Introduction
Predictable, successful endodontic therapy depends on correct prognosis, effective cleaning and shaping, disinfection of root canals and an adequate obturation. The amount of dentin removed during therapy should optimally clean and shape the canals, and subsequent obturation should ensure a tight apical and coronal seal. [1]
The advent of Ni-Ti rotary instrumentation has revolutionized root canal treatment by reducing operator fatigue, time required to finish this preparation, and procedural errors associated with root canal instrumentation.[2], [3], [4], ,[5], [6] The files made from Nickel-Titanium (Ni-Ti) have two to three times more elasticity in bending and corrosion as compared with equivalent designs manufactured from stainless steel. Ni-Ti is also more resistant than stainless steel and can retain its shape after loading.[7]
Endodontic therapy consists of a triad of debridement, disinfection and obturation of root canal system. It has been demonstrated that bacteria remain in the deep portion of root canals even after application of chemical disinfectants.[8] Inability to completely obliterate the irregularities of root canals space with a filling material and to adequately seal the apical foramen has been reported to account for nearly 60% of root canal failures.[9] So obturation can be regarded as one of the most important criteria for success of endodontic therapy. A well done obturation in turn depends on shaping of the canals. Gutta-percha is the most widely used and accepted obturation material due to its inertness, biocompatibility, dimensional stability, compactibility, plasticity when warmed, and ease of removal for post placement and retreatment.[10]
Three popular techniques that utilize three physical properties to obdurate the root canal system are lateral condensation, vertical condensation and warm lateral condensation. Lateral condensation offers the advantage of controlled placement of gutta-percha into the root canal. However, the final root canal filling may lack homogeneity and must rely on sealers to fill the voids between individual cones.[11] Vertical condensation uses heat to produce a homogenous and dimensionally stable gutta-percha mass for obturation of root canal system.[10] However, the improved flow of gutta-percha can result in over-extension of gutta-percha into periapical tissues which can be very time consuming.[12] Warm lateral condensation using an ultrasonically energized spreader (UES) retains the length control of cold lateral condensation while adding the superior ability of a thermoplasticized technique to replicate the three-dimensional shape of root canal.[13] All the rotary Ni-Ti files available today come with a complimentary obturating system. But in the clinical practice owing to cost effectiveness, we are unable to use the effectively. So it becomes necessary to evaluate the conventional obturation techniques in well prepared canals.
The purpose of present study was to compare the fill density obtained by lateral and ultrasonic condensation in canals of distal roots of mandibular molars prepared with 2 Nickel -Titanium rotary systems using Computerized Imaging Method.
Materials And Methods
40 extracted mandibular molars with fully formed apices were taken for the study. A #10-K File was placed in the distal canal until it was just visible at the apical foramen to check patency. Access cavities were prepared using high speed round bur No 4. Pulp tissue was extirpated. For uniform sample preparation, the crowns were sectioned at 14mm from the apex using diamond disc in a slow speed handpiece under copious water irrigation. The roots were separated by cutting perpendicular to the furcation in the same way. Only distal roots were selected for the study, owing to their deviation from round to oval canal shape. Modeling wax was used to cover the apex of the roots and specimens were mounted in dental plaster in form of blocks. The blocks were then trimmed to remove the excess and smoothened. Wax was then removed off.
The 40 specimens were randomly divided into 2 groups of twenty each based on the instrument used for canal preparation.
Group 1: Protaper
Group 2: RaCe
The specimens were held using a custom made jig during preparation. In both groups, EDTA was used as a lubricant and saline as an irrigant during instrumentation. Instruments were used according to manufacturer’s instructions using a gear reduction handpiece (Ni-Ti control; 128:1) with air-motor.
The groups were further divided into two subgroups of 10 each according to the method of obturation using gutta-percha.
Subgroup A- Lateral Condensation
Subgroup B- Ultrasonic Condensation
The root canal sealer used in all specimens during obturation was AH 26 ( Dentsply - Caulk)
Lateral condensation was performed using Ni-Ti finger spreaders. #35 gutta-percha was used as master cone in all the samples. Accessory cones were placed corresponding to #20 and #25 spreaders.
