INTRODUCTION
Saving each tooth of the dental arch for as long a time as possible is the first and foremost goal of endodontic therapy. However, endodontic success greatly depend upon achieving a perfect and hermetic seal at the root.
Root canal anatomy, length, shape and configuration are so much varied that no set rules can be applied in any regard and with only practical experience and clinical judgments the anatomy of the canals can be foretold.
Being a hand operative procedure, endodontic therapy requires fine skill and a very sharp tactile sense. This skill lies in the ability of the operator to interpret the action of the instrument as he manipulates it in the canal. With this faculty
developed to the fullest potential, skillful endodontic procedures can be performed without direct vision. A good knowledge of working surfaces of endodontic hand instruments permit the operator to select the correct instrument and
use it in a proper sequence. A thorough understanding of the tip configuration of root canal instrument which is the only guiding factor once the instrument is in the canal. However endodontic hand instruments vary extremely. They are perhaps the most misunderstood and misused in the dental instrumentarium. Selection of an instrument for a particular procedure is merely a matter of personal choice. No standardization existed considering the influence of design of endodontic instruments on tactile sensation. Digital tactile sensation being the single most important factor in locating the root apex. This study was taken up to evaluate the working efficacy in tactile sensation of the most commonly used instruments in endodontic therapy i. e K. file, the reamer and the H-file. With tactile sensitivity as the sole parameter, this project further examined the variation in tactile sensitivity between postgraduate receiving endodontic training and undergraduates at clinical level.
MATERIAL AND METHODS
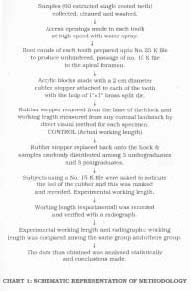
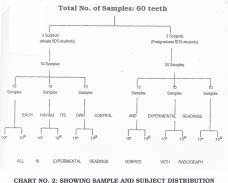
Samples constituted of sixty caries free, unfilled, freshly extracted human permanent single rooted teeth, with both crown and root intact each of the specimen was thoroughly cleaned, to ward off all debris and stored in normal saline for
experimentation. The investigation commenced by preparing an access opening in each of the collected teeth. This was done with the assistance of an appropriately sized inverted come, diamond point at high speed with a water spray. The initial point of entry was, the area just above the cingulum for the incisors while for premolars it was slightly buccal to the central groove, with the bur directed along the long axis of the root. After the “drop in the roof” was felt, a long shanked No. 4 or 6 round bur was used in a “sweeping out motion” in an incisal direction to facilitate a clear direct access. Ultimately, a end cutting fissured diamond point was used to refine the final shape of the access opening, which emerged to be roughly triangular in incisors, white it being round in premolars. Next, using a #15,# 20,and #25 K file of 25 mm
length the root canals of each of the specimens was prepared in a systematic step back manner, with intermittent irrigation with 5.2% sodium hypochloride solution by a hypodermic syringe, thus ensuring sure that # 15 K file of 25 mm length reached the apical foramen without any hindrance or canal obstruction. Now, a circular rubber stopper of approximately 2 cm diameter was selected, to be positioned in constant contact with the root aped of each of the chosen sample. A 1" 1" brass split die was utilized to make blocks of auto-polymerizing resin. Vaseline was applied on all the inner surfaces of the die with a plastic instrument. After the circular rubber stoppers were placed in the well of the brass die. Self polymerizing resin was put into the die by incremental method that is small amounts of powder-liquid alternating at regular intervals, till the tooth with the rubber stopper at the root apex was uniformly covered with acrylic upto cementoenamel junction, taking care not to block the coronal access opening with acrylic. The resin was allowed to set and after it was hard, the split die was opened by placing a wax knife in the
 | Fig. 1: Materials used in the study
 |
grove along the walls and the bade of the die, forcing it split open to obtain a black . the excess resin all over, was removed with a acrylic trimmer at low speed. The trimmer was also used to remove excess resin at the bade of the block in a manner to expose the rubber stopper making its entire outline visible. Vertical grooves were cut in the base of the resin block to expose about one half of the thickness of the rubber stopper, this facilitating its easy removal and placement as and when required. The final shine to the resin frame work was given using denture finishing stones ,
and sand paper at lower speed followed by polishing with pumice slurry on a buff . similarly, all the sixty samples with individual circular rubber stopper were placed into their respective acrylic blocks.
