Introduction:
Transposition refers to the development and eruption of a permanent tooth in a position normally occupied by another permanent tooth[1]. Transposition can be either complete or incomplete. In case of complete transposition both the crowns and the entire root structure of the involved teeth are found parallel in their transposed positions whereas in incomplete transposition the crowns may be transposed while the root apices remain in their normal positions[1]. Alternatively the crowns may be in the correct order while the root apices may be transposed. The etiology of maxillary canine - first premolar transposition appears to involve genetic influences within the multifactorial model[2]. Transposition affects both sexes however females are more commonly affected than males[2]. Also, unilateral transpositions are common as compared to bilateral with a predilection for the left side[3]. Treatment planning for this anomaly is based on the decision whether to maintain the transposed tooth order or correct it. This article will describe correction of a case of unilateral complete transposition.
Diagnosis:
The patient was a normally developing 10 year old female in mixed dentition, with a retrusive mandible and slightly deficient anterior facial height (Fig-1a). She had a large midline diastema, (Fig-1b), missing maxillary lateral incisors and complete transposition of right maxillary 1st premolar and canine (Fig-1c). Molar relation was Class I with normal overjet and overbite. Maxillary molars were rotated mesially. Mandibular arch had a mild arch length discrepancy.
 | Figure 1a – 10 Year Old Female Patient Withretrusive Mandible And Slightly Deficient Anterior Facial Height.
 |
 | Figure 1b – Study Models In Mixed Dentition Stage Showing Large Midline Diastema.
|
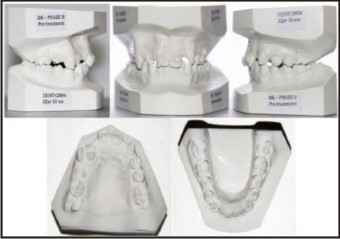 | Figure 1c – Study Models In Permanent Dentition Stage Showing Missing Maxillary Lateral Incisors And Complete Transposition Of Right Maxillary 1st Premolar And Canine. Midline Diastema Has Been Closed.
|
Panoramic radiograph (Fig-2) showed that permanent maxillary lateral incisors were missing, and an unusual tooth position in the region of right permanent maxillary first premolar and canine: a unilateral canine-first premolar transposition. With Clark’s tube shift method4 it was established that the root of maxillary canine was placed buccal to the roots of maxillary first premolar.
 | Figure 2 - Panoramic Radiograph Showing Missing Permanent Maxillary Lateral Incisors , And An Unusual Tooth Position In The Region Of Right Permanent Maxillary First Premolar And Canine: A Unilateral Canine-first Premolar Transposition. The Lateral Cephal
|
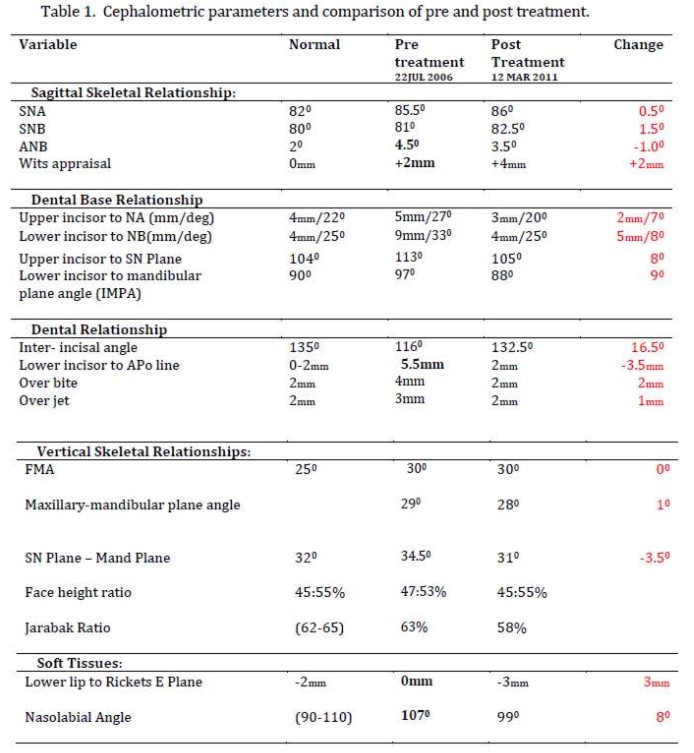
The cephalometric (Fig-2) analysis revealed prognathic maxilla and a relatively retrognathic mandible and an ANB angle of 4.50. Maxillary and mandibular incisors were proclined. The Frankfurt mandibular plane angle showed vertical growth direction (Table-1).
 | Figure 3 – (A) Open Coil Spring For Mesial Movement Of 13., (B) Initially Thetransposed First Premolar (14) Was Bonded Lingually And Was Tied With An E-chain To Transpalatal Arch To Move It Distally And Palatally, Away From The Path Of Canine., (C) 14 Was
|
Treatment Objectives:
The treatment objectives were to (1) close midline diastema (2) correct the transposed canine and first premolar (3) close the missing maxillary lateral incisor spaces in the upper arch and subsititute canines for laterals (4) correct dentoalveolar protrusion (5) control vertical dimension and (6) maintain the facial balance.