Ultrasonic condensation was performed using ultrasonically energized spreader (UES), SO4 (Suprasson-Satelec). #20 and #25 accessory cones were placed. The tip was activated at power 3-4 as recommended by the manufacturer and holding time for spreader in canals was 15 seconds. Specimens were stored in an incubator at 37S04;C and 100% humidity for 24 hours to simulate oral conditions and allow adequate time for sealer to set.
Cross sectional observation of ability of gutta-percha in each group to obliterate the canal space was carried out to evaluate obturation quality.
Cross sections were performed at three levels after removing the specimens from plaster blocks:
1. 2mm coronal to working length (Apical Cross-section)
2. Half the distance from anatomic apex to coronal surface of the root (Mid-root Cross-section)
3. Two-thirds the distance from anatomic apex to the coronal surface of the root (Coronal Cross-section)
Cross- sectioning was carried out with a diamond disc in a slow speed handpiece under copious water irrigation. Each specimen was examined with an Intra-oral camera with a stabilizer for standardization and measuring software (Schick Technologies).
The obturation quality of each section was evaluated by observing the space or spaces in each section that contained sealer rather than gutta-percha. To objectively compare these observed spaces between the various specimens, the CDR’s on-screen, linear-measuring device was used to measure these spaces on the following criteria.
The maximum linear distance between the gutta-percha mass and the canal wall at any point around the circumference of the gutta-percha mass was measured to the nearest 0.1 mm, as was the maximum measurable linear space within the gutta-percha mass (in cases where such spaces were observed). The larger of the two measurements was recorded for each specimen. In specimens where either no space was observed or where the maximum space observed was less than 0.1 mm, the measurement of that specimen was taken as 0 mm.[14]
Statistical analysis for all data was performed by using either Student independent t-test.
Results
The maximum linear measurement, in mm, of sealer present between gutta-percha mass of Groups 1, 2 (Subgroup A and Subgroup B) are given in Tables 1 and 2 respectively.
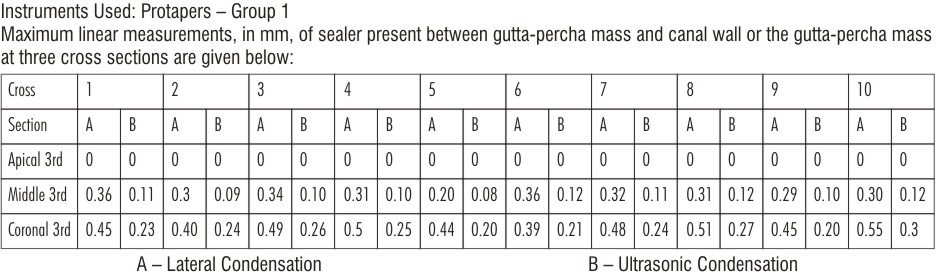 | Table 1
 |
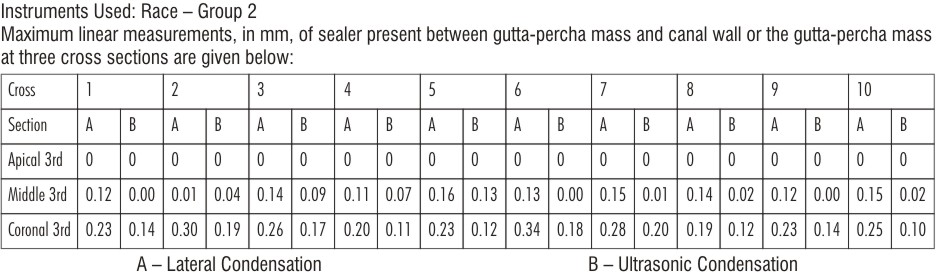 | Table 2
|
The statistical analysis is given in Tables 3, 4 and 5.