METHODOLOGY
After numbering the samples from 1-60,the rubber stopper under each of the specimen was removed to make the root apex visible. A, #15 K file of 25 mm length., to which an endodontic marker was attached, was passed through the
coronal access opening slowly, until the tip of the file was just seen to come out of the root apex. The endodontic marker was so adjusted that the tip of the file was just at the apex of the root. Now the file was withdrawn and the distance between the endodontic marker and the file tip was measured and recorded in millimeters. This gave the actual working length for that specimen which acted as a control measurement for that sample. The rubber stopper was now replaced back. The actual working length of all the specimen was recorded in a similar manner which were the control recording for the respective samples. Next
 | Fig. 2: Fiad Explorer XL 65KV (Dental X-ray Machine)
|
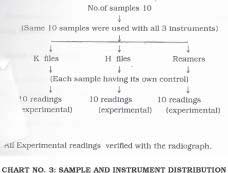
three undergraduate students at clinical level and three postgraduates undergoing endodontic training were selected and were the subjects in the study. Sample were randomly distributed equally i.e. 10 each among all the six subjects.
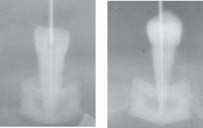
Each of the subjects was given a #15 K file of 25 mm length, with an endodontic marker. Wearing well fitting latex gloves each operator passed the #15 K file of 25 mm length with a marker, in the root canal till they could just feel the softness of the rubber stopper with the tip of the file. The endodontic marker was adjusted at a point when the operator could just feel the softness of the rubber. With the file in the canal, the acrylic block was placed on a wooden block of 2" 4" that had a horizontal slot at one end, into which an intra oral periapical radiographic film was fitted, such that radiographic film was parallel to the long axis of the tooth. The radiographic cone was adjusted in such a manner that the cone tip was in the centre of the acrylic block and a radiograph was shot.
 | Fig. 3: Photograph of radiographs showing samples in which rubber stopper did not touch the root apex
|
 | Fig. 4: Photograph of radiograph showing in root apex location by undergraduate student using #15 K file
|
 | Fig. 5: Photo of radiograph showing root apex location by postgraduate student using #15 K file
|
The file was removed and the distance between the endodontic experimental working length as obtained by the operator. The radiograph was developed and fixed and then finally dried. Placing it on a view box, the distance from the coronal
landmark and the file tip was measured and recorded in millimeters from the radiograph. This formed the radiographic working length similar procedure was performed by each of the operator on their respective 10 samples. It was observed
that there was a marked difference in the performance of undergraduates and postgraduates, hence when H. files and reamers were to be used for subsequent experimentation undergraduates were to be used for subsequent experimentation undergraduates were excluded and only postgraduates were given the samples to use H.
files and reamer. Similar procedure was adopted as done for K files . Thus the data so obtained was subjected to statistical analysis readings obtained, tabulated and analysed.
