrusive and extrusive forces are applied.
Objectives:
1. The objective of this study will be to investigate stress distribution at the root apex in cases of deviated root shapes using finite element models (FEMs).
2. To determine the different types of orthodontic forces i.e. intrusion, extrusion, that cause stress, especially at the root apex.
3. To determine qualitatively the change in stress distribution pattern when different types of tooth movement are simulated by changing the direction of force application.
4. To assess quantitatively the amount of stress produced at the root apex by intrusive and extrusive forces.
Materials & Methods:
Preparation for FEM
A 3-dimensional finite element model of permanent maxillary central incisor with normal root morphology and its variation-dilacerated as classified by Lavender and Malmgren[6],[8] (four variations i.e. short root, blunt root, dilacerated root and pipette shaped root) were prepared along with its supporting structures (PDL, cancellous bone) using Ansys version 10 software. This model was then used to analyze the stress distribution on the root surface on application of various types of orthodontic forces (intrusive, extrusive).
Construction Of Maxillary Central Incisor Model With Deviated Root Morphology:
All the steps involved were similar to that of construction of normal model(crown length of 10.5 mm and root length of 13mm based on data derived from Ash -1984) except the morphology of root structure.
For model B (dilacerated root) the root was made to follow a curve in distal direction keeping the length constant. (Figure No.1)
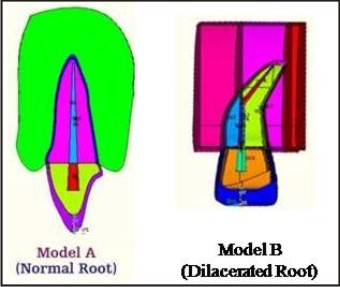 | Fig 1 : Construction Of Maxillary Central Incisor
 |
Material property data representation :
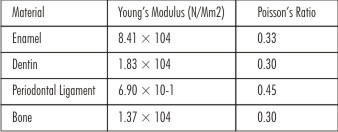
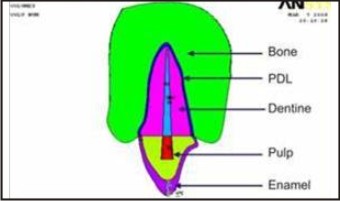
Each structure was then assigned a specific material property. The different structures in the finite element model are enamel, dentine, periodontal ligament and alveolar bone. The material properties used in this study have been taken from finite element studies previously conducted and were the average values reported in the literature.[9] (Figure No.2,Table No.1).
 | Fig 2 : Defining The Columes
|
 | Table 1: Material Parameters Used In The Finite Element Model.17
|
In this model all the structures were assumed to be isotropic. (For an isotropic material the properties are same in all directions). (Table No.1).
Boundary Condition & Solution:
The boundary condition, in the finite element model was defined at all the peripheral nodes of the bone with 0o of freedom in all directions and that of tooth structure and surrounding PDL with 6o of freedom.
The loading configuration was designed to simulate conventional orthodontic tooth movement. Application of forces in this study was in conjunction with the range of optimum forces for orthodontic tooth movement as proposed by Proffit.[12] (Table 2, Figure No. 3).
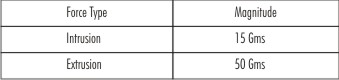 | Table 2: Force Used For Different Type Of Tooth Movement
|
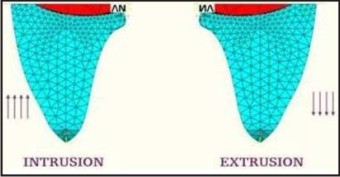 | Fig 3 : Force Direction
|
Result: (Table No 3)
-Deviated root morphology of tooth structure is suggested to prone for increased root resorption as compared to normal root morphology on application of orthodontic forces in various directions.
 | Table 3: Stress Values At The Apex
|
-Dilacerated root morphology was seen to be most affected root morphology for root resorption.
Apex shows maximum stress in dilacerated root on application of orthodontic forces in various directions.(Table No 3).