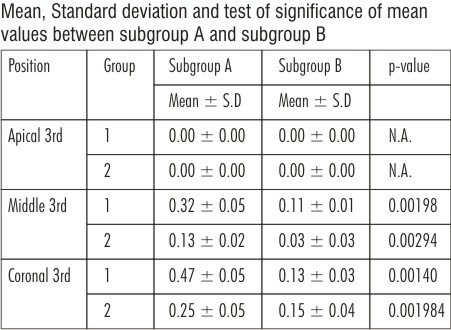 | Table 3
|
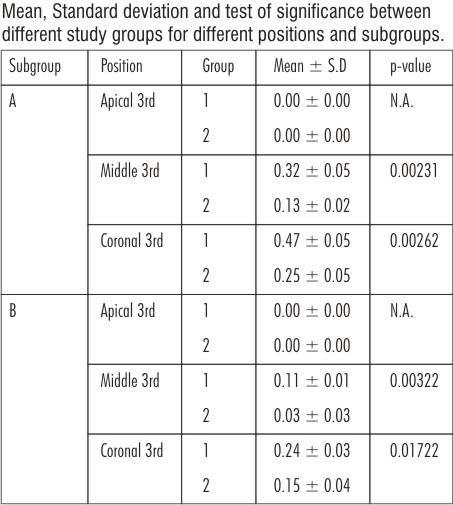 | Table 4
|
 | Table 5
|
The sections of specimens at various levels of cross-section as viewed under the Intra-oral camera are given in Figures 1 - 6.
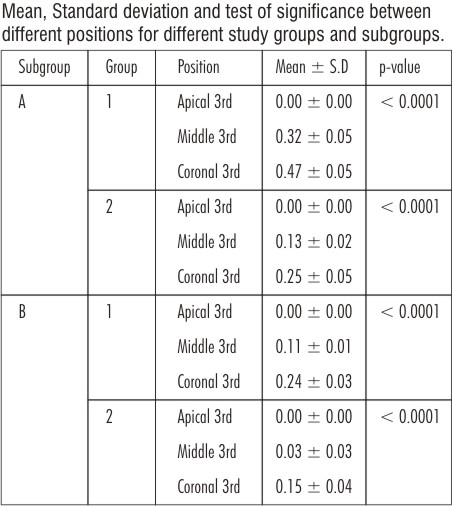
 | Table 5Fig 1 : Lateral Condensation Apical 3rd
|
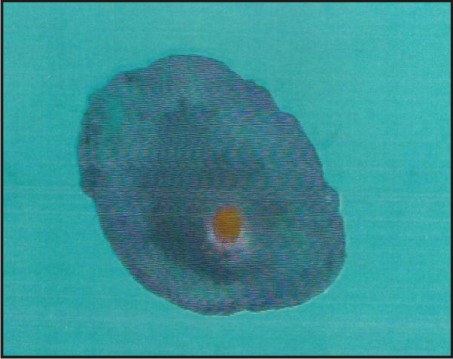
 | Fig 2 : Ultrasonic Condensation Apical 3rd
|
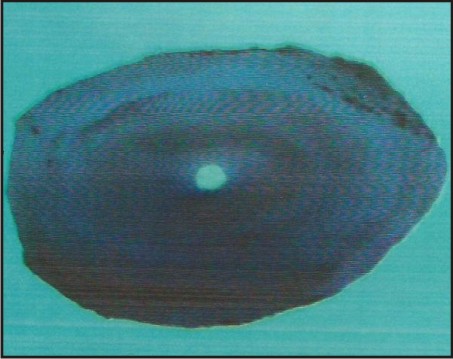
 | Fig 3 : Lateral Condensation Middle 3rd
|
 | Fig 4 : Ultrasonic Condensation Middle 3rd
|
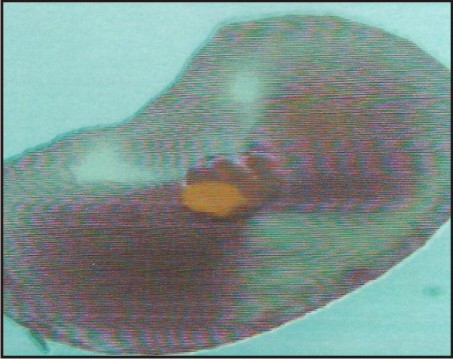
 | Fig 5 : Lateral Condensation Coronal 3rd
|
 | Fig 6 : Ultrasonic Condensation Coronal 3rd
|
Statistical Analysis:
Mean and standard deviation were estimated from the samples for each study group. Mean values were compared by Student Independent t-test.
In the present study p < 0.05 was considered as level of significance.
The Results Showed:
In Group 1, the mean maximum linear measurement was found to be maximum in Subgroup A followed by Subgroup B; and was maximum in coronal third followed by middle and apical third.
In Group 2, the maximum linear measurement was found to be maximum in Subgroup A followed by Subgroup B; and was maximum in coronal third followed by middle and apical third.
