Introduction:
Dental plaque is considered to be the single most important easily demonstrable local etiological factor playing a significant role in the initiation and progression of periodontal disease.[1] There is a high correlation between poor oral hygiene, the presence of plaque and the prevalence and severity of gingival and periodontal diseases.
The pathological potential of plaque is attributed to its ability to concentrate large populations of microorganisms in proximity to gingival tissues that initiates an inflammatory process in the supporting structures of the teeth.[2] Loe et al (1965), in their study, clearly demonstrated that gingival inflammation consistently follows the build-up of plaque, and that conversely, removal of plaque can reverse this process.[3], [4], [5], [6] The 1998 European Workshop on Mechanical Plaque Control emphasized it by concluding, “Forty years of experimental research, clinical trials and demonstration projects in different geographical and social settings have confirmed that effective removal of dental plaque is essential to dental and periodontal health throughout life”.[7]
To achieve this goal, mechanical removal of plaque is the most reliable, dependable and common method of controlling and preventing the accumulation of bacterial plaque and other deposits.[6],[8],[9],[10],[11] Amongst the mechanical methods, a toothbrush is undisputedly the most efficient and widely used oral hygiene measure.[6],[11],[12]
Toothbrushes can be classified as manual and powered. Powered toothbrushes offer an alternative to manual toothbrushes.[13],[14] For the electric toothbrushes, the individual only guides the head of the toothbrush around the dentition, the mechanical cleaning action being provided electrically. The advantages of electric toothbrush lay in the fact that they require minimum skill in handling by the patient and that the head has a constant and autonomous movement, independent of brushing technique used.[15],[16]
The addition of low frequency acoustic energy generates dynamic fluid movements and provides cleaning slightly away from the bristle tips.[13] The vibrations have been shown to interfere with bacterial adherence to oral surfaces.[17], [18], [19] Hydrodynamic shear forces created by these brushes disrupt plaque a short distance from the bristle tips, providing additional interproximal plaque removal.[20] According to Hope CK and Wilson M in 2003, the fluid shear forces induced by the activated toothbrush are of sufficient magnitude to remove oral biofilms from a distance of at least 2.65 mm from the bristles.[21] Swedish watchmaker Fredrick Wilhelm Tornberg is credited with designing the first mechanical toothbrush in 1885, but it was reliably sold in 1939 (in Switzerland). Broxodent, was a rotating electric toothbrush introduced by Squibb Pharmaceutical at the centennial of the American Dental Association in 1960.[22], [23], [24]
In recent years, a range of new electric toothbrushes with varying characteristics, design and arrangement of bristles, head or filament motion (reciprocating, arcuate, orbital, vibratory, elliptical or dual) and speed (may vary from 1000 strokes/minute to 31,000 strokes per minute) are being introduced in the market in an attempt to achieve optimal tooth cleanliness. The purpose of the present study was to evaluate the efficacy of two commercially available powered toothbrushes in plaque control.
Materials And Method:
For the present study, 20 subjects (10 males and 10 females) having normal occlusion and in the age group of 18-25 years were selected amongst the students of Dental College living under similar environment and dietary conditions in the hostels to avoid intra-sample variation. Subjects were explained the study design and a written informed consent was obtained from each of them
Selection criteria included: 1) a full complement of teeth (excluding 3rd molars), 2) no caries or restoration on the tooth surfaces, 3) normal occlusion with good gingival and periodontal health, 4) a good general health without any systemic disease.
Materials used: Colgate Strong Teeth toothpaste, Colgate Motion powered toothbrush and Oral-B Cross Action Power powered toothbrush (Figure-1).
 | Figure 1 : Showing The Head Designs Of The Two Brushes
 |
The specifications of the brushes are:
Colgate Motion Powered Toothbrush (CM PTB): Working at a frequency of 2120 rpm; Having 10 degrees inclination of shank and handle; Oval shaped working head (22.3 mm long, and 8 mm wide at the tip and 13.4 mm wide at the centre); It has a dual action head i.e. an upper small circular head- rotating anti-clockwise with 8 tufts of soft bristles (10.85 mm long and 0.18 mm diameter) and a lower large circular head- rotating clockwise with 23 tufts of soft bristles (8.35 mm long and 0.18 mm diameter) arranged in 2 concentric rows.
Oral-B Cross Action Power Powered Toothbrush (OB PTB): Working at a frequency of 2225 rpm; Having 3 degrees inclination of shank and handle; Rectangular working head (25.5 mm long and 14.2 mm wide); It has a dual action head i.e. an upper circular head- rotating clockwise having 22 tufts of soft bristles (5.95 mm long and 0.15 mm diameter) arranged in 3 concentric rows and a lower head- having vibratory motion with 14 tufts of soft bristles (8.64 mm long and 0.19 mm diameter) arranged in criss-cross manner.