 | Fig. 6: Photographs of radiographs showing root apex location by #15 K file
|
 | Fig. 7: Photographs of radiographs showing root apex apex location by #15 reamer
|
 | Fig. 8: Photograph of radiographs showing root apex location by #15 H file
|
 |
|
 |
|
 |
|
DISCUSSION
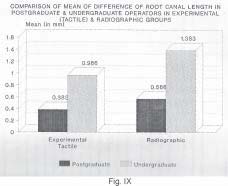
In routine endodontic practice, it has been that commercially available endodontic hand instruments are much varied as regards to their flute design, handle design, length etc., each claiming its superiority over the other. A number of previous studies have been conducted to evaluate cutting efficiency, instrument flexibility, standardizing them, however, a very little work has been done on tactile efficacy of various commercially available endodontic instruments. Digital tactile ensation being the premier and still the most effective method of root apex location as advocated by Seidberg19, this study was taken up to evaluate variation in tactile sensation at the root apex using the most commonly used instruments in endodontic, i.e. K-file, reamers and H-files. Furthermore, according to Samuel Luks18, tactile sense, is at its best when finger pressure while holding the instrument handle is at a minimum and the force exerted on the instrument during instrumentation is not excessive. Thus this project compared different root canal instruments and working efficiency in tactile sensation between post graduate practicing endodontics and ndergraduate students at clinical level. nalysing the result obtained it was observe that on an average the experimental (tactile) root canal length for postgraduates ware 0.08% higher from the control while the same for undergraduates was 0.925% higher from the control. This indicate a marked difference in working efficacy between the undergraduate student and postgraduate.
Similarly, comparing the radiographic working length it was seen that for the postgraduates it was 1.245% higher from the control reading. Thought radiograph showed a minor variance it was mandatory as it not only indicated the position of the file in the root canal with respect to the root apex but also verifild that if the root apex was a rigid contact with the ubber
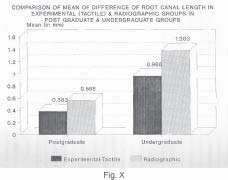
stopper. Hembrough et al.10 also believed that radiographs were indispensable for calculation of endodontic working length. Furthermore, it was seen that, experimental (tactile) differential root canal length in undergraduate operators was 152.21% higher from the postgraduate operator, which were takes as base. Similary, radiographic differential root canal length for undergraduate operator was 144.34% higher from postgraduate operator. This is depicted in the from of a bar graph comparing the difference of canal lengths in postgraduates and undergraduate operator in experimental
(tactile) and radiographic groups.
Using pooled values and comparatively evaluating experimental (tactile) Vs radiographic values, it was seen that postgraduate ‘t’ value is not significant concluding that there was no significant difference in root canal lengths in experiment and radiographic groups for postgraduates. These result coincided with those obtained by Osion17, who examined the “in vitro” ability of existed in working length when teeth were radiographed in dried jaw bone and
radiographic working length of extracted.
But for the undergraduate, experimental (tactile) Vs radiographic comparison shows ‘t’ valued significant p<0.05, indicating a marked difference between experimental and radiographic reading in pooled undergraduate operators.
The variation of experimental (tactile) values from the radiographic values in both postgraduate and undergraduate group can attributed to slight magnification achieved while taking the radiograph.
Finally, a comparative evaluation experimental (postgraduate Vs undergraduate) and radiographic (postgraduate Vs undergraduate) values, indicate ‘t’ being highly significant i.e. for experimental and radiographic (postgraduate Vs
undergraduate) p<0.01. Hence, difference in root canal lengths differs significantly in undergraduate and postgraduate operators, in both experimental (tactile) and radiographic groups, (values being higher for undergraduates in both the groups). The study shows marked difference existed between tactile sensitivity of undergraduates and postgraduates proving undergraduates to be less skilled in locating the root apex by tactile sensitivity, and that undergraduates had relatively more chance of going beyond the apex. Sunada20 and lnoue et al..11 also reported that feeling the
root apex with an instrument requires a degree of tactile skill and endodontic practical experience.
As the study was done on single rooted with prepared canals and direct access to the apical foramen the undergraduate showed a great variance in locating the root apex, it was presumed that undergraduates working on posterior multirooted teeth with fine and curved canals would show a variance of extreme nature. Keeping this in view for the next stage of experimentation undergraduates were excluded and only postgraduates were selected for experimentation. With 10 samples each, postgraduate endodontist was asked to pass a Kfile, a reamer and H-file into the samples. Hence they indicated the feel of the softness of the rubber, a radiograph was lot, file withdrawn and measurement achieved.