When compared among the Groups, it was found that, the mean linear measurement of sealer present between gutta-percha mass and canal wall, or within the gutta-percha mass was found to be maximum in Group 1 for both the subgroups.
The overall results showed that obturation quality was best in Group 2 than in 1.
Ultrasonics gave both three- dimensional and homogenous fill of the canal with gutta percha in both the groups.
Discussion
Endodontic treatment is being performed more commonly and with predictable success in our day to day practice, because of advancement in materials, science and technology. The success of treatment depends upon the endodontic triad i.e. complete elimination of micro organisms from the root canal system, enlargement and three dimensional filling of root canal.[8] Two major causes of endodontic failure, as cited by Washington study, were imperfect obturation and incomplete obturation.[15] Inadequate cleaning and shaping results in incomplete obturation of root canal system.
Incomplete obturation alone contributes to nearly 60% of root canal failure. Therefore, a root canal filling should be a dense, well adapted, three dimensional, with a homogenous mass of core material.[10] Several obturation techniques have been advocated throughout the years for obliterating root canal systems. Cold lateral compaction of gutta-percha points and sealer still remains very popular today. Brayton et al reported this method to produce and non-homogenous filling containing voids between the accessory points and canal walls, as well as many unfilled lateral canals and unequal sealer distribution.[11] Other techniques such as injection moulded, thermo plasticized gutta-percha and thermo mechanical compactions have evolved in an attempt to improve the obturation quality.
Among these methods of root canal filling, the use of ultrasonically energized spreaders (UES) as an aid for lateral condensation of gutta-percha has been proposed. [16], [17] It has been suggested that the energy developed by the UES can be transformed into heat and consequently, the thermomechanical effects produced by the spreader may transform the cones into a more homogenous mass.[8]
Baumgardner K.R. et al in 1990 in a microleakage study revealed significantly better obturations when teeth were filled using UES as compared with manual condensation with fine finger spreader. The reduced apical leakage with UES probably can be attributed to ultrasonic energy plus deeper spreader penetration rather than deep penetration of spreader alone. In using UES, the operator had a distinct impression of using less force on the spreader. The condensed mass had fewer voids and more homogenous lateral condensation.[17]
Alfonso Moreno in 1977 showed considerable improvement in the reduction of leakage by use of thermomechanically softened gutta-percha technique. The ultrasonically activated root canal file could be used as a heat carrier in vertically condensed warm gutta-percha technique.[16] Shaping is a development of logical cavity preparation, which is specific for anatomy of each tooth. The optimum shape is continuous tapering, multi plane cone with the smallest diameter at the apical limit of instrumentation as described by Schilder and Yee in 1984.[19] Achieving an optimal shape is a must for good obturation. Hence, cleaning and shaping has gained more importance and lots of instruments are available for the same.
Following the standardization of endodontic instruments by Ingle and Levine in 1958, the canal preparation was accomplished using carbon- steel reamers. Subsequently, stainless steel instruments were introduced which are relatively inflexible and have a potential hazard of creating canal irregularities during preparation. The rise of developing irregularities increased with the size of instruments and with curvature of roots.[20]
An ideal endodontic instrument should be flexible to allow negotiation of curved root canal, be resistant to fractures and cut efficiently.[21] To overcome these problems, Walia et al introduced a new generation of Nickel-Titanium rotary instruments, which were 2-3 times more flexible stainless steel files due to their low elastic modulus.[22] They also have unique properties like shape memory, corrosion resistance and super elasticity as described by Yeneyama in 1993.[23]
Nearly 30 years ago, Schilder introduced a concept of cleaning and shaping root canals in conical shape and then obturating this space ‘three-dimensionally’ with gutta-percha, warmed in the canal and condensed vertically with pluggers.[10] It was his contention that all the ‘portals of exit’ from the canal be obturated with maximum amount of gutta-percha and minimum sealer. Various root canal filling techniques based on heat and pre-heated gutta-percha have been introduced in order to enhance complete filling of root canal but all these techniques require sealer in adequate sealing of root canals.[24]
Though many techniques are available for obturation as mentioned above, lateral condensation of gutta-percha is the most frequently used, extensively studied and clinically proven of all root canal obturation techniques.[25] Each rotary Nickel-Titanium instrument discussed earlier comes with its own complementary obturating system. But we still use the cold lateral condensation for canals prepared using rotary Nickel-Titanium instruments. However, to date studies are lacking on the effectiveness of this technique in obturating canals prepared with Nickel-Titanium rotary instruments.[14]
The use of Protaper instrument, which has a variable taper, results in canal preparation that tapers from its working length- 7%-5% (for #F1) at coronal extent. The use of conventional lateral condensation technique for obturation of the tapered canal would involve the fitting of an ISO certified gutta-percha cone with an apical to coronal taper of 0.02mm/mm, followed by lateral condensation with hand or finger spreader and addition of numerous gutta-percha cones in an attempt to obturate the space between the master cone and the walls of the prepared canal space.[15] So the efficacy of lateral condensation for canals prepared using rotary Nickel-Titanium instruments is questionable to an extent.
