Introduction:
Radicular cyst is the most common odontogenic cyst occurring in the periapical area of any teeth. The majority of the cases of radicular cysts are asymptomatic and associated with the non vital tooth.[1] The cyst comprises about 52 to 68% of the jaw cysts.[2] The peak incidence is in the 3rd and 4th decades of life with more male predilection.[3] Most commonly the cyst occurs in the maxillary than in the Mandibular region.[4] We present a rare case of painful multiple radicular cysts in a 35 year old female patient.
Case Report:
A 35 year old female patient reported to the department of Oral Pathology with the chief complaint of pain in the lower and the upper anterior region of the jaw. The patient noticed the swelling about five months back and pain in the same region about three months back. The pain was intermittent and dull in nature and exaggerated during mastication and on lying down. The past medical and dental history was not relevant. On extra oral examination the Submandibular lymph nodes on the left side were palpable. Intra oral examination revealed severe attrition with respect to 21, 22, 23, 31, 32, 33, 34, 35, 41, 42 & 43. Examination of the lesion proper in mandible revealed swelling extending from mesial of 33 to the distal aspect of 35. In maxilla the swelling was present on the palatal and labial aspect. Palatally it extended from gingival margin to the mid portion of the mid palatal raphae, with a smooth surface and associated with tenderness. Labially it extended from the gingival margin to the labial vestibule, with smooth surface and associated with tenderness. All the swellings were oval in shape, with smooth surface and diffuse borders. The orthopantamograph (Figure-1) in maxilla showed single unilocular radioluscency associated with the roots of 21, 22 and 23. In mandible it showed the multiple unilocular radioluscency associated with 33, 34 & 35, 42 & 43. The hematological examinations were under normal range. Based on the clinical and radiological examination provisional diagnosis of Radicular cyst was given. All the lesions were excised and put for histopathological examination. Macroscopically (Figure-2) each specimen was measuring about 2x1.4cm, 0.8x0.5cm, 0.7x0.5cm and 0.5x0.6cm respectively, soft in consistency, cream to brown in color with irregular margins. The H&E stained section (Figure - 3 & 4) showed the presence of parakeratinised stratified squamous epithelium and the connective tissue components. The epithelium was of 3 to 5 layers thick and showed long elongated rete ridges showing arcading pattern. The connective tissue just below the epithelium showed presence of dense chronic inflammatory cell infiltrates mainly the lymphocytes. Other part of the connective tissue reveals the haphazardly arranged collagen fiber bundles and blood vessels with extravasated RBC’s. The overall features were suggestive of Radicular cyst.
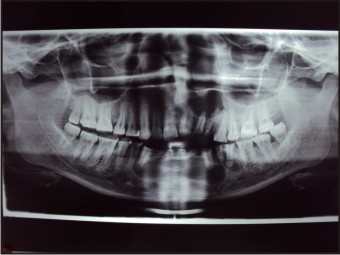 | Figure-1: Orthopantamograph
 |
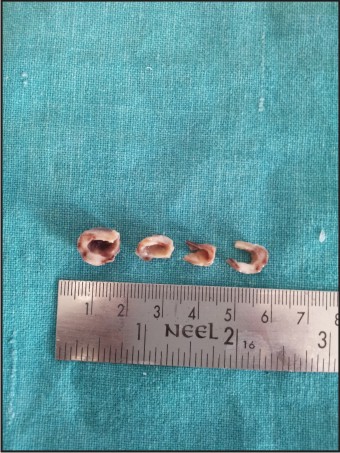 | Figure-2: Grossed Specimen
|
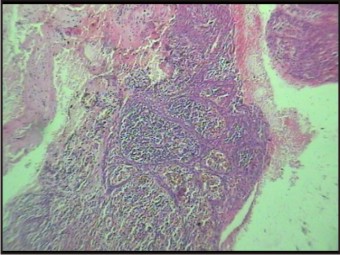 | Figure-3: Arcading Pattern Of The Epithelium
|
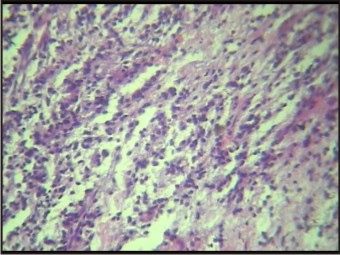 | Figure-4: Dense Inflammatory Cell Infiltrate In The Connective Tissue
|
Discussion:
Radicular cyst is usually associated with carious, non vital, discolored or fractured tooth.[5] Due to the inflammation of the periradicular tissues there will be proliferation of the epithelial cell rests of malassez, which will further undergo cystic degeneration resulting in radicular cyst.[6] The size rarely exceeds 1 cm and is often seen in patients between30 and 50 years old with higher incidence in the maxillary anterior region.[7]
Since the radicular cyst is associated with a non vital tooth, the patient may present with current or prior symptoms of tenderness, pain, swelling or drainage in the affected area. However many periapical cysts are asymptomatic, being discovered only during routine radiographic examination. But the present case came with the complaint of pain and swelling in the anterior maxilla and mandibular region. Most of the radicular cysts are 2cm or less in size, although occasional lesions may demonstrate dramatic enlargement with destruction of a significant portion of the jaw.
The radicular cysts are lined by stratified squamous epithelium that is often irregular and proliferative in nature with arcading of the rete ridges. Since the epithelium may exhibit extensive areas of ulceration, some radicular cysts may show only focal remnants of the epithelial lining. Mucous cells are identified in up to 40% of radicular cysts.[8]
Several treatment options are available for a radicular cyst such as surgical endodontic treatment, extraction of the offending tooth, enucleation with primary closure, and marsupialization followed by enucleation.[1] In this case, surgical enucleation was preferred and was performed uneventfully.
Conclusion:
Radicular cyst is a very common condition in the oral cavity. However occurrence of multiple radicular cysts is a rare finding. So the present case was reported with multiple radicular cysts occurring in mandible and maxillary anterior region.
Reference:
1. Shafer HL. 6th ed. Amsterdam: Elsevier; 2006. Textbook of Oral Pathology.
2. Nair PN. Review New perspectives on radicular cysts: Do they heal? Int Endod J. 1998; 31:155–60.
3. 3rd ed. Singapore: Varghese Publication House; 1992. Mervyn Shear, Cysts of oral regions; pp. 136–70.
4. Rees JS. Conservative management of a large maxillary cyst. Int Endod J. 1997; 30:64–7.
5. Scholl RJ, Kellett HM, Neumann DP, Lurie AG. Cysts and Cystic Lesions of the Mandible: Clinical and Radiologic-Histopathologic Review. Radiographics. 1999; 19:1107–24.
6. Lin LM, Huang GT, Rosenberg PA. Proliferation of epithelial cell rests, formation of apical cysts, and regression of apical cysts after periapical wound healing. J Endod. 2007; 33:908–16.
7. Weber AL. Imaging of cysts and odontogenic tumors of the jaw. Radiol Clin North Am. 1993; 31:101–20.
8. Gnepp D. Saunders Company; 2001. Diagnostic Surgical Pathology of the Head and Neck.
|