Radiographic working length for each instrument also measured from the radiograph and recorded.
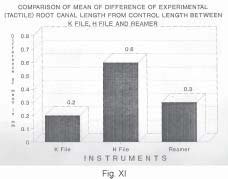
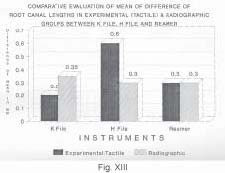
Comparatively evaluating K-files reamers and H-files (Table 14), it as seen that ‘t’ was significant (p<0.05) in experimental values for K-file Vs Hfile ( ‘t’=2.686) and H-file Vs reamer (‘t’=2.104), and was higher for H-file. However, for K-file Vs reamer ‘t’ values were insignificant (0.867) concluding that there was no significant difference in tactility between K-files and reamers as illustrated in bar diagram Fig 2 , ,,
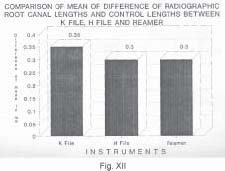
A comparison between reamers and K- file indicted that for both experimental (tactile) and radiographic values were higher for reamers.
 |
|
 |
|
 |
|
 |
|
 |
|
Thus from the above description. it is concluded that although, experimental (tactile) and radiographic values differed significantly from the control values for all the instrument, K-file rated best as for as location of root apex for tactile
sensation was concerned and the reason for this according the Samuel luks was that the spear point at the tip of the K-file as facilitated the tactile location of the apical formen. next came the reamers while lastly H-files, which always show a marked variation in locating the root apex. Hfile too has a spear point at the tip but has a tendency to get caught in the dentinal wall and produce a notch due to extremen sharpness of the tip cone and the adjoining flutes, leading to ledge formation or perforations.However, instrument handle length and diameter are other factors in optimum sensitivity
and control of endodontic hand instruments which are the subject of further investigation and clinical trial.
CONCLUSIONS
The following conclusion is drawn from the present study:
1. With digital tactile sense as the parameter analysis among K-file, H-file and reamers proved k-files to be best in tactile apex location followed by reamers and lastly the H-files.
2. Radiograph cannot fully interpret the actual working length nor does it can accurately indicate the position of the instrument in the root canal with respect to the root apex.
3. With the undergraduates showing a marked less proficiency in tactile apex location than postgraduates receiving endodontic training it is concluded that endodontic practice require high degree of digital tactile skill which can only be acquired by after good amount of specialized endidintic training and practical endodontic experience.
REFERENCE
1. Aurelio, A. James, Nahmias, Yosef, Gersteim, Harold: A model for demonstrating an electronic canal length measuring device. J.O.E., Vol. 9, No. 12, Page569, 1983 (Dec.).
2. Becker, G.J., Lankelma, P., Wesselinks, P.R., Thrdon Van Velzen, S.K.: Electronic determination of root canal length.
J.O.E., Vol 12, NO. 12, Page 876-879, 1980 (Dec.).
3. Berman, Louis, H., Fleischman, Steven B.: Evalution of the accuracy of the Neosono-D Electronic Apex Locator. J.O.E.,
Vol 10, No.4, Page 164-167, 1984 (Aprill).
4. Chandler N., Bloxham G.: The influence of two handle designs and gloves on the performance of a stimulated endodentic task. J.O.E.; vol.16, No. 11, page 541-2, 1990 (Nov.).
5. Chandler, Nicholas., Bloxham, Graeme: Effect of gloves on tactile discrimination using an endodontic model. Int. Endo.J., Vol. 23, page 97-99, 1990.
6. Cox, V.S., Brown, C.E. Jr, Bricdler, S.L., Newton, C.W.: Radiographic interpretation of endodontic file length. Oral
Surg, Oral Med, Oral Pathol, Vol 73, No. 3, Page 340-4, 1991 (Sep.).