In conclusion, dilacerated root morphology exhibit far greater tendencies for root resorption as compared to normal root shapes. This conclusion makes it highly meaningful to identify the root shapes in the diagnosis and treatment planning stage itself. Orthodontic force application on such teeth should be evaluated with care and also forces of lesser magnitude and intermittent in nature are more advantageous in root with deviated morphology.
The future scope in the direction of FEM studies should involve more accurate simulation of loading and approximation of material behaviors as well as variations in geometries of PDL, bone and tooth in 3-dimensional finite element analysis
Discussion:
With increasing focus on the objective assessment of orthodontic treatment outcomes, apical root resorption is clearly an important effect to which the orthodontic specialty must consider. However, despite the rigorous efforts, the exact nature of the initiation and control of apical root resorption remains essentially unknown.[13]
It is most frequently found in the apical area of root, because orthodontic forces are concentrated there and the apical tooth structure presents cellular cementum that is less mineralized, more friable and easy to be traumatized.[14]
Studies state that maxillary incisors are most susceptible for root resorption during orthodontic treatment followed by maxillary canine and mandibular anterior teeth. Maxillary and mandibular posteriors are supposed to be least affected.[15] , [16]
All the orthodontic forces applied were with in the optimum levels as stated by Profitt.[12]
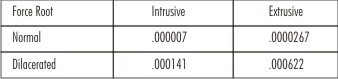
1. Intrusion (15 gms): (Figure no. 4)
In the present study intrusive force was produced with the application of optimum orthodontic force of 15 gms in vertically upward direction.[12]
All the models showed stress concentration at the cervical area of root surface. (Figure No. 4)
At the apex (Table No 3) maximum stress was seen at the dilacerated root .
These result are comparable with study carried out by Koji Oyama et al[9] (2007).The study concluded that teeth with deviated roots morphology resulted in a greater loading of the root than normal root shape during orthodontic force application and it is therefore important to identify the root shapes at the beginning of orthodontic treatment. The findings of present study were not in accordance with the study carried out by Rudolph D[17] (2001).
 | Fig 4 : Intrusion
|
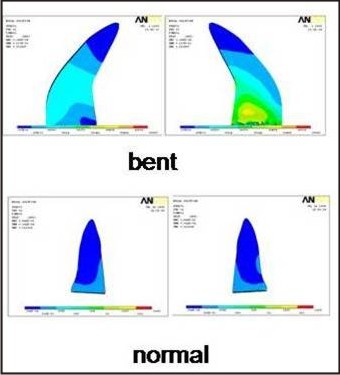
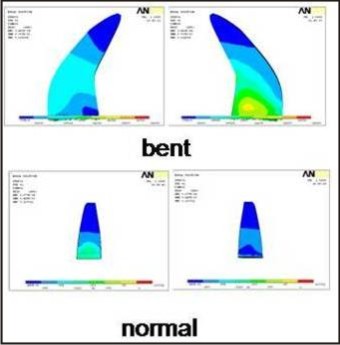
2. Extrusion (50 gms): (Figure No. 5)
Extrusion was achieved by applying 50 gm of vertical force directed towards the incisal edge and parallel to the long axis of the tooth.
Overall maximum concentration of stress was seen at the cervical region of the model.
At the apex, maximum stress was seen at the apex of dilacerated root as compared to the normal model. The stress value was 0.000622 N/mm2 i.e. approximately 23 times that of normal model (0.0000267N/mm2). (Table No. 3)
The findings of present study were not in accordance with the study carried out by Rudolph D[17] (2001).The difference in the results in the above study and present study maybe due to difference in construction of Finite element model in relation to the root shapes or may be due to difference in the properties applied to each tooth structure.
 | Fig 5 : Extrusion
|
By combining and comparing the result of the present study on application of different forces on deviated root forms, stress distribution pattern is clarified suggesting of increased root resorption in maxillary central incisor with deviated root morphology.
It can also be stated that maximum root resorption is likely to be seen in dilacerated root These results are in accordance with the studies carried out by Levander E, Malmgren[5] (1988), Mirabella A, Artun J[18] (1995) , Sameshima G, Sinclair P[19] (2001), Nigul K, Jagomagi T[20] (2006)
Conclusion:
-Deviated root resulted in a greater loading of the root surface than normal root shape during orthodontic force application even at optimum level. These deviations are suggested to promote root resorption more than that seen in normal.