Method:
The study was divided into 2 phases - each phase of 4 weeks duration with a washout period of 15 days in between the two phases: In phase I, all subjects used “Colgate Motion Powered Toothbrush” and in phase II, all subjects used “Oral-B Cross Action Powered Toothbrush”.
At the start of each phase, thorough dental prophylaxis of all the subjects was carried out to bring the plaque scores to zero. All the subjects were advised to brush their teeth twice a day i.e. immediately after breakfast and after dinner for 2 minutes with the toothbrush assigned for that phase. After 4 weeks, the subjects discontinued using the powered toothbrush and proceeded with their manual toothbrush that they used before the study for the next 15 days. This wash out period was introduced to discontinue the familiarization of the subjects with the first powered toothbrush before they used the next powered toothbrush. After 15 days, again a thorough prophylaxis of all the subjects was done to make them plaque free and the second toothbrush was assigned to the subjects for the next phase.
Following instructions were given to each participant;
1) participants were asked to squeeze out 2.5 cm ribbon of the supplied tooth paste on the head of the toothbrush provided, 2) to use only the toothbrush and the tooth paste provided, 3) not to use any mouthwash during the course of the study, 4) not to take any antibiotics and other drugs during the study.
Plaque Recording: In each phase, plaque scores were recorded after the completion of the first week and fourth week with the help of disclosing solution (0.075% Basic Fuchsin), using Turesky, Gillmore and Glickman plaque index which is the modification of Quigley, Hein and Elliot plaque index.[25] Each subject was given 15 ml of above solution and asked to swish that slowly in the mouth for 20 seconds. This was followed by two rinses with plain water and recording of the scores was done. The recorded data of plaque score was put to statistical analysis and the results obtained were compiled.
Results:
The recorded parameters were subjected to student paired t-test and results were compiled. A paired t-test is used to compare two population means where you have two samples in which observations in one sample can be paired with observations in the other sample. Examples of where this might occur are:
• Before-and-after observations on the same subjects (e.g. students’ diagnostic test results before and after a particular module or course).
• A comparison of two different methods of measurement or two different treatments where the measurements/treatments are applied to the same subjects (e.g. blood pressure measurements using a stethoscope and a dynamap).
The results of the study are presented in Tables 1-3 and Figures 2-3. Table-1 shows the mean plaque scores of all individuals at different recording periods in phase-I and phase-II.
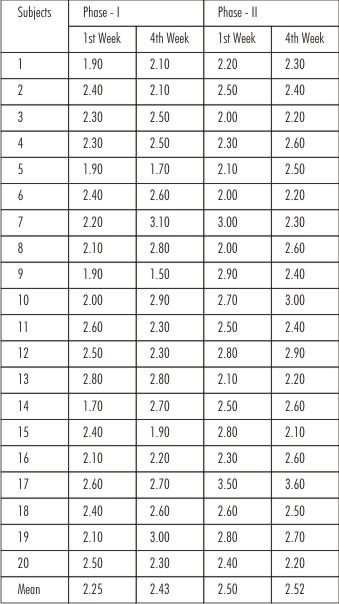 | Table 1 : Mean Plaque Scores At Various Recording Periods In Phase-I and Phase-II
|
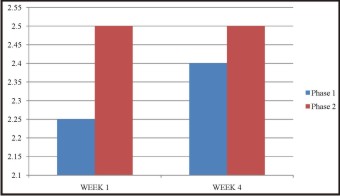 | Figure 2 : Showing The Comparison Of The Mean Plaque Scores Of Phase – I And Phase - II At The End Of 1st And 4th Week
|
 | Table 2 : Significance Of Difference Between The Mean Plaque Scores In Phase - I And Phase - II
|
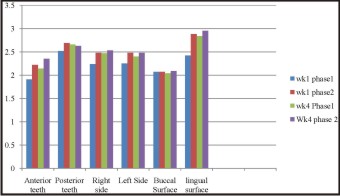 | Figure 3 : Showing The Comparison Of The Mean Plaque Scores Of Different Areas In Phase - I and Phase - II At The End Of 1st And 4th Week
|
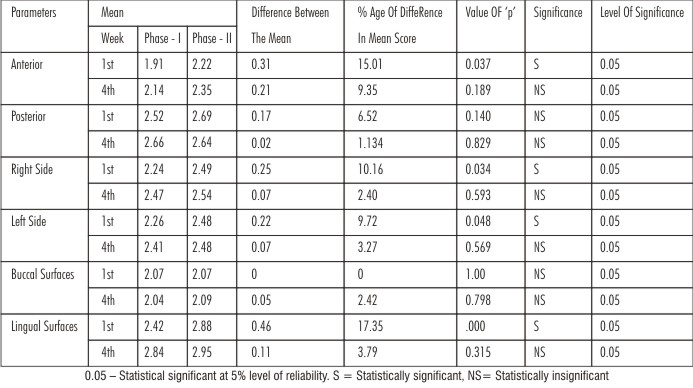 | Table 3 : Significance Of Difference Between The Mean Plaque Scores Of Different Areas In Phase - I And Phase - II
|
Mean Plaque Scores: The differences between the mean plaque scores of phase-I and phase-II after 1st week and 4th week are shown in Table-2 and Figure-2. This difference after 1st week was 0.25 which was found to be statistically significant at 5% level of significance. However, at the end of 4th week, the difference was 0.08 which was statistically insignificant.
