Introduction
Endodontic treatment in deciduous teeth is a therapeutic option with infected pulps[1]. Treatment of root canals of deciduous teeth with necrosis or irreversible pulpitis helps to keep the integrity of the primary teeth until their physiological exfoliation[2],[3],[4].
The root canal treatment involves removing microorganisms from within the pulp space and filling of root canal system, which is done to prevent re-infection whilst preventing injury to the succedenous tooth bud. The most challenging step in the root canal treatment is the determination of the working length, which is defined as distance from the coronal reference point to the point at which the canal preparation and obturation should terminate.[5]
In primary teeth, the ideal method used to determine the root canal length is controversial. Traditionally, radiographs have been the principal tool for determining primary root canal lengths. However, radiographs can only provide two-dimensional image. The accurate dimension of root canal length or even an estimation of the dentinocemental junction cannot be achieved radiographically because of anatomic variations, interference of anatomical structures or errors in projection.[6] It has been suggested that the radiographically obtained working length be shortened by 2-3 mm, especially in resorbing teeth, to prevent over extension through the apical foramen.[7] But this cannot be applied as a universal criterion as there is vast variability in the amount of resorptive process of each individual primary tooth. Also, superimposition of permanent successors over primary root apices may obscure root canal length determination.[3],[8] Furthermore it has been seen that most anatomic variations in the root canal of primary teeth during resorption are present in the facio-lingual plane, which are missed easily upon radiographic assessment.[9] In children, it is often very difficult to get intraoral radiographs to measure the root canal length because of poor cooperation and limited access to the mouth.[3], [8]
Recently, electronic methods for determining the root canal length in both primary and permanent teeth have gained popularity amongst dentists because of the hazards of radiation, the technical problems associated with radiographic techniques, and the avoiding over instrumentation beyond the root canal terminus. However, there are few studies about the use of electronic apex locators in primary dentition in an in vivo setting.
Therefore, the purpose of this study was to evaluate the working length by means of fifth generation apex locator (Propex II) and to co-relate this working length with the traditional radiographic working length determination in primary teeth of children visiting the general dental OPD of our hospital.
Materials and Method
This was an in vivo study on 199 root canals from 91 teeth in children reporting to the department of pediatric dentistry.
Inclusion criteria for the study –
Primary teeth indicated for pulpectomy
Indications for pulpectomy in primary teeth according to Ingle –
Primary teeth with pulpal inflammation extending beyond the coronal pulp, but with roots and alveolar bone free of pathologic resorption.
Primary teeth with necrotic pulps, but minimum bony destruction in the furcation area.
Pulpless primary teeth with sinus tracts.
Pulpless primary teeth without permanent successors.
Teeth with one/ all of the above indications were included in the study.
Under appropriate local anesthesia, all caries was first removed and access preparation completed. Orifices of the root canals were identified. After initial debridement and cleaning, one head of electrode of Propex II EAL (lip clip) was attached to the mouth and the other one (file holder) was attached to a K file # 15. File was gently introduced to the canal until the EAL monitor showed that the file has reached the apex. At this point a rubber stop was set on the coronal reference point and file was removed. On a molar tooth, the process was done on all 3 canals. Then the distance between rubber stop and file apex was measured by a millimeter ruler and measures were recorded as measured working length by EAL in mm.
For determination of canal length by radiographic method, an approximate working length was established using the preoperative radiograph as a guide. A K file # 15 with a rubber stopper was introduced. After establishing a reference point on the tooth, the file was advanced till the approximated working length. The tooth was radiographed using the standard angulations in bisecting angle technique. The length of the file reaching the radiographic apex was measured and noted. The radiographic working length was established 2 mm short of this length[7]
The results obtained were subjected to statistical analysis.
Results
199 root canals of 91 primary teeth teeth were selected and subjected to electronic and radiographic working length determination. The mean working length in the radiographic group was 11.325 with sd deviation of ± 1.726. and 10.327 and 10.327 ± 1.977 in the apex locater group.
The mean difference between radiographic and apex locater working length with a0.05 level of significance was 1.025 with sd of± 1.006 was statistically significant
Statistical analysis was done and the student t-test was applied. The mean difference between the radiographic working length and the apex locator was 1.025 +/- 1.006, with p value <0.001. (Table 1 & 2).