Treatment Progress:
The treatment was done in two phases
A 2×2 appliance was given in the first phase of treatment. Midline diastema was closed with e chain.
In the second phaseit was decided that transposition would be corrected first followed by closure of spaces and reshaping of maxillary canines. In the mandibular arch it was decided to extract 1st premolars and close the spaces. Preadjusted 022 slot Roth straight wire appliance was bonded. A transpalatal arch was given to maintain anchorage and correct molar rotation. The initial wires were 016 Ni Ti, 17×25 Ni Ti and 17×25 SS wire. Open coil spring was placed on the right side between the 1st molar and the transposed maxillary canine to move the canine mesially. Right second premolar was not bonded at this time. The transposed first premolar was bonded lingually and was tied with an e-chain to transpalatal arch to move it distally and palatally, away from the path of canine when the canine completely moved mesially, the 1st premolar was bonded bucally and derotation ties were given lingually and bucally (Fig-3). Throughout this period left side missing lateral incisor space was maintained with the help of an artificial tooth which was attached to the arch wire via a lateral incisor bracket. Once the transposition was corrected successfully the next phase of treatment started which involved space closure in the upper arch (missing lateral incisor space) and 1st premolar extraction and space closure in the lower arch. The bonding in the lower arch was done at this stage. Space closure in the upper arch was done with T loops. Lower spaces were closed by niti closed coil springs. After 30 months of the beginning of active treatment, the fixed appliances were removed, and a removable retention appliance was placed in the upper arch. A .0195- in coaxial stainless steel fixed retainer was bonded to the cingula of the mandibular anterior teeth.
 | Figure 4 - The Maxillary Canines And The First Premolar Were Successfully Positioned And Proper Alignment And Tooth Position Were Obtained.
|
Results:
The maxillary canines and the first premolar were successfully positioned and proper alignment and tooth position were obtained. All spaces were closed. Ideal overjet and overbite were also achieved. Canines were reshaped to look like laterals. Class I molar relationship and facial balance was maintained (Fig-4).
 | Figure 5 - Final Radiographs Showed Root Parallelism And No Evidence Of Root Resorption.
|
Discussion:
The main difficulties in correcting the altered tooth position with maxillary premolar-canine transposition are avoiding root interference, root resorption, and controlling root position of the transposed teeth.[2] In this case there was an additional finding of missing lateral incisors which further complicated the case. The question here was whether to maintain the lateral incisor space and later place implants or to close the space and reshape canines. On evaluation it was found that the space was insufficient for the placement of implants and dentoalveolar protrusion needed to be corrected therefore it was decided to close the space and then reshape the maxillary canines to make the appearance esthetically acceptable. The patient also was keen to have the spaces closed and avoid prosthodontic replacement.
The first premolar was initially moved palatally to avoid any interference with mesial movement of canine. The canine was moved mesially by using an open coil spring between canine and first molar. The coil spring also helped conserve anchorage as it counteracted the mesial force of e chain which was being used to move the premolar palatally and distally. Thus simple mechanics used with a complete understanding of the action and reaction can help correct most difficult cases. The 1st premolar root was dilacerated which was an unfavorable finding to carry out such major root movement but on the other hand the proximity of central incisor and premolar was undesirable and not a very esthetic solution.
Final Radiographs (Fig-5) showed root parallelism and no evidence of root resorption even though the premolar had been moved a considerable distance and dilaceration of the root was present. Proper clinical assessment and careful treatment planning are a must for treating this type of case of maxillary canine 1st premolar transposition.
 |
|
References:
1. Shapira Y, Kuftinec Mm. Maxillary canine-lateral incisor transposition-Orthodontic management. Am J Orthod Dentofacial Orthop 1989; 95:439-44.
2. Peck L, Peck S, Attia Y. Maxillary canine- first premolar transposition, associated dental anomalies and dental basics. Angle Orthod 1993; 63:99-109.
3. Peck S, Peck L. Classification of maxillary tooth transpositions. Am J Orthod Dentofacial Orthop 1995; 107:505-17.
4. Clark CF. A method of ascertaining the relative position of unerupted teeth by means of film radiographs. Proc R Soc Med Odontol Sectn 1910; 3: 87-90.
|