Modern rotary instruments are known to produce round root canals with no or minimal apical transportation. But their efficacy in oval canals still remains elusive. A study by Wu in 2001 reported high prevalence of oval root canals in human teeth.[26] The percentage of root canals that deviate from round shape at 5mm from apex was 56% for distal root canals of mandibular molars and 80% for mandibular incisors.[27]
Since distal canals of mandibular molars have got high prevalence of oval canals, they were selected for the study. All the distal canals of selected teeth were checked for patency using #10 K-file to make sure that there was no canal blockage which would result in alteration of canal procedures. All the distal canals of molars were sectioned 14mm from the apex to have a uniform length. After sectioning, the roots were embedded in plaster blocks so that they could be help with the help of a jig during preparation and can be removed for sectioning again after obturation. Instrumentation was performed in a sequence as per the manufacturer’s instructions for Pro-taper and RaCe. These were run at a slow speed in a gear reduction handpiece.
Marshall and Massler in 1961 suggested that sealer is necessary to improve the apical sealing ability of obturating material.[28] Sealer enhances the possible attainment of impervious seal and serves as filler for canal irregularities and minor discrepancies between the root canal wall and core filling material.[25] Sealers are often expressed through lateral and accessory canals and they can assist in microbial control should there be micro-organisms left in root canal walls or in tubules.[29]
Studies have shown sealer to be weak point in obturation of root canal. Dumsha and Hovland in 1985 demonstrated through microleakage studies that leakage might occur at interface of dentin and sealer, at the interface of solid core and sealer, through sealer itself, or by dissolution of sealer. Leakage does not occur through solid core.[30] Goal of obturation should therefore be to maximize the amount of solid core and to minimize the amount of sealer in prepared canals. AH26 was used as a sealer in this study because as an epoxy resin sealer, it showed superior properties with respect to strength, flow, radiopacity and adhesion.[31] Lateral condensation was performed in the selected canals using Nickel-Titanium finger spreaders. Since #35 gutta-percha was used as master cone in all samples, accessory cones were placed corresponding to #20 and #25 spreaders. The holding time for each subsequent spreader was 20 seconds to allow lateral condensation of gutta-percha.
Ultrasonic condensation was performed using ultrasonically energized spreaders, S04 (Suprasson, Satelec) size 35 gutta-percha was used as a master cone and #20 and #25 accessory cones were placed after subsequent activation of spreader. The tip was activated at power setting 3-4 for a holding period of 15 seconds. This combination produced a rise of root temperature within acceptable limit, which was not detrimental to the periodontium.
G.C. Bailey et all in 2004 have shown increase of 10°C rise in temperature when spreader was activated at power setting 5 and held for 15 seconds. This resulted in root charring and fracture of spreader tip.[32]
The specimens were stored for 24 hours in a humidor for adequate set, so as to lock the gutta-percha cones within the canal that would prevent movement and distortion of gutta-percha during sectioning.[33] As the sealer between canal walls and gutta-percha or between gutta-percha can act as a weak link and eventually lead to microleakage, it was taken to be a void in this study if it was more that 0.1mm in size.[14] The linear measuring device of an intra-oral camera was used to calibrate the distance. Photographs of the cross-section were taken from a standardized distance and image was displayed on to the computer monitor using Schick’s CDR System. Obturation quality for each section was evaluated by observing the space or spaces in each section that contained sealer rather than gutta-percha.
The obtained results indicated overall good three-dimensional fill with ultrasonic compaction as compared to lateral condensation of gutta-percha.