Increment in mean plaque score: The increment in mean plaque score after 1st week in phase-I was 2.25 and after 4th week was 0.18, and the increment in mean plaque score in phase-II after 1st week was 2.50, and after the 4th week was 0.02. Table-3 and Figure-3 show the comparison of the mean plaque scores of different areas i.e. anterior teeth, posterior teeth, right side, left side, buccal and lingual surfaces in phase-I and phase-II at the end of 1st and 4th week.
Anterior Teeth: The difference between the mean plaque scores of anterior teeth between phase-I and phase-II after 1st week was 0.31 which was found to be statistically significant at 5% level of significance. However, this difference was 0.21 after the 4th week which was statistically insignificant.
Posterior Teeth: When the difference between the mean plaque scores of posterior teeth in phase-I and phase-II was compared in relation to each other by applying the t-test, the difference after 1st week was 0.17 and after 4th week was 0.02 which was statistically insignificant.
Right Side: At the end of 1st week the difference between the mean plaque scores of right side in phase-I and phase-II was 0.25 which was found to be statistically significant whereas the difference between them after 4th week was 0.07 that was statistically insignificant at 5% level of significance.
Left Side: The difference between the mean plaque scores of left side in both the phases, when put to statistical analysis, came out to be 0.22 at the end of 1st week which was statistically significant (i.e. p<0.05) whereas the difference after 4th week was 0.07 which was not statistically significant
Buccal Surfaces: The difference between the phases after 1st week was 0.0 and after 4th week was 0.05 which were statistically insignificant at 5% level of significance.
Lingual Surfaces: The difference in mean plaque scores between both the phases at the end of 1st week was 0.46 which was found to be statistically significant (i.e. p<0.05) whereas it was 0.11 after 4th week which was found to be statistically insignificant.
Discussion
Periodontal disease, in its various forms has afflicted mankind since the dawn of history. It is widely acknowledged that plaque accumulation is an important factor in the initiation and progression of gingival and periodontal disease.[1] This suggests that maintenance of an effective plaque control is the cornerstone of any attempt to prevent or control periodontal diseases. In an attempt to assist individuals in removing dental plaque, a variety of electric toothbrushes have been produced.[9]
The two powered toothbrushes used in the study were- Colgate Motion Powered Toothbrush (CM PTB) and Oral-B Cross Action Powered Toothbrush (OB PTB). The results of the study showed that CM PTB demonstrated significantly greater plaque reduction in mean plaque scores as compared to the OB PTB at the end of 1st week. This could be due to narrow and oval shaped working head of CM PTB that it could easily be worked over the anterior as well as posterior teeth, as compared to the rectangular head of OB PTB that might have made it more bulky and a bit difficult to operate. Also, the bristles in the upper head of Colgate Motion were slightly thicker and harder than that of the Oral-B that helped in better plaque removal in the 1st phase. Subjects in both the phases showed slightly higher plaque scores at week 4, thus suggesting a ‘rebound’ effect during this period of unsupervised oral hygiene. This finding confirms to the findings of Baab DA et al (1989) who conducted their study over a period of 4 weeks and reported similar results.[22]
When the relative effectiveness of toothbrushes in plaque control was compared, it was observed that the variation in the shape of the working head when studied for a period of one week was found to be statistically significant. One possible explanation of this finding might be due to fact that patients were very conscious about their oral hygiene in the period immediately following their oral prophylaxis, but with the course of time the patients might got lenient in maintaining proper oral hygiene and might showed less compliance at subsequent visits.[26],[27]
The maximum increment in the mean plaque score was noted at 1st visit after prophylaxis in each phase. This may be due to the fact that plaque first accumulated in those areas which are not accessible to the friction of mastication or are relatively inaccessible to the action of toothbrushing. In subsequent weeks most of the plaque formed on the accessible areas is removed with the action of toothbrush, resulting in stabilization or decrease in increments in mean plaque score.
