|
|
|
| Formocresol Pulpotomy: Saviour Of Primary Tooth |
Kirtaniya BC 1 , Gupta KK 2 , Gaur A 3 , Sharma A 4
1 Professor And Hod, Department Of Pedodontics - Himachal Dental College, Sundernagar.
2 Reader, Department Of Pedodontics - Himachal Dental College, Sundernagar
3 Senior Lecturer, Department Of Pedodontics - Himachal Dental College, Sundernagar
4 Postgraduate Student, Department Of Pedodontics - Himachal Dental College, Sundernagar
|
| Address For Correspondence |
Dr. Kirtaniya B.C., Professor and HOD,
Department of Pedodontics,
Himachal Dental College, Sundernagar,
District-Mandi, Himachal Pradesh, India
Mobile: +919816408557
e-mail: drbimalchandra@gmail.com |
| Abstract |
| The pulp therapy in primary teeth in the form of pulpotomy is a simple and effective procedure. Over the years, various medicaments have been tried and used for pulpotomy in primary teeth but formocresol still remains a popular medicament for this technique in these teeth. There are some advantages and disadvantages of this material and if used judiciously, the advantages are more and no disadvantage is found so far success rate is concerned. In this article we try to explain the use of formocresol as a pulpotomy agent in primary teeth. |
|
| Keywords |
| Formocresol, Pulpotomy, Primary Tooth, Calcium Hydroxide |
|
| Full Text |
Introduction
Restoration of the damaged primary tooth is an important part of paediatric dentistry. It becomes more challenging when the pulp is involved. The most common cause for pulpal exposure is caries followed by trauma and it may so happen during cavity preparation. The spread of infection and inflammation after pulpal exposure may be throughout the pulp cavity for which pulpectomy is the treatment of choice. When the infection and inflammation is limited to the coronal pulp as indicated through clinical and radiographic evaluation, pulpotomy should be performed in all circumstances.
Pulpotomy can be defined as the surgical removal of the infected and inflamed coronal pulp followed by placement of a suitable medicament over the radicular pulp that promotes healing and preserves the vitality and function of the tooth. The American Academy of Paediatric Dentistry defines it as a procedure involving amputation of the coronal portion of the affected or infected dental pulp.[1] Treatment of the remaining radicular pulp tissue should preserve the vitality and function of all or part of the remaining radicular portion of the pulp. The coronal pulp chamber is filled and the tooth is restored with a stainless steel crown.
Indications For Pulpotomy
1) Carious exposed primary tooth provided the infection and inflammation is limited to the coronal pulp tissue.
2) A large traumatic exposure of the pulp of primary tooth and the patient reports to the dentist immediately or within 24 hours.
3) A smaller traumatic exposure of the pulp of primary tooth and the patient reports to the dentist after 24 hours but before 72 hours.
4) Pulpotomy in primary tooth can be done as an emergency and intermediate procedure where there is an irreversible pulpitis which is then followed by pulpectomy and RCT.
5) In case of pin point traumatic pulp exposure (or even non exposure of the pulp), intentional pulpotomy is done where crown is insufficient to hold a temporary restoration.
6) A large mechanical exposure of pulp while cavity preparation, pulpotomy is indicated.
7) A haemophilic child or children suffering from other bleeding disorders where extraction is to be avoided[2].
8) A diabetic child where general anaesthesia has to be avoided
9) Patient compliance – previous unhappy experience of tooth extraction; the patient here finds pulp treatment more preferable and less stressful.
10) Dentition in which there is shortage of space, tooth loss here will further lead to crowding.
Contraindications
1) There should not be spontaneous pain or persistent pain or pain at night.
2) The tooth should not be tender on percussion.
3) There should not be excessive bleeding while performing pulpotomy.
4) There should not be internal resorption or pathological external root resorption
5) There should not be any exudates or pus at the exposure site or within the pulp chamber.
6) There should not be interradicular or periapical radiolucency
7) There should not be excessive calcifications of the root canals or the pulp chambers.
