Introduction
One of the main objectives of nonsurgical endodontic treatment is the elimination of infection from the root canal system and prevention of reinfection of the root canal system.[1] The success of root canal therapy depends on the accurate knowledge of the root canal system.[2] Many of the problems encountered during and after root canal treatment occurs because of inadequate understanding of pulp space anatomy. Current knowledge of pulp space anatomy is based on research findings and individual case reports.[3] Studies on the internal and external anatomy of teeth have shown that anatomic variations can occur in all groups of teeth and can be extremely complex.[4]
Several authors have studied the morphology of root canals of mandibular incisors and the results are very divergent in relation to the anatomic characteristics.[5] Variation in root canal anatomy such as presence of extra canal, multiple foramina, apical delta, furcation, accessory canals etc. are common findings leading to apical percolation.[6] Thus, failure in root canal preparation of mandibular incisor occurs mostly because dentists miss the presence of second and/or lateral canals[2]. It is generally accepted that many mandibular incisors have two canals which may merge into one canal before reaching the apex.[7],[8],[9] Numerous studies have shown the mandibular incisors to have a single root with one or two root canals, mainly Type I and Type III canal configurations. [4],[5],[6],[7],[8],[9],[10]
The objective of the present case study is to record the occurrence of a two rooted mandibular central incisor demonstrated by radiovisiography and computed tomography (CT) examination.
Case Report
A 63-year-old male patient reported to the dental office with a complaint of severe pain in the right mandibular central incisor which was unprovoked and severe on biting. The dental history revealed prior root canal therapy in the tooth about a week ago. On examination, it was found that the patient had undergone a full- mouth rehabilitation procedure in which most of the teeth were root canal treated followed by placement of porcelain fused to metal crowns.
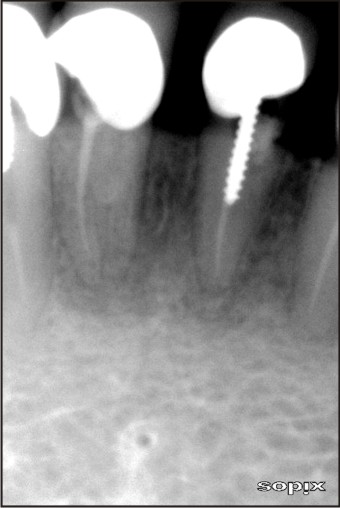
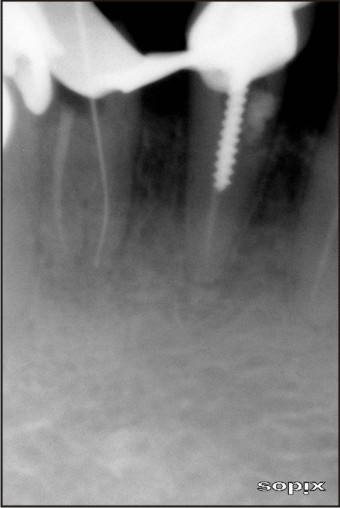
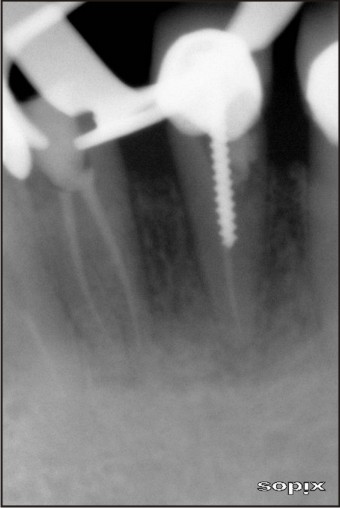
The clinical examination of the mandibular right central incisor revealed severe pain on percussion. The gingival was apparently normal, not sensitive to palpation, with no evidence of a swelling. The digital radiograph showed the tooth to be adequately obturated with the evidence of a mesial shadow. A second root placed lingually was revealed on a tube-shift radiograph (Fig.1) which was later confirmed by a CT scan of the mandible (Fig.2). The PFM crown was removed and after placement of a rubber dam, the access cavity was modified to envision the orifice of the second uninstrumented root. The working length was determined and confirmed radiographically (Fig.3). The canal was prepared using Protaper rotary instruments (Maillefer, Dentsply, Asia) till size F1, using EDTA as a lubricant and was copiously irrigated with 5.25% sodium hypochlorite after every file (Fig.4). Calcium hydroxide mixed with 2% Chlorhexidine was placed in the canal as an intracanal medicament for two weeks and analgesics were prescribed. The patient on recall was found to be asymptomatic, the root canal was obturated with gutta percha (Fig.5). A Resin-modified zinc oxide eugenol temporary restoration was placed and permanent restoration was advised. Post-operative radiographs revealed the presence of two separate obturated roots (Fig.6). Light cured composite resin as a permanent restoration, followed by placement of porcelain fused to metal crown.
