Introduction
In the anterior region of the mouth, the labial cortical plate over the natural teeth is much thinner than its lingual counterpart. Periodontal disease creates infrabony defects on the lingual aspect of the supporting bone but often causes complete loss of the labial alveolar process. Dehiscence of the labial plate may also occur as a consequence of tooth eruption orthodontic therapy, parafunction, trauma, vertical root fracture, apicectomy, ill-fitting crown margins, subgingival tooth preparation and extractions. The facial plate of bone is also first to remodel or resorb after tooth extraction, disease, or trauma and it does so to a greater extent than the lingual cortical bone.[1]
In the anterior maxilla, the alveolar bone is rapidly re countered after the loss of the natural teeth, even in the presence of an intact alveolus after extraction. There is 25% decrease in volume during the first year and 40% to 60% decrease in width within the first 3 years after tooth loss[1], [2]. Bone resorption in the maxillary ridge frequently results in a knife edged deformity, which complicates implant placement and stabilization. Grafting with autogenous bone has been documented to be highly effective in reconstructing jaw anatomy[3], [4].
Case Report
A 23year old female dentist reported to our clinic with complaint of mobility and pus discharge with upper right central incisor region. She had a history of trauma and horizontal fracture of tooth. A root canal treatment was done as its management 3 years back. On radiographic examination the root of upper central incisor was completely resorbed and periapical radiolucency was present in relation to the tooth. Hence, the central incisor was extracted and curettage of socket was done. An intermediate temporary prosthesis was placed and patient was planned for implant surgery and recalled after 3 months for implant placement. After 6 months radiographic examination was done to estimate the bone formation and to estimate the length of implant to be placed [Fig 1, 2].
Surgical protocol followed under local anesthesia [lignocaine 2% with 1:80,000 adrenaline] with all aseptic precautions.
 | Fig-1 : Preoperative View
 |
 | Fig-2 : Preoperative Iopa X-ray
|
Stage-I
Flap design- A trapezoidal flap with palately placed horizontal incision to expose the implant site [Fig 3]. The horizontal incision was placed palately to avoid the incision to be on implant and also the flap completely covers the implant.
Direct implant site revealed a thin residual ridge which required bone grafting. A buccal cortical plate dehiscence was noticed while drilling the implant site. An implant of size 3.75Dx13L [ADIN, Tourage] was placed. An autogenous bone graft was taken from the buccal cortex of the adjacent pyriform aperture area. The buccaly exposed implant was covered with composite graft of buccal cortical chip and xenograft [perioglass] [Fig 4]. A GTR barrier membrane was placed and secured with tie sutures on palatal and labial periostium. The flap was closed with 3-0 vicryl suture.
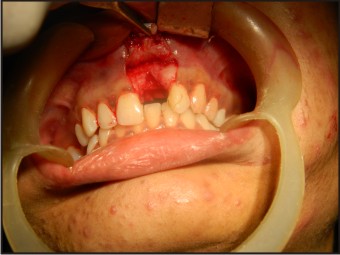 | Fig-3 : Trapezoidal Incision With Palataly Placed Horizontal Incision
|
 | Fig-4 : Composite Graft Placed Over Buccaly Exposed Implant
|
Stage-II
After six months the uncover surgery was performed and a healing cap placed to develop the emergence profile of the prosthetic component [Fig 5].
![Fig-5 : Healing After Placement Of Healing Cap[6 Month Post Op]](article-image-5240-FIG_5_HEALING_AFTER_PLACEMENT_OF_HEALING_CAP[6_MON.jpg) | Fig-5 : Healing After Placement Of Healing Cap[6 Month Post Op]
|
Prosthetic phase
A 15o abutment was placed due to deep bite [Fig 6]. A closed tray impression was taken [Fig 7] and porcelain fused to metal crown was placed. A composite build up of adjacent tooth was done to develop contact areas [Fig 7].
 | Fig-6 : 15 Degree Abutment In Place
|
 | Fig-7 : Closed Tray Impression
|
 | Fig-8 : Aesthetic Crown With Composite Restoration
|
Follow up
The patient was followed up for 1 year with good implant stability. A esthetic gingival graft surgery was further planned to develop esthetic inter-dental papilla between the central incisors.
Discussion
Autogenous bone grafts are considered as a gold standard and predictable regeneration is achievable due to its potential osteogenic property. Furthermore it has been shown that in the facial skeleton, membranous bone such as that harvested from mandible undergoes less resorption than endochondral bone[5],[6]. Intraoral block bone grafting is a predictable operation with high success rate for long span augmentation up to complete jaw augmentation or extensive bone reconstruction of maxillary alveolar ridges[7]. Autogenous bone grafting using blocks of bone obtained intra orally or extra orally are widely considered the best approach to augment deficient alveolar ridges[8], [9], [10]. Composite bone grafts have been used for implant bone grafting with success[11]. This composite bone grafts can serve as a blend of osteogenic bone and osteoconductive graft particle.
Hence, composite graft can serve as a viable alternative to the completely autogenous bone graft.
References
1. Carlsson GE, Thilander H, Hedegard B: Changes in contour of the maxillary alveolar process after extractions with or without insertion of an under immediate full denture, Acta Odontol Scand 25:21-43, 1967.
2. Pietrokovski J, Massler M: Alveolar ridge resorption following tooth extraction, J Prosthet Dent 17:21-27, 1967.
3. Burchard H.Biology of bone transplantation. Orthop Clin North Am.1987; 18:187-95.
4. Marx RE. Biology of bone grafts. In:Kelly JPWed. OMS Knowledge Update. Rosemount, IL:American Association of Oral and Maxillofacial Surgeons; 1994:RCN;3-17.
5. Zins JE, Whittacker LA. Membranous versus endochondral bone autografts: Implication for craniofacial reconstruction.Plast.Reconstr.Surg 1983;72:778-86.
6. Phillips JH, Rhan BA. Fixation effects on membranous and endochondral onlay bone grafts vascularisation and bone deposition. Plast.Reconstr. Surg 1990;85:891-7
7. Schwrtz-Arad D, Lwin L. Intraoral autogenous block onlay bone grafting for extensive reconstruction of atropic maxilary alveolar ridges. J periodontal 2005; 76:636-41.
8. Misch CM. Comparison of intraoral donor sites for onlay grafting prior to implant placement. Int.J Oral Maxillofac implants 1997; 12:767-76.
9. Misch CM. Use of the mandibular ramus as a donor site for onlay bone grafting. J Oral Implantol 2000; 26:42-9.
10. Misch CE, Dietsch F. Endosteal implants and iliac crest grafts to restore severly resorbed totally edentulous maxilla- A retrospective study. J Oral Implantol 1994; 20:100-10.
11. Direct sinus elevation and composite bone grafting for immediate implant placement in the posterior maxillary region. Nettemu Sunil Kumar, R Soumya. J of Dental implants 2011; 1:29-33.
|