8) Excessive tooth mobility should not be there.
9) Children with rheumatic heart disease, bacterial endocarditis or congenital heart disease where there are chances of transient bacteraemia should avoid such treatment.
10) Children with hypogammaglobulinemia or suffering from cancers or transplant recipients are contra-indicated for such treatment.
11) Caries penetrating the floor of the pulp chamber or a grossly decayed tooth which is not restorable.
12) A tooth close to natural exfoliation (i.e. with less than 2/3rd of root length remaining.)
Procedure
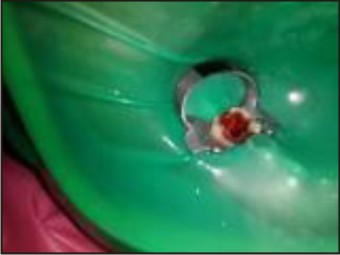
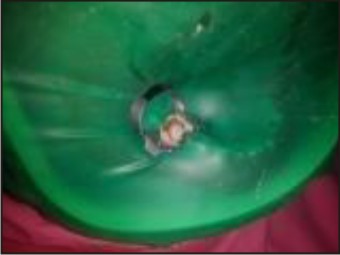
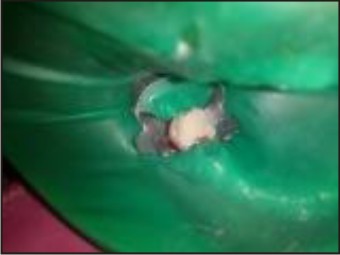
Localanaesthesia is administered and the tooth is isolated with rubber dam (Fig1). All the caries and unsupported enamel is removed from the tooth. With a round bur the access opening is made and the roof of the pulp chamber is removed with a fissure bur. It is to remember that plugging the pulp tissue with the bur is to be avoided while access cavity preparation or its extension. Now, with a sharp sterile spoon excavator the coronal pulp tissue is extirpated (Fig 2). We do not recommend round bur to be used for removal of coronal pulp tissue because the floor of pulp chamber of primary tooth is thin and porous. Bleeding is arrested with pressure packs. With a cotton pellet, 1:5 dilution of formocresol is applied over the amputed radicular pulp for 5 minutes after excess formocresol is wiped out from the cotton pellet on a blotting paper (Fig 3).
 | Fig 1 : Pre Operative
 |
 | Fig 2 : Pulp Removed With Spoon Excavator
|
 | Fig 3 : Formocresol Applied
|
Recent studies have shown that 1 minute application of the same dilution is equally effective and successful. The cotton pellet is removed and the pulp chamber is dried with a fresh cotton pellet. The pulp chamber is filled partially with ZOE cement and the tooth is filled with GIC followed by restored with a stainless steel crown (Fig 4 and 5).
 | Fig 4 : GIC Filling
|
 | Fig 5 : Stainless Steel Crown
|
In the two visits pulpotomy technique, the cotton pellet is left in contact with the pulp tissue for 3-5 days with a temporary filling material like ZOE or cavit. After 3-5 days the tooth is reopened and the cotton pellet is removed. The pulp chamber is partially filled with ZOE cement and the tooth is restored with a silver amalgam restoration followed by a stainless steel crown. This technique is still very much useful when there is sluggish bleeding persist after amputation of the coronal pulp tissue and the surgeon feels that the inflammation is beyond coronal pulp. The indications of two visits pulpotomy are:
1) Sluggish or profuse bleeding from the amputated pulp stumps.
2) Bleeding is difficult to control.
3) Slight purulence in the pulp chamber.
4) Thickened periodontal ligaments.
5) It is also indicated where short appointment is necessary e.g. un-cooperative patients.
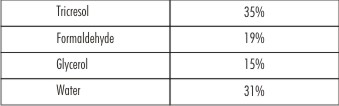
Composition Of Formocresol
Despite some drawbacks, formocresol continues to be the most commonly used medicament in the treatment of primary teeth pulpotomy. The composition[5] of formocresol is as follows:
 |
|
The above composition is popularly known as Buckley’s solution and the recommended dilution is 1:5 in distilled water.
