Introduction
To overcome clinical problems of distal extension dentures, single implants placed bilaterally allow reducing the potential for denture dislodgement and providing aesthetically acceptable prosthetics.[1],[2] It has been reported that freestanding single dental implants can be used to resolve problems with bilateral distal extension removable partial dentures in a cost-effective manner.[3], [4]
Although implant-retained partial overdentures with attachments provide a convenient treatment approach, several clinical factors must be considered. The position and number of implants must be determined by prosthetic requirements, but anatomic limitations in many situations can also affect outcomes. Therefore, clinical judgment should be used carefully for selecting appropriate attachments both before and after the installation of surgical implants. In particular, careful evaluation of available restorative space in relationship with the localisation and orientation of the implants is essential when selecting attachments.[5], [6]
The main properties to be considered in this selection are:[7]
Size : Attachment selection is often guided by the amount of space available and should be evaluated at the diagnostic stage. Adequate space should be provided to accommodate abutment height as well as minimum occlusal thickness for resin and artificial teeth. In the case of problems caused by limited interocclusal, it is necessary to provide a system that provides a less vertical height attachment.
Angulation compensation and alignment correction: Compensation is provided by angulated abutments or can be built into the attachment design to allow for use with nonparallel implants without additional parts.
Resiliency : In order to allow for distal extension, resilient attachments are required to provide stress relief.
For certain implant systems, the overdenture attachments available in the catalogue are limited to one abutment design, generally a ball abutment. In case of limited restorative space, an over-voluminous attachment leads to the fabrication of a structurally weak prosthesis with an aesthetic compromise[6]. To overcome the problem, a shorter abutment with the possibility for correcting or tolerating implant angulation is needed. This article describes a simple technique to make a custom-made cast abutment in a situation with RPD and limited interocclusal space.
Technique
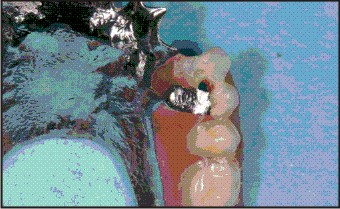
In the situation reported, two attachments placed on maxillary right and left premolars sites with a limited restorative space caused perforation of the occlusal surface of the artificial teeth (Fig. 1A) (Fig. 1B).
 | Fig 1a
 |
 | Fig 1b
|
To overcome the problem a cast to abutment (Friadent Aurobase 45-2440, Dentsply, Friadent,Germany) and a Locator attachment (Locator, Zest Anchors LLC, Escondido, CA., USA) were provided, and the following procedure was performed:
1. Make an implant level impression with copings (Friadent Transfer Coping with Standard Abutment Screw And Friadent Transfer Cap 45-1640 ;Dentsply Friadent) and polyvinyl siloxane impression material (Dentsply Caulk, Milford, Germany) with a stock tray.
2. Connect implant analogues (Frialit Internal Hex Implant Analog45-4040Dentsply Friadent, Germany) to impression copings (Friadent Transfer Coping with Standard Abutment Screw and Transfer Cap 46-1640, Dentsply, Friadent, Germany) and pour the final cast with type IV dental stone (Denstone; Heraeus Kulzer, South Bend, Ind), including a soft tissue replica.
3. Make a cast of the opposing arch and mount the casts on a semi-adjustable articulator using occlusal rims over the laboratory analogues.
4. Fit a cast to the abutment on the analogue implants and cut the waxing sleeves down to the gingival level (Fig. 2A).
5. Cut the threaded part of a Locator abutment (or matrix) (Locator, Zest Anchors LLC, Escondido, CA, USA) with a separating wheeland perforate thecenter of the abutments with a bud bur to form an entry for a separate abutment screw.
6. Duplicate the modified Locator matrix in castable resin (Duralay, Reliance Dental Mfg., Worthington, IL, USA) and wax it to the cast to abutments (Fig. 2B).
7. Attach the wax patterns to sprue formers, invest and cast in noble alloy (V-Classic, Cendres et métaux, Bienne, Switzerland).
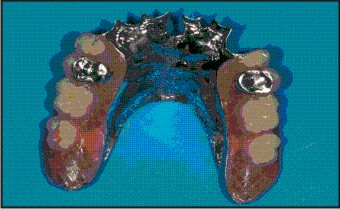
8. Finish the custom-made cast abutment, insert and tighten the abutment screw to the recommended torque (Fig. 3a, b).
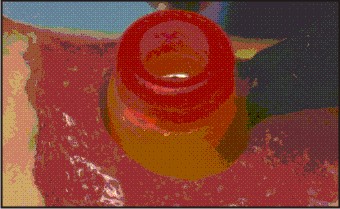
9. Insert the patrix (denture cap processing male component) of the attachment in the intaglio of the RPD (Fig. 4) with a chair side pick-up procedure or process the denture component at the laboratory according to the manufacturer's instructions.
10. Remove the processing male component from the denture cap and replace it by a nylon male component that can accommodate a divergent implant up to 20° (Zest order #8527, Zest anchors). Choose the male component (green, orange or red) according to the level of retention desired.
 | Fig 2a
|
 | Fig 2b
|
 | Fig 3a
|
 | Fig 3b
|
 | Fig 4
|
Discussion
This technique provides a solution for limited interocclusal space situations in an implant supported removable partial denture. It is indicated when the shape, width or length of the machined attachment available in the implant system is incompatible with the available restorative space.[6]
The cylindrically designed attachment used with the prefabricated cast-to component, was reported to have the smallest vertical profile available and allow for up to 40° compensation between abutments.[5] In addition, repair and replacement are quick and easy.[7] Thus, it is considered to be suitable for managing a large number of clinical situations, especially those with limited restorative space and/or angulated implants in an implant supported removable partial or complete overdenture.
A limitation of this technique is that the custom abutment is screwed along the implant axis and angulation correction with the castable resin component is limited. However, specific nylon male components that snap onto the custom-made abutment are designed to accommodate for divergence, making it possible to implement them in the case of poor parallelism between the implant axis and the RPD path of insertion.
Summary
This report describes a technique for making a custom attachment combined with an RPD to correct a situation in which the restorative space was too limited for a standard machined abutment. This technique avoids using prostheses over contours due to the volume of inappropriate abutments and reduces maintenance.
References
1. Uludag B, Celik G. Fabrication of a maxillary implant-supported removable partial denture: a clinical report. J Prosthet Dent 2006; 95:19-21.
2. Grossmann Y, Levin l, Sadan A. A retrospective case series of implants used to restore partially edentulous patients with implant-supported removable partial dentures: 31-month means follow-up results. Quint Int 2008; 39:665–671.
3. Kuzmanovic DV, Payne AG, Purton DG. Distal implants to modify the Kennedy classification of a removable partial denture: a clinical report. J Prosthet Dent 2004; 92:8-11.
4. Mijiritsky E, Ormianer Z, Klinger A, et al. Use of dental implants to improve unfavourable removable partial denture design. Compend Contin Educ Dent 2005; 26:744–6.
5. Chaimattayompol N, Arbree NS. Assessing the space limitation inside a complete denture for implant attachments. J Prosthet Dent 2003; 89:82-5.
6. Ahuja S, Cagna DR. Defining available restorative space for implant overdentures. J Prosthet Dent 2010; 104:133-6.
7. Chikunov I, Doan P, Vahidi F. Implant-retained partial overdenture with resilient attachments. J Prosthodont 2008; 17:141-8.
|