At apical third region of both groups for both sub-groups, the prepared canal spaces in a specimen appeared to contain single gutta-percha cone with minimal or no sealer present at gutta-percha/canal wall interface. In all cases, intimate adaptation of master cone to the prepared canal space presented both spreader penetration and sealing of accessory cones at the level of both lateral as well as ultrasonic condensation. The results were in direct correlation with study by Michael W. Hembrough et all[14], 2002.
At mid-root level, several gutta-percha cones with minimal sealer were evident in cold lateral condensation in group II. Group I showed spaces between cones and could be attributed to the fact that pro-taper, though gave a smooth, tapered canal shape, left large untouched areas in wide canals.[34] Probably the difference in the taper within the same instrument could also have played a role in this. In group II, the taper of instrument is much less and hence the canals were not widened to the extent of other group. Therefore, a good lateral compaction was achieved. The results were in direct correlation with study done by M.W. Hembrough et al[14] No sealer was seen in ultrasonic warm condensation in both groups I and II because heat production thermoplasticizes the gutta-percha and results in providing three dimensional fill as discussed earlier. The results are in direct correlation with study done by Peter and Wollard et al.[35]
At coronal third level, several accessory cones were evident in all the groups and sealer seen in all specimens because both accessory cones and spreaders were able to penetrate to this level several times. Obturation was judged to be complete if a spreader did not penetrate more than 3mm. Michael et all suggested that coronal condensation could not be fully achieved.[14] The same result was seen in our study also.
It is clear from the above discussion that ultrasonic compacting using UES gave a more homogenous mass with little voids as compared to cold lateral compaction. So whenever possible, it is better to use warm lateral condensation.
Conclusion
Under the conditions of study, it can be concluded that:
- Ultrasonic compaction (warm lateral condensation) produced a more homogenous, three dimensional obturation when compared to cold lateral condensation.
- Optimal obturation was achieved in canals prepared with RaCe when compared to Protapers.
- Conventional obturating systems using ISO standardized gutta-percha can effectively substitute complementary obturating systems of corresponding Nickel-Titanium instruments.
References
1. Pia Deplazes, DVC Peters and Fred Barbakow. Comparing apical preparations of root canals shaped by Nickel-Titanium Rotary instruments and Nickel-titanium Hand instruments. J Endod 2002;27:196 – 202.
2. Glossan CR, Haller RH, Dove SB, Del Rio CE. A comparison of root canal preparations using Nickel-Titanium engine- driven and K-Flex endodontic instruments. J Endod 1995;21:146 – 151.
3. Short JA, Morgan LA, Baumgardner JC. A comparison of canal centering ability of four instrumentation techniques. J Endod 1997;23:503 – 07.
4. Brynt ST, Thompson SA, Al Omari MAO, Dummer PMH. Shaping ability of profile rotary Nickel-Titanium instruments with ISO sized tips in simulated root canals. Int Endod J 1998;31:275 – 81.
5. Gambil JM, Aldes M, Del Rio CE. Comparison of Nickel-Titanium and stainless steel hand file instrumentation using Computed Tomography. J Endod 1996;22:369 – 75.
6. Park HA. Comparison of greater taper files, profiles and stainless steel files to shape curved root canals. Oral Surg Oral Med Oral Path Oral Radiol Endod 2001;9:715 – 18.
7. Ponti M, McDonald J, Sergio Kuttler, Howard C Stzassler and James C Dumsha. Canal centering ability of two rotary file systems. J Endod 2002;28:283 – 86.
8. Matsumiya S, Kitamura M. Histopathological and histobacteriological slides of relation between the condition of sterilization of the interior of root canal and healing process of periapical tissues in experimental infected root canal treatment. Bull Tokyo Coll 1960;1:1 – 19.
9. Dow PR, Ingle JL. Isotope determination of root canal failure. Oral Surgery 1955;1100 – 04.
10. Schilder H. Filling root canals in three- dimensions. Dent Clin North Am 1967;11:723 – 44.
11. Bryton SM, Daris SR, Goldman M. Gutta – percha root canal fillings, an in-vitro Part I. Oral Surg 1973;35:226 – 31.
12. Budd CS, Weller RN, Kulid JC. A comparison of thermoplasticized injectible gutta- percha obturation techniques. J Endod 1986;12:139 – 45.