Milestone Studies
Formocresol was introduced in dentistry by Buckley who treated “putrescent “and necrotic pulp with this solution during 1904 to 1906. Thereafter, it was used as a root canal disinfectant and Sweet[6] in 1930s advocated a 5 visit pulpotomy with this solution. He performed 16,651 pulpotomy with formocresol from 1930 to 1955 and found a success rate of 97%. Doyle[8] in 1962 advocated a 2 visit pulpotomy and Spedding[9] in 1965 advocated a single visit 5 minute application of formocresol in pulpotomy of primary teeth. Straffon and Han[11] (1968, 1970) concluded that formocresol at 1:5 strength might be equally effective and possibly less damaging pulpotomy agent. Garcia - Godoy[13] in 1980’s advocated a 1:5 dilution of formocresol for 1 minute application in pulpotomy in dogs. However, further studies are needed for verification of its success of 1 minute application of formocresol in pulpotomy in primary teeth of humans.
The histological studies of the pulp tissue after formocresol application were first studied by Massler and Mansukhani[14] in 1959. The authors studied the effect of formocresol on pulp of 43 human primary and permanent teeth in detail. The treatment interval was 1-36 minutes application of formocresol and the duration of study was 1-3 years. They have found that there are three distinctive layers formed after the application of formocresol. These are
1) Immediately after application of formocresol, a broad eosinophilic zone of fixation is formed
2) Below, a broad pale staining zone with poor cellular definition and further below
3) A zone of inflammation diffusing apically into the normal pulp tissue.
After 60 days the remaining pulp tissue was believed to be completely fixed.
Other Studies
Formocresol has been in use for more than hundred years in dentistry and it is the most popular medicament for pulpotomy in primary teeth among paediatric dentists all over the world. Clinical and radiographic successes of formocresol pulpotomy in primary teeth were studied by various authors throughout the world. Doyle and McDonald (1962) compared formocresol pulpotomy technique with calcium hydroxide in primary canine and found that the formocresol technique to be 95% successful clinically at the end of 1 year. Law and Lewis[15], (1964) evaluated the clinical effectiveness of formocresol technique over 4-year period and reported a 93 to 98% success rate. Berger[17] (1965) compared one-appointment formocresol pulpotomy with ZOE pulpotomy in human primary molars which were cariously exposed. He found a success rate of 97% for formocresol group and 58% success rate for ZOE group both clinically and radiographically. Fuks[19] et al (1990) found an 18% failure rate after 25 months in pulpotomized primary molars with gluteraldehyde. They concluded that their results did not justify substituting gluteraldehyde for formocresol in primary tooth pulpotomy.
The advantages of formocresol for pulpotomy in primary teeth are:
1) It is germicidal
2) It does not induce internal root resorption of primary tooth
3) It is very much effective in primary teeth and the success rate is more than 90%
4) No untoward effects were observed to the developing permanent tooth buds.
5) It does not influence physiological root resorption of primary tooth ie neither it accelerates nor it causes delayed root resorption of primary tooth.
However, there are some drawbacks with this material too. These are:
1) Local toxicity: If it is accidentally applied on gingiva or mucosa or lips it causes ulcerations. It can be easily avoided if judiciously used.
2) It was found to be cytotoxic, mutagenic and carcinogenic. Formocresol was found to be carcinogenic in rodents. No human study was reported on this effect.
3) Systemic absorption: It was found in periodontal ligaments, bone, dentin and urine. Whether its systemic absorption is harmful or tolerable is still debatable.
4) Its antigenicity has also been reported.