It is usually seen that the subjects are more conscious in cleaning their anterior teeth as they are visible during talking and smiling, and neglect or give less importance to their posterior teeth. Rugg-Gunn and MacGregor (1978), and MacGregor and Rugg-Gunn (1979) supported this finding by suggesting that certain tooth sites appear to receive little attention during the brushing cycle and such sites include posterior teeth and palatal/lingual surfaces.[28], [29], [30] CM PTB had statistically significant greater plaque reduction as compared to OB PTB at the end of 1st week. However, this difference was not statistically significant when the means of the posterior teeth of the two phases were compared at any time period of the study. This can be explained as posterior teeth have less accessibility to both the toothbrushes owing to less vestibular depth in the posterior region.[30]
Generally, the facial/buccal surfaces are given more focus while toothbrushing than the palatal and lingual surfaces. This may be due to fact that lingual and palatal surfaces are often difficult to reach with a toothbrush. Similar results were observed by Rugg-Gunn and MacGregor (1978), and MacGregor and Rugg-Gunn (1979) who demonstrated that at least 90% of brushing time is spent on the buccal surfaces whereas a maximum of 10% of brushing time was allocated to the lingual.[28],[29],[31] On the buccal surfaces, no significant effect of the brush head design on plaque removal was observed by either of the brushes at any time period. However, Colgate Motion showed significantly better results in lingual areas at the end of 1st week which can be attributed to the inclination between shank and handle i.e.10 degrees (as compared to a 3 degrees inclination of that of OB PTB) that allowed better adaptation of the brush head on the lingual surface.
Neither of the comparisons made between right and left side, being cleaned by the same toothbrush, at any time point came out to be statistically significant indicating that the efficacy of the powered toothbrushes is independent of the right- or left-handedness of the patient. However, plaque removal by CM PTB as compared to OB PTB was found to be statistically significant in both the left and right sides at the end of 1st week but no significant differences were found at the end of 4th week.
Although toothbrushing has become the most widely practiced method of individual mechanical plaque removal, a paucity of conclusive research exists on the optimal design of toothbrushes and bristles. Therefore, testing of new prototype toothbrushes should be structured.
Conclusion
In the present study, it was found that plaque removal by CM PTB exhibited improved plaque removal than OB PTB in many areas of the oral cavity in both the time periods but the results were statistically significant only at the end of 1st week. Therefore, it is concluded that within usual variations, the shape of the working head by itself has, but, limited influence on the cleaning efficiency of the toothbrush.
References
1. Zimmer S, Didner B, Roulet J-F. Clinical study on the plaque removal ability of a new triple-headed toothbrush. J Clin Periodontol 1999;26:281-5.
2. Glickman I. Dental plaque, acquired pellicle, materia alba, food debris, dental calculus and dental stains. In: Glickman I, editor. Clinical Periodontology: Prevention, Diagnosis and Treatment of Periodontal Disease in the Practice of General Dentistry. University of Michigan: Saunders; 1972. p. 291-314.
3. Loe H, Theilade E, Jenson SB. Experimental gingivitis in man. J Periodontol 1965;34:177-87.
4. Bogren A, Teles RP, Torresyap G, Haffajee AD, Socransky SS. Clinical and microbiologic changes associated with the combined use of a powered toothbrush and a triclosan/copolymer dentifrice: A 3-year prospective study. J Periodontol 2007;78:1708-17.
5. Horiuchi M, Yamamoto T, Tomofugi T, Ishikawa A, Morita A, Watanabe T. Toothbrushing promotes gingival fibroblast proliferation more effectively than removal of dental plaque. J Clin Periodontol 2002;29:791-5.
6. Shibly O, Schifferle RE, Ciancio SG, Tarakji M, Mather ML. A clinical comparison of 2 electric toothbrush designs. J Clin Periodontol 1997;24:260-3.
7. Perry DA. Plaque control for the periodontal patient. In: Carranza FA, David L, Giannobile WV, Kenney EB, Novak MJ, editors. Carranza’s Clinical Periodontology. St. Louis(MO): Saunders Elsevier; 2006. p. 728-48.
8. Lazarescu D, Boccaneala S, Illiescu A, De Boever JA. Efficacy of plaque removal and learning effect of a powered and a manual toothbrush. J Clin Periodontol 2003;30:726-31.