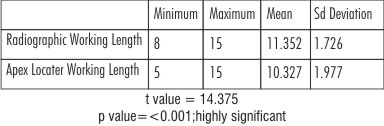 | Table 1 : Descriptive Statistics Mean And Standard Deviation For Radiographic And Electronic Working Length Determination (N=199)
 |
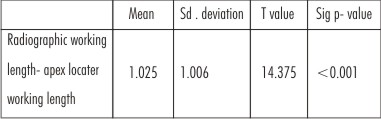 | Table 2 : Paired Test Mean Difference Between Radiographic And Electronic Working Length
|
There was a highly significant difference between the two measurements with the electronic lengths being shorter than the radiographic length.
Discussion
An important facet of successful pediatric endodontics is attaining the compliance of the child patient. The procedure and its duration form an important part to ascertain patient cooperation.[12] Determining the working length is a necessary step to perform the procedure. The use of radiography in pulp treatments has some inconveniences, such as: interferences, superimposition or variation of images; patient exposure to x ray; and technical aspects like quality of the equipment available in the clinic, the time to obtain radiographs and the child’s level of cooperation.[13] Inappropriate radiographic techniques due to oral cavity size of children, the film size and the positioner size can make accurate location of radiographic apex difficult.[14],[15] A very significant fact that does not support the use of radiographs for working length determination is that most anatomic variations in the root canal of primary teeth during resorption are present in the facio-lingual plane, which are missed easily upon radiographic assessment.[9]
Other methods have been proposed to determine the working length of root canals, such as apex locators. Over the period of time, various improvements in apex locaters have made them more accurate and sensitive in determining working length. Newer generations use multiple frequencies to determine the point of maximum impedance, which defines the endpoint of the working length.[16],[17],[18],[19] Some authors have reported the accuracy of the apex locators in permanent teeth[14], but information on primary teeth is limited in both in vitro and clinical studies.[12],[13] Apex locaters are considered to be inaccurate in teeth undergoing resorption.[12] But Leonardo et al in his study comparing actual working length ex vivo and working length obtained by root zx II and sybron endo found that their readings were highly corelatable with actual length in incisors as well as molars, with or without resorption.[13]
Though extensive studies on the anatomy of apical constriction have not been done in primary teeth as done by Kutler et al in permanent teeth.[20] But a few studies done on the changing anatomy of the apex of primary teeth yield the following results:[21]
1. Endodontic and anatomic apex distance is much shorter than 2-3 mm in primary teeth as opposed too permanent teeth.
2. Lingual canals are shorter due to pattern of resorption, which is more so in case of lower teeth.
3. Root length in excess of 7mm is associated with regular, intact, round or multiple apices with small diameter (0.1 mm) and curved canal shapes. Establishing the fact that a constriction at the apex is present despite the ongoing resorption, which can be detailed by an electronic apex locator.
Studies have been published comparing the apex locators with Conventional radiography. Katz et al reported the canal length of primary teeth with the Root ZX and with CR in vitro. They did not find statistically significant differences comparing both methods with the actual length.[22], [3] Aghreed GH Mohammad in his study comparing tactile method, conventional radiography and electronic apex locaters proved that apex locater should be the technique of choice in determining root canal length in primary teeth[23]
Subramaniam et al reported an in vitro study comparing the digital tactile sense technique, apex locators, and conventional and digital radiography with the stereomicroscopy (real length) to determine the working length in primary single rooted teeth. They did not find statistically significant differences after comparing all the techniques.[17] However, in a clinical study done by Nuria Patino Martin et al on primary teeth working length determination, there was a significant difference between the working length determined by radiographs and apex locators and the comparison between real length as ascertained by SEM and the two techniques showed that apex locators were significantly more accurate than conventional radiography. [11]
In support of the use of apex locators, some authors have also concluded that an apex locator is a valuable tool to complement the radiographic methods of working length determination, since it reduces the number of radiographs required for determination of root canal length.[24]
Most research that has determined working length in primary teeth has been done in vitro.[3],[19] For this reason, we consider it important to perform further clinical studies. In Our study we used Propex II, a 5th generation apex locater which works on the principal of measure of energy at multisignal frequencies rather than the amplitude of the signals. It is claimed that the 5th generation apex locators give superior readings[19],[25],[26] in the presence of a wet canal rather than a dry canal[27] ,which makes it more helpful for usage, especially in children, where isolation is tough to be maintained, thus supporting the choice of use of propex 2 in our study.