Other Medicaments Used For Primary Teeth
To overcome some drawbacks of formocresol various agents were tried both in experimental animals and in human teeth. The other medicaments used for pulpotomy in primary teeth includes gluteraldehyde, ferric sulphate, freeze dried bone, MTA, and transforming growth factors (TGF). Gluteraldehyde has got superior fixation property by cross linkage. It causes less necrosis of pulp tissue as well as less dystrophic calcification. It is an excellent antibacterial agent. But Fuks et al (1990) did not recommend it as a substitute for formocresol. On the other hand, ferric sulphate forms a ferric ion-protein complex which occludes capillaries mechanically. It is less inflammatory than formocresol and it maintains the vitality of the tooth. This medicament seems to be promising for pulpotomy in primary teeth. Fuks and co-workers[20] in 1997 have found equal success rates with formocresol and ferric sulphate both in animals and in human studies.
Bone morphogenetic proteins have been proposed as a pulpotomy material in experimental animals. Bone morphogenetic proteins 2 to 8 belongs to transforming growth factor (TGF)-β, that are signalling proteins that regulate cell differentiation. Bone morphogenetic proteins 2 and 4 have been implicated in odontoblastic differentiation. Nakashima[21] (1994) demonstrated dentin bridging in dogs teeth after pulpotomy with BMP-2 and BMP-4 along with recombinant human dentin matrix.
Discussion
Often, some paediatric dentist and general dentist have tendency to extract a cariously involved primary tooth and place a space maintainer into the extracted space. In routine practice, space maintainers which are commonly used are band and loop, lingual arch or Nance palatal arch type. They do not help in mastication of food, speech and aesthetics. When the child is growing; he needs proper food and nutrition during the most active period of overall growth and development. Do these types of space maintainers provide him all the necessary things? Above all, we must not forget that a primary tooth is the best space maintainer for their successors. Therefore, we must save them through pulpotomy with formocresol, if indicated.
The premature loss of primary teeth due to dental caries and infection will result in 1) loss of arch length, 2) ectopic eruption of the permanent tooth, 3) insufficient space for eruption of permanent teeth which may cause impaction, 4) mesial migration and tipping of posterior teeth adjacent to primary molar loss, 5) midline shift, 6) extrusion of opposing permanent teeth 7) development of abnormal oral habits and 8) there may be development of localised hypoplasia. For these reasons maximum attempts must be made to preserve the primary teeth in a healthy state until normal exfoliation occurs. Moreover, an untreated carious primary tooth or traumatically affected primary tooth might cause enamel hypoplasia (Turner’s tooth) to the developing permanent tooth buds. A simple procedure of pulpotomy will help you to resolve all the above mentioned problems which might arise later on as a result of dental caries.
When the tooth is infected grossly and the infection and inflammation is wide spread, pulpectomy and RCT is the treatment of choice. But the technique requires skill, is more time consuming, need multiple appointment, patient’s cooperation and costly. However, in highly uncooperative patients it is the skill of the paediatric dentist which makes him perform the procedure or it can be performed under GA which is more costly. If not succeeded extraction of the tooth should be avoided and pulpotomy can be used as an alternative treatment.
Calcium hydroxide should not be used as a medicament in pulpotomy for primary tooth because it induces internal root resorption. The probable causes[22] may be that calcium hydroxide is alkaline and irritating in nature which might cause over stimulation of the radicular pulp tissue thereby formation of osteoclast or odontoclast type of cells that cause internal resorption. In the primary tooth, inflammation is wide spread and if some inflammatory tissue is left at the orifice of the root canals might attract osteoclasts. Moreover, primary teeth are in the process of physiological root resorption, osteoclastic activity might be further increased due to the irritating nature of calcium hydroxide and cause internal resorption. However, in a study of calcium hydroxide versus formocresol Waterhouse[23] et al, 2000 concluded that calcium hydroxide can be used as a pulpotomy agent for the treatment of primary teeth. We don’t recommend Calcium hydroxide as a pulpotomy agent in primary dentition because of above mentioned drawbacks.