7. Fouad, Ashraf F., Rivera, Eric M, Krell, Keith V.: Acurracy of the endex with Variation in canal irrigants and foramen
size. J.O.E., Vol. 19, No. 2, Page 63-7, 1993 (Feb.).
8. Fouab, Ashraf F., Krell, Keith V., Mckendry, Douglas T., Foorbusch, Gerald F., Oslon, Robert A.: J.O.E., Vol. 16, no.
9, Page 446-49, 1990 (Sep.).
9. Frank, Alfred L., Torabinejab, Mahmoud: An In vitro evalution of endex evalution epex locator. J.O.E., Vol. 19, No. 4, Page 177-79, 1993 (April).
10. Hembrough, Jiffrey H., Weine, F.S., Pisano, J.V.,Eskoz, N.: Accuracy of an Eloctronic Apex Locator: A clinical evaluation
in maxillary molars. J.O.E., Vol. 19, No. 5, Page 242-46,1993 (May).
11. Inoue, N., Skinner, D.H.: A simple and accurate way of measuring root canal length. J.O.E., Vol.11, No. 10, Page
421-27, 1985 (Oct.).
12. Inoue Noboru: An audiometric method for determining thelength of root. J. Canad. Dent. Assn. No. 9, Page 630-36,
1973.
13. Johnstein, T., Corcoran, J.F., Zillich, R.M.: The influence of the major and minor foramen diameter on apical electronic
probe measurement. J.O.E., Vol.16, No. 11, Page 520-22, 1990 (Nov.).
14. Kobayashi, C., Suda, H.: New electronic canal measuring device based upon ratio method. J.O.E., Vol. 20, No. 3, Page 111-114, 1994 (March).
15. McDonald, N.J., Horland, E.J.: An evaluation of apex locator endocater. J.O.E., Vol. 16, No. 1, Page 5-8, 1990 (Jan.).
16. Negm, M.M.: An instrument for measuring root canal length and apex location. A rapid technique. J. Oral Surg., Oral Med., Oral Pathol., Vol. 153, No. 4, Page 405-9, 1982 (April).
17. Oslon, A.k., Goerig, A.C. Cavataio. R.E., Luciano, J.: The ability of the radiograph to determine the location of the apical foramen. Int. Endod. J., Vol. 24, No. 1 Page 28-35, 1994 (Jan.).
18. Samuel Lucks: An analysis o froot canal instruments. J.AD.A., Vol. 50, page 85-92,1959 (March).
19. Seidberg, B.H., Alibrandi, B.V., Fine, H., Logue B Clinical investigation as measuring working lengths or root canals
with an electronic device and with digital tactile sense. J.A.D.A., Vol. 90, Page 379-87, 1975 (Feb.)
20. Sunada, I.: New method for measuring the length of the root canal. J.D. Res., Vol. 41, No. 2, Page 375-387, 1962 (March).
21. Treble, S.J., Chandler, N.P., Shaw, and J.R.: Tactile sensitivity of three endodontic instrument handles. Endod. Dent.
Traumato. 9: 77-78, 1993.
22. Trope, M., Rabie, G., Tronstad, and L.: Accuracy for an electronic apex locator under controlled clinical conditions.
Endod. Dent. Traumatol. 1: 142-145, 1985.
23. Ushiyama. J.: New principle and method for measuring the root canal length. J.O.E., Vol., 9, No. 3, Page 97-104, 1983 (Nov.)
24. Ushiyama, J.: Reliability and safety of the voltage gradient method of root canal instrument. J.O.E., Vol. 10, Bi.11 Page
532-37, 1984 (Nov.)
25. Ushiyama, J., Nakamura, M., Nakamura, Y.: A clinical evaluation of the voltage gradient method of measuring the
root canal length. J.O.E., Vol. 14, No. 6, Page 283-87, 1988 (June). |