Our study showed a statistically significant difference between radiographic and electronic apex locator’s determination of working length in primary teeth.
The results also showed that the electronic apex locator lengths were shorter in most cases evaluated. The reason could be that in the primary anterior teeth (incisors and canines), the permanent tooth buds lie apically and lingually near the primary roots. Resorption is initiated on the primary root’s lingual surface. This causes the apical foramen to move coronally, resulting in a difference in the apical foramen and the anatomic apex and complicating determination of root canal length. At the time of root resorption, additional dentin deposition also occurs internally, which might significantly change the number, size, and shape of the canals within the primary roots. Continued physiologic, apical resorption of the roots makes the teeth progressively shorter. In addition, resorption on the roots’ internal surfaces adjacent to the forming permanent tooth might open other communications with the periapical tissues, which in essence may be responsible for the consistently shorter readings obtained in our study.[28]
There is also a marked variability in terms of tactile assessment as well as radiographic interpretation as compared to actual working length, while it has been shown by different investigators in various in-vitro studies that the apex locaters give accurate readings in terms of ascertaining the endodontic working lengths[3],[16],[29],[30]. Our study is in accordance with the study of Kielbasa et al.[31] who reported that Root ZX was an accurate method and that tooth type, canal, and apex with or without resorption did not alter the apex locator’s accuracy. A similar study by Oznuran F et al[32] and a recent meta analysis on the accuracy of apex locater in primary teeth[33] conclude that electronic apex locater offer acceptable level of accuracy in determining the root canal length in primary teeth
Also the fact that this is a simpler, non-painful and easier methodology gives an additional benefit of use especially in the pediatric patient; so we recommend the use of apex locater as an alternative to radiography in children.
References
1. Fuks AE, Eedeliman E. Pulp therapy in the primary dentition. Current opinion in Dent.1991; 1(5): 556-63
2. Dandashi MB, Nazif MM, Zullo T, Elliot MA, Schneider LG, Czonstkowsky M. An in vitro comparison of three endodontic techniques for primary incisors. Pediatric Dent.1993; 15(4): 254-6
3. Mente J, Seidel J, Buckalla W, Koch MJ. Electronic determination root canal length in primary teeth with or without root resorption. Int. Endod J.2002; 35(5): 447-52
4. Takushige T, Cruz EV, Asger MA, Hoshino F. Endodontic treatment of primary teeth using the combination of anti bacterial drugs. Int Endod J 2004; 37(2): 132-8
5. Zahid iqbal, Rafeeq Ahmed Menon. Comparison between radiographic and electrical working length determination in root canal treatment in vivo study ISRA Medical journal, 2013 (5): 41-46
6. Cianconi L, Angotti V, Felici R, Conte G, Mancini M. Accuracy of 3 electronic apex locators compared with digital radiography: An ex vivo study. J endod 2010: 36, (12): 2003-7
7. Dagenais M, Hooper S, Kong B, Prusky S, Yip J, .Zahoor H. Electronic apex locaters: an evidence based study. http://www. dentistry. utoronto.ca / system / files / x2_ebl_report.pdf
8. Angwaravong O, Panitvisai P. Accuracy of an electronic apex locator in primary teeth with root resorption. Int Endod J-2009; 42(2): 115-21
9. Ballal S, Gupta T, Kandaswamy D. Management of a retained primary maxillary 2nd molar with c shaped canal confirmed with help of spiral computed tomography- case report. Endodontology. 2006; 18: 14-19
10. M.P.J Gordon, N.P. Chandler. Electronic apex locators. J. International Endodontic Journal, 2004; 37: 425- 437,
11. Nuria Patino-Marin, Norma Veronica Zavala, Gabriel Alejandro Martinez-Castanon, et al. Clinical evaluation of the accuracy of conventional radiography and apex locators in primary teeth. Pediatric Dentistry, 2011; 33(1): 389-392.