9. Johnson BD, McInnes C. Clinical evaluation of the efficacy and safety of a new sonic toothbrush. J Periodontol 1994;65:692-7.
10. McCracken GI, Janssen J, Swan M, Steen N, de Jager M, Heasman PA. Effect of brushing force and time on plaque removal using a powered toothbrush. J Clin Periodontol 2003;30:409-13.
11. van der Weijden GA, Hioe KPK. A systematic review of the effectiveness of self-performed mechanical plaque removal in adults with gingivitis using a manual toothbrush. J Clin Periodontol 2005;32 Suppl 6:S214-28.
12. Checchi L, Farina E, Felice P, Montevecchi M. Electric toothbrush analysis of filaments under stereomicroscope. J Clin Periodontol 2004;31:639-42.
13. Forgas-Brockmann LB, Carter-Hanson C, Killoy WJ. The effects of an ultrasonic toothbrush on plaque accumulation and gingival inflammation. J Clin Periodontol 1998;25:375-9.
14. Echeverria JJ, Sanz M. Mechanical supragingival plaque control. In: Lindhe J, Karring T, Lang NP, editors. Clinical Periodontology and Implant Dentistry. United Kingdom: Blackwell Munksgaard; 2003. p. 449-63.
15. Driesen GM, Warren PR and Hilfinger P. Cleaning efficacy of a new electric toothbrush. Am J Dent 1998;11:S7-S11.
16. Warren PR and Chater B. The role of electric toothbrush in the control of plaque and gingivitis: a review of 5 years clinical experience with the Braun Oral-B Plaque Remover (D7). Am J Dent 1996;9:S5-S12.
17. McInnes C, Engel D and Martin RW. Fimbria damage and removal of adherent bacteria after exposure to acoustic energy. Oral Microbiol Immunol 1993;8:277-82.
18. Wu-Yuan CD, Anderson RD and McInnes C. Ability of the Sonicare electric toothbrush to generate dynamic fluid activity that removes bacteria. J Clin Dent 1994;5;89-93.
19. Heasman PA, McCraken GI. Powered toothbrushes: a review of clinical trials. J Clin Periodontol 1999;26:407-20.
20. Hope CK, Petrie A, Wilson M. In vitro assessment of the plaque-removing ability of hydrodynamic shear forces produces beyond the bristles by 2 electric toothbrushes. J Periodontol 2003;1017-22.
21. Hope CK, Wilson M. Effects of dynamic fluid activity from an electric toothbrush on in vitro oral biofilms. J Clin Periodontol 2003;30:624-9.
22. Baab DA and Johnson RH. The effect of a new electric toothbrush on supragingival plaque and gingivitis. J Periodontol 1989;60:336-41.
23. Ainamo J, Xie Q, Ainamo A, Kallio P. Assessment of the effect of an oscillating/rotating electric toothbrush on oral health. A 12-month longitudinal study. J Clin Periodontol 1997;24:28-33.
24. Sicilia A, Arregui I, Gallego M, Cabezas B, Cuesta S. A systematic review of powered versus manual toothbrushes in periodontal cause-related therapy. J Clin Periodontol 2002;29 Suppl.3:S39-54.
25. Turesky S, Gilmore ND and Glickman I. Reduced plaque formation by the chloromethyl analogue of vitamin C. J Periodontol 1970;41:41-3.
26. Robertson PB, Armitage GA, Buchanan SA and Taggert EJ. The design of trials to test the efficacy of plaque control agents for periodontal diseases in humans. J Dent Res 1989;68:1667-71.
27. McCracken GI, Heasman L, Stacey F, Steen N, de Jager M and Heasman PA. Testing the efficacy of 2 prototype brush heads for a powered toothbrush: refining the model. J Clin Periodontol 2002;29:42-7.
28. Rugg-Gunn AJ & MacGregor IDM. A survey of toothbrushing behaviour in children and young adults. J Periodont Res 1978;13:382-8.
29. MacGregor IDM, Rugg-Gunn AJ. A survey of toothbrushing sequence in children and young adults. J Periodont Res 1979;14:225-30.
30. Addy M, Renton-Harper P, Warren P, Newcombe RG. An evaluation of video instruction for an electric toothbrush: comparative single brushing cross-over study. J Clin Periodontol 1999; 26:289-93.
31. Claydon N, Moran J, Newcombe RG, Smith SR, Addy M. Clinical development and evolution in plaque removal performance of a battery powered toothbrush. J Clin Periodontol 2004;31:835-9.
|