 | Fig 1
 |
 | Fig 2
|
 | Fig 3
|
 | Fig 4
|
 | Fig 5
|
 | Fig 6
|
Discussion
The present case report illustrates a rare case of mandibular central incisor with two separate roots. Emilio C. Sponchiado and associates have reported that there are no limits for the morphological variability of the root canal.[1] Finding more than one root in the mandibular central incisor is rare. Louis I. Grossman, S. oliet reported that, the mandibular central incisor presents with one root which is flat and narrow mesiodistally but wide labiolingually.[11] The main reason for the unfavourable outcome in endodontic treatment of mandibular incisors is the inability to detect the presence of a second canal, which will not be disinfected and obturated during treatment.[12] This was true in the case of the presented report in which a separate root was present and was missed during treatment. It is essential that clinicians know the clinical and radiographic signs that suggest the presence of extra canals/roots. As per literature and studies conducted in different populations of the world by different authors regarding the morphology of mandibular incisors, it has been found that, mandibular central incisor generally presents only one root and one canal, but prevalence of one root with two canals is also seen. The prevalence of two-rooted mandibular central incisor has not been reported yet as such.[2],[3],[4]
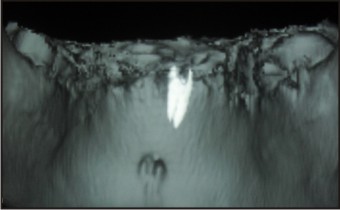
Careful interpretation of the radiographic features is essential in order that root canals are not overlooked. This depends on the availability of good and accurate radiographs and, ideally periapical radiographs taken from at least two different horizontal angles.[13] In the presented case, a second canal was suspected as the symptoms suggested it. But, radiographs exposed with a mesial shift of the X-ray tube head showed the presence of a separate lingual root. A CT scan of the mandible was performed to gain clear evidence of two separate roots as the presence of mesial or distal longitudinal grooves in the roots of mandibular incisors can lead to root canal bifurcations.[5] Computed tomography revealed the presence of a separate lingual root on the transverse sections (Fig.7) and also in the 3-D reconstruction of the tooth (Fig.8). It has been noted that CT provides accurate positioning, that is non-invasive, reproducible, high resolution and the reconstructed images based on CT image reliably represent the original structure.[14] As a powerful diagnostic tool, computed tomography has overcome the disadvantages of conventional radiography, and has attracted a great amount of attention in endodontic therapy. [15] The canal of the missed root was obturated in the second visit after the placement of the intracanal medicament to significantly reduce or eliminate micro-organisms if any, as the mixture of calcium hydroxide and 2% chlorhexidine has been proven to be very effective.[16]
 | Fig 7
|
 | Fig 8
|
This case report presents us with yet another example of the anomalous nature of mandibular lower central incisors. It helps us realize that knowledge of the internal anatomy is paramount to good endodontic practice. This case report also highlights the importance of multiple radiographs and the use of computed tomography as an adjunct in identifying abnormal tooth anatomy.
References
1. Emilio Carlos Sponchiado, Hanan Awwad Abdel Qader Ismail, Marcia Raquel lima Braga, Fabricio Kitazono de Carvalho, Claudia Andrea Correa Garcia Simoes. Maxillary central incisor with two root canals: a case report. J Endod 2006;32:1002-4.
2. Sinziana Scarlatescu, Andreea Cristiana Didilescu, Stefan-loan Stratul, Darian Rusu, Mihaela Grigore, Maria Greabu, Andrei lliescu. Root canal morphology of mandibular central incisors in south-eastern Romanian population: Endodontic and periodontal implications. Timisoara Med J 2010;60:280-3.
3. A. A. Al-Qudah, L. A. Awawdeh. Root canal morphology of mandibular incisors in a Jordanian population. Int Endod J 2006;39:873-7.
4. Lalit C Boruah, Atul C Bhuyan. Morphological characteristics of root canal of mandibular incisors in North-East Indian population: an in vitro study. J Con Dent 2011;14:346-50.
5. Simone Helena Gonsalves de Oliveira, Luiz cesar de Moraes, Horacio Faig-Leite, Samira Esteves Afonso Camargo, Carlos Henrique Ribeiro Camargo. In vitro incidence of root canal bifurcation in mandibular incisors by radiovisiography. J Appl Oral Sci 2009;17:234-9.
6. Ingle JI. Endodontics 2nd edn. Philedelphia; Lea and Febiger 1965;771-2.
7. Young hee Hwang, Kyung san Min. Clinical management of 3 mandibular incisors with 2 separate root canals and foramina: case report. J Can Dent Assoc 2005;71:388-9.
8. Vertucci FJ. Root canal anatomy of mandibular anterior teeth. J Am Dent Assoc 1974;89:369-71.
9. Bellizzi R, Hartwell G. Clinical investigation of in vivo endodontically treated mandibular anterior teeth. J Endod 1983;9:246-8.
10. Mauger MJ, Schindler WG, Walker WA. An evaluation of canal morphology at different levels of root resection in mandibular incisors. J Endod 1998;24:607-9.
11. Louis I. Grossman, Seymour oliet, Carlos E. Del Rio. Endodontic Practice. 11th edn. Philedelphia; Lea and Febiger 1988;165.
12. Katral N, Yanikoglu FC. Root canal morphology of mandibular incisors. J Endod 1992;18:562-4.
13. Yuri S. Kabak, Paul V. Abbott. Endodontic treatment of mandibular incisors with two root canals: report of two cases. Aust Endod J 2007;33:27-31.
14. Jin Zhao, Yan Li, Zhi-wei Yang, Wei Wang, Yan Meng. Three-dimensional computed topography analysis of a patient with an unusual anatomy of the maxillary second and third molars. Int J Oral Sci 2011;3:225-8.
15. Ballal S, Sachdeva GS, Kandaswamy D. endodontic management of a fused mandibular second molar and paramolar with the aid of spiral computed tomography: a case report. J Endod 2007;33:1247-51.
16. Reduction in cultivable bacterial population in infected root canals by chlorhexidine- based antimicrobial protocol. J Endod 2007;33 (5): 541-7
|