-It is therefore necessary to identify the root shape at the beginning of orthodontic treatment as factors for high risk of root resorption.
-Orthodontic force application on such teeth should be evaluated with outmost care and forces lesser then the optimum force required or intermittent forces are suggested.
-Use of instruments like Correx or Dontrix gauges are advocated for measuring the forces applied by various orthodontic appliances during the treatment.
-Intra oral peri apical radiographs of teeth with high risk of root resorption during the course of treatment can aid in keeping a check on root resorption.
References :
1. Reitan, K. Initial tissue behavior during apical root resorption. Angle Orthod. 1974; 44:68-82.
2. Rygh, P. Orthodontic root resorption studied by electron microscopy. Angle Orthod. 1977; 47:1-16.
3. Harry, M.R. and Sims, M.R. Root resorption in bicuspid intrusion. Angle Orthod. 1982; 52:235-258.
4. McGuinness NJ, Wilson AN, Jones ML, Middleton J.A stress analysis under periodontal ligament under various orthodontic loadings.Eur J Orthod.1991 Jun;13(3):231-42.
5. Jones ML, Hickman J, Middleton J, Knox J, Volp C.A validated finite element method study of orthodontic tooth movement in human subject.J Orthod.2001 Mar;28(1):29-38.
6. Middleton J, Jones M, Wilson A. The role of the periodontal ligament in bone modeling: the initial development of a time-dependent finite element model.Am J Orthod Dentofacial Orthop.1996 Feb; 109(2):155-62.
7. Puente MI, Galbán L, Cobo JM. Initial stress differences between tipping and torque movements.A three-dimensional finite element analysis.Eur J Orthod.1996 Aug;18(4):329-39.
8. Levander, E. and Malmgren, O. Evaluation of the risk of root resorption during orthodontic treatment. A study of upper incisors. Eur. J. Orthod. 1988; 10:30-38.
9. Horiuchi A,Hotokezaka H, Kobayashi K. Correlation between cortical plate proximity and apical root resorption.Am J Orthod Dentofacial Orthop.1998 ; 114(9):311-318
10. Proffit W, Fields H. Contemporary orthodontics. Fourth edition. St.louis: Mosby publishers; 2007
11. Vlaskalic V et al.Etiology and sequelae of root resorption. Seminars in orthodontics.1998; 4(2): 124-131.
12. Preotease C et al. Orthodontically induced root resorption correlated with morphological characteristics. Romanian J of Morphology and Embryology. 2009; 50(2):257-262.
13. Sameshima G, Asgarifar K. Assessment of root resorption and root shape: periapical vs panoramic films. Angel orthod.2001; 71(3):185-189
14. Ramanathan C, Hofman Z. Root resorption in relation to orthodontic tooth movement. Acta Medica. 2006; 49(2): 91-95.
15. Oyama K, Motoyoshi M, Hirabayashi M. Effect of root morphology on stress distribution at the root apex. Eur J Orthod.2007; 29(2): 113-117.
16. Rudolph DJ, Willes PMG , Sameshima GT.A finite element model of apical force distribution from orthodontic tooth movement.Angle Orthod.2001 Apr;71(2):127-31.
17. Hines, F.B., Jr. A radiographic evaluation of the response of previously avulsed teeth and partially avulsed teeth to orthodontic movement. Am. J. Orthod. 1979; 75:1-19.
18. Malmgren, O., Goldson, L., Hill, C., Orwin, A., Petrini, L. and Lundberg, M. Root resorption after orthodontic treatment of traumatized teeth. Am. J. Orthod. 1982; 82:487491.
19. Malmgren O, Levander E. Minimizing orthodontically induced root resorption: Guidelines based on a review of clinical studies. World j orthod. 2003; 4 (1):19-30.
20. Rudolph DJ, Willes PMG , Sameshima GT.A finite element model of apical force distribution from orthodontic tooth movement.Angle Orthod.2001 Apr;71(2):127-31.
|