12. Bodur H, Odabas M, Tulunoglu O. Accuracy of two different apex locaters in primary teeth with and without root resorption. Clin Oral Invest. 2008; 12(2): 137-41
13. Leonardo MR, Silva LAB, Nelson Filho P, Silva RAB, Raffaini MSGG. Ex vivo evaluation of the accuracy of 2 electronic apex locaters during root canal length determination in primary teeth. Int Endod J 2008; 41(4) :317-21
14. Hassanien EE, Hashen A, Chalfin H. Histomorphometric study of the root apex of mandibular premolar teeth: An attempt to correlate W.L. measured with electronic & radiographic methods to various anatomic position in the apical portion of the canal. J Endod. 2008; 34 (4): 408-12
15. Shahbahang S,Goon WY, Gluskin AH. An in vivo evaluation of root Zx electronic apex locator. J Endod. 1996; 22(11): 616-8
16. Vahid Zand , Hadi Mokhtari , Mehrdad Lotfi et al . Accuracy of working length determination with root ZX apex locator and radiography: An in vivo and ex vivo study . African Journal of Biotechnology .2011 10 (36): 7088-7091.
17. Subramaniam P, Konde S, Mandanna DK. An in vitro comparison of root canal measurement in primary teeth. J. Indian Soc Pedod Prev Dent; 2005; 23(3) ;124-5
18. Aaylin A O , Ali E, Merve E . In vitro evaluation of the accuracy of two electronic apex locators in primary teeth. KU Tip Fak Derg 2010; 12(1): 7-10
19. Sergio Luiz Pinheiro , Iris Nogueira Bincelli , Talita Faria et al. Comparison between electronic and radiographic method for the determination of root canal length in primary teeth. RSBO.2012; 9(1): 11-16
20. Kuttler Y. Microscopic investigation of root apexes. J. Am Dent Assoc 1955 ; 50:544-52
21. Rimondi L, Baroni C.Morphologic criteria for root canal treatment of primary molars undergoing resorption. Dent trauamatol 1995; 11: 136-141
22. Katz A, Mass E, Kaufman AY. Electronic apex locater: A useful tool for root canal treatment in the primary dentition. J Dent Child.1996; 63: 414-7
23. Aghareed Gh. Mohammed. An in vitro comparison of root canal length measurements in primary teeth. Al- Rafidain Dent J 2009; 9( 1):77-82
24. Aqueel Khalil Ebrahim , Reiko Wadachi and Hideaki Suda . Electronic apex locators – A Review . J. Med Dent Sci 2007; 54: 125 – 136
25. Manhal A.R,.Majeed ; Ahmed Gh. . Assessment of the accuracy of a fifth generation apex locator (in vitro study). J. Bagh College Dentistry., 2011:23(1)
26. Mahendra Patel, Manish Shah. Principles of various electronic apex locators and working length determination. Journal of Research and advancement in Dentistry.2012; 1(2) 50-6
27. Anca Popescu, Electronic devices for determining the working length in root canal therapy. 10th International Conference on Development and application systems, Suceava , Romania , May 27-29, 2010:207-10
28. Joe H. Camp, Diagnosis Dilemmas in Vital Pulp Therapy: Treatment for the Toothache Is Changing, Especially in Young, Immature Teeth. Pediatric Dentistry.2008; 30(3): 197-205
29. Goldberg F, Briseno -MarroquinB B , Frajlich S , DreyerC,. In vitro evaluation of the ability of three apex locators to determine the working length during retreatment. J Endod. .2005; 31 (9): 676-8
30. Milad Soruri , Malihe Moeini , Safa Rekabi , Zahra Bahrololumi et al . A clinical comparison of the accuracy of an electronic apex locator (EAL) and radiography in determination of root canal length in primary molars. American journal of research communication.2013; 1 (2): 119-27
31. Keilbassa AM, Muller U, munz I, Mounting JS. Clinical evaluation of the measuring accuracy of root Zx in primary teeth. Oral surg Oral Med Oral path Oral radiol Endod 2003: 95:94-100.
32. Oznurhan F, Ünal M, Kapdan A, Ozturk C, Aksoy S.Clinical evaluation of apex locator and radiography in primary teeth.Int J Paediatr Dent. 2015 May; 25(3): 199-203
33. Ahmad IA, Pani SC.Accuracy of electronic apex locators in primary teeth: a meta-analysis.Int Endod J. 2015 Mar; 48(3): 298-307.
|