References
1. American Academy of Pediatric Dentistry : Guideline on pulp therapy for primary and young permanent teeth. Reference manual 2002-2003 page 86-90
2. UK National Clinical Guidelines in Paediatric Dentistry. International Journal of Paediatric Dentistry.2000; 10:248-252
3. P.Carrotte. Endodontic treatment for children.BDJ.2005; 198:9-15
4. Camp J. Pedodontic-endodontic treatment: In : Cohen S, Burns R, eds Pathways of the Pulp.9th ed. St. Louis, Mo: Mosby Year Book.
5. Buckley JP. The chemistry of pulp decomposition with a rational treatment for this condition and its sequelae. J Am Dent Assoc 1904; 3:764.
6. Sweet CA: Procedure for treatment of exposed and pulpless deciduous teeth. J Am Dent Assoc 1930; 17:1150-53.umber 2
7. Sweet CA: Treatment of vital primary teeth with pulpal involvement. Therapeutic pulpotomy. J Colorado D A. 1955; 33: 10-4 (Quoted) Ranly DM: Pulpotomy therapy in primary teeth: new modalities for old rationales. Pediatr Dent 1994; 16: 403-9.
8. Doyle WA, McDonald RE, Mitchell DF: Formocresol versus calcium hydroxide in pulpotomy. ASDC J Dent Child.1962; 29: 86-97. (Quoted) Ranly DM: Pulpotomy therapy in primary teeth:
9. Spedding RH, Mitchell DF, McDonald RE. Formocresol and calcium hydroxide therapy. J Dent Res 1965; 44:1023.
10. Spedding RH. Formocresol pulpotomies for permanent teeth. In: Goldman HM, et al., editors. Current therapy in dentistry.Vol 5. St. Louis: CV Mosby; 1975
11. Straffon LH, Han SS. The effect of formocresol on hamster connective tissue cells: a histologic and quantitative radioautographic study with proline H3. Arch Oral Biol 1968;13:271.
12. Straffon LH, Han S S. Effects of varying concentrations of formocresol on RNA synthesis of connective tissue in sponge implants. Oral Surg 1970;29:915.
13. Garcia-Godoy F. Penetration and pulpal response by two concentrationsof formocresol using two methods of application. J Pedod 1981; 5:102.
14. Massler M, Mansukhani H. Effects of formocresol on the dentalpulp. J Dent Child 1959; 26:277.
15. Law DB, Lewis TM. Formocresol pulpotomy in deciduous teeth. J Am Dent Assoc 1964; 69:601.
16. Lewis B: Formaldehyde in dentistry: a review for the millennium. J Clin Pediatr Dent 1988; 22: 167-78.ities for old rationales. Pediatr Dent 1994; 16: 403-9.
17. Berger J. Pulp tissue reaction from formocresol and zinc oxide and eugenol. J Dent Child 1965;32:13.
18. Berger JE: A review of erroneously labeled “mummification” techniques of pulp therapy. Oral Surg. 1972; 34: 131-44.
19. Fuks AB et al: Assessment of a 2% buffered gluteraldehyde solution in pulpotomized primary teeth of schoolchildren, (Dent Child 57:371-375, 1990.
20. Fuks AB, Holan G, Davis JM, Fidelman E: Ferric sulfate versus dilute formocresol in pulpotomized primary molars: long-term follow up. Pediatr Dent 1997; 19: 327-30new modalities
21. Nakashima M. Induction of dentin formation on canine amputated pulp by recombinant human bone morphogenetic proteins (BMP)-2 and -4. J Dent Res 1994;73:1515.
22. McDonald RE, Avery DR. Treatment of deep caries, vital pulpexposure and pulpless teeth. In: McDonald RE, Avery DR,editors. Dentistry for the child and adolescent. 6th ed. St.Louis: CV Mosby; 1995. p. 428–54.
23. P.J.Waterhouse, JH Nunn and J.M.Whitworth. An Investigation of the relative efficacy of Buckley’s Formocresol and Calcium Hydroxide in primary molar vital pulp therapy.BDJ.2000;188;32-36
|
|
|
|
|
|
|