13. Alexander K. Deitch, Frederick R. Liewehr, Lesley A. West, William R. Patton. A comparison of fill density obtained by supplementing cold lateral condensation with Ultrasonic condensation. J Endod 2002;28:665 – 67.
14. Micheal W. Hembrough, Robert Steiman, Kimberly K. Belanger. Lateral condensation in canals prepared with Nickel-Titanium rotary instruments: An evaluation of the use of three different master cones. J Endod 2002;28:516 – 19.
15. John I Ingle and John David West. Obturation of radicular space: Ingle & Bakeland ed. Endodontics: 54th Edition: 223 – 319 Philedelphia.
16. Moreno A. Thermomechanically softened gutta-percha root canal filling. J Endod 1977;3:186 – 88.
17. Baumgardner KR, Krell KV. Ultrasonic condensation of gutta-percha: an in-vitro dye penetration and scanning electron microscope study. J Endod 1990;16:253 – 59.
18. Zmener O, Banegas G. Clinical experience of root canal filling by ultrasonic condensation of gutta-percha. Endod Dent Traumatol 1999;15:57 – 59.
19. Schilder H, Yee FS. Canal debridement and disinfection. Cohen S, Burns RC: Pathways of Pulp, 3rd Edition. Mosby Company.
20. Shankar P, Parmeshwaran A, Lakshmi Narayanan L. Apical third instrumentationof curved canalswith K- type and canal master instruments. J Endod 1993;19:224 – 27.
21. Camps IJ, Petrot WJ. Machining effect of Ni-Ti, K-type files in linear motion. Int Endod J 1995;28:279 – 84.
22. Walia H, Brantley WA, Gerstein H. An initial investigation of bending and torsional properties of NiTi root canal files. J Endod 1988;14:346 – 51.
23. Pilo R, Corcino G, Tamse A. Residual dentin thickness in mandibular premolars prepared with hand and rotary instruments. J Endod 1998;24:401 – 4.
24. R.T.G Moor, G.M.G. Hommez. The long-term sealing ability of an epoxy resin root canal sealer used with five gutta-percha obturation techniques. Int Endod J 2002;35:631 – 36.
25. Gutmann JL, Witherspoon DE. Obturation of the cleaned and shaped root canal system. Cohen S, Burns RC, eds. Pathways of Pulp. 7th Ed. St. Louis: CV Mosby: 258 – 361.
26. Wu MK, Wesselink PR. A primary observation on the preparation and obturation of the oval canals. Int Endod J 2001;34:137 – 41.
27. T. Rodig, M. Hulsmann, M. Muhge, F. Schafers. Quality of preparation of oval distal root canals in mandibular molars using Nickel-Titanium instruments. Int Endod J 2002;35:919 – 28.
28. Marshall FJ, Massler M. the sealing of pulpless teeth evaluated with radio-isotopes. J Dent Med 1961;16:172 – 84.
29. Al Khatibb ZZ et al. The antimicrobial affects of various endodontic sealers. Oral Surg Oral Med Oral Path Oral Radiol Endod 1990;70:784 – 89.
30. Hovland EJ, Dumsha TC. Leakage evaluation in-vitro of root canal sealer cement sealapex. Int Endod J 1985;18:179 – 82.
31. Dorothy McComb, Dennis C Smith. Comparison of physical properties of polycarboxylate based and conventional root canal sealers. J Endod 1976;2:228 – 35.
32. G. C. Bailey, S.A. Cunnington, K. Gulabiwala, D.J. Setchell. Ultrasonic condensation of gutta-percha: the effect of power setting and activation temperature rise at the root surface- an in-vitro study. Int Endod J 2004;37:447 – 54.
33. Fuzz Z, Charniaque O, Pilo R, Weiss E. Effect of various mixing ratios on antibacterial properties and hardness of endodontic sealers. J Endod 2000;519 – 22.
34. O. A. Peters, C. I. Peters, K. Schonenberger, F. Barbakow. Protaper rotary root canal preparation: effect of canal anatomy on the final shape analyzed by micro CT. Int Endod J 2003;36:86 – 92.
35. Wollard RR, Brough SO, Maggio J, Seltzer S. Scanning electron microscopic examination of root canal filling materials. J Endod 1976;2:98 – 110.
|