Introduction
The articulation between the squamous part of the temporal bone and the head of the mandibular condyle is known as Temporomandibular Joint (TMJ).
Temporomandibular Disorders, commonly called TMD are a group of conditions that cause pain and dysfunction in the jaw joint and the muscles that control jaw movement.
Occlusal Appliance Therapy (Reversible)
Uses of occlusal appliances
1. To provide a more orthopedically stable joint position
2. To introduce an optimal occlusion that reorganizes the reflex muscular activity.
3. Protect the teeth and supporting structures from the abnormal forces.
The common types of appliances are the stabilization or the muscle relaxation appliance and the anterior positioning or the orthopedic repositioning appliance. The other types are the anterior bite plane, the posterior bite plane, the pivoting appliance and the soft or resilient appliance.
The most common form of treatment provided by dentists for TMD is occlusal appliance therapy(OAT). This may be otherwise referred to as a bite-raising appliance, occlusal splint, bite guard, or interocclusal orthopaedic device.[1]
An occlusal applianceis a removable device, usually made of hard acrylic that is custom made to fit over the occlusal surfaces the teeth in one arch, either the mandible or maxilla. Generally, it is constructed so that there is even occlusal contact with teeth of opposing arch in centric and anterior contact only lateral and protrusive excursions of the mandible. There are generally two types of occlusal appliances in common use:
The flat plane or stabilizationor muscle relaxationappliance
the anterior positioning or orthopedic repositioning appliance
Flat plane appliance - It covers all the teeth in the arch and its purpose is to relax the elevator muscles, provide joint stability and to protect the teeth from abnormal forces such as bruxism. There must be bilateral, equal intensity posterior occlusal contacts so that an environment of a stable physiological mandibular posture is created. Canine guidance should be created for lateral and protrusive excursions of the mandible. Most importantly, however, as pain, muscle activity, edema and inflammation subside, the resulting changes in maxillo-mandibular relationships must be compensated for by regular adjustments to the flat plane appliance. With improvement within the first weeks, then the patient should be re-evaluated for other factors that may require supplementary or a complete change in the treatment regimen.
Anterior repositioning appliancesare used less often because repositioning of the mandible over a period of time can result in irreversible changes to the occlusion such as bilateral posterior open bites. The purpose of these appliances is to alter the structural condyle-disc-fossa relationship in an effort to decrease adverse joint loading[2].
Centric Relation Splint:
This is also known as the Tanner appliance, the Fox appliance, the Michigan splint, superior positioning appliance or the stabilization appliance. This splint provides a temporary and removable ideal occlusion [Figure:1]
 | Fig.1 - Centric Relation Splint
 |
The stabilization appliance is given usually on the maxillary arch for the sake of stability.
When the appliance is in place, the condyles are in the most stable position in the glenoid fossa. The posterior also disocclude during lateral movements by canine guidance.
Indications
1. Patients having muscle hyperactivity during periods of stress
2. Patients having muscle hyperactivity due to centrally mediated myalgia and local muscle soreness.This appliance helps to reduce forces on the damaged teeth and to help in healing[3].
Locating The Centric Relation Position
The centric relation position is the most musculoskeletaly stable position of the mandible and hence it must be accurately located in the patient. This can be done by two methods.
1. The bimanual palpation method
2. using a flat anterior plane to disocclude about 3-6mm so that the posteriors are disocclude about 1-3 mm
Adjusting The Eccentric Guidance
The appliance is adjusted till all posterior eccentric contacts eliminated and only canine contacts remain.
The incisors may also be used to provide protrusive contacts and not one incisor is loaded singly.
The canine must have smooth and uninterrupted glides into protrusive and lateral movements
Anterior Positioning Appliance
This appliance is used to temporarily position the condyles more anterior then their musculoskeletaly stable position to relieve the existing symptoms [Figure:2.1 & 2.2].
 | Fig.2.1 - Anterior Repositioning Appliance
|
 | Fig.2.1 - Anterior Repositioning Appliance
|
Indications:
1. Disc derangement disorders
2. Joint sounds
3. Intermittent or chronic locking of the joints
4. Inflammatory disorders like retrodiscitis.
Fabrication Of The Appliance
The appliance does not extend onto the labial surfaces of the teeth and hence is more esthetic than the stabilization appliance.
The key to successful construction of the appliance is in locating the correct anterior stop. It is made on the anterior part of the appliance by asking the patient to protrude his mandible and finding the position in which the clicking and the joint pain is relieved.
Sometimes, stoppage of the clicking alone does not indicate that the mandible is positioned anterior to the retrodiscal tissue. So if symptoms fail to resolve, more advanced methods like arthroscopy and MRI may be used to ascertain the position of the mandible.
Adjustments
The patient is asked to wear the appliance only at night.
The normal stimulation of the retrodiscal tissue in the daytime is to promote fibrous healing of the tissue and enables it to resume function. If the patient has prolonged pain and finds relief in wearing the appliance during daytime, he can wear it till symptoms are reduced.
The type, extent and the chronicity of the disorder, determines the length of the time that the appliance is worm. If symptoms were relieved merely by increase in the vertical dimension, then a stabilizing appliance would be the treatment of choice
Anterior Bite Plane
This is also known as a Luciajig or, as an anterior de-programmer. This is a partial coverage appliance used for occlusal disengagement. By providing an ideal anterior guidance and temporarily disengaging the back teeth, a very tense masticatory musculature can be encouraged to relax.[5]
It is a hard acrylic appliance designed so that only the anterior teeth contact to disocclude the posteriors to eliminate any influence the posterior teeth have on the occlusion. [Figure:3,4].
 | Fig.3 - Anterior Bite Plane
|
 | Fig.4 - Anterior Bite Plane
|
Indications
1. Muscle disorders related to orthopedic instability or an acute change in the occlusal condition.
2. Short periods of parafunctional activity
With the anterior bite plane, which does not cover the posterior teeth, there is a great risk of the posterior teeth supra erupting and causing an anterior open bite. A stabilization appliance can be used in most cases where an anterior bite plane is used and must be preferred. When a full arch device is fabricated, the chance of supra eruption is avoided.
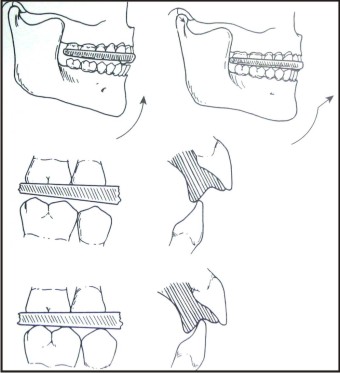
Posterior Bite Plane
It is a hard acrylic appliance, which covers the posterior mandibular teeth and is connected by a cast lingual bar. The objective of this appliance is to bring about changes in the vertical dimension and the mandibular positioning. [6]
Indications
1. When there is severe loss of vertical dimension.
2. Need to make major changes in the anterior positioning of the mandible.
This appliance is used in some disc derangement disorders.
The main risk of this appliance is the intrusion of the covered teeth and the supra eruption of the uncovered teeth. So full coverage must always be considered.
Pivoting Splint
• This is a hard acrylic appliance given over the mandibular teeth with only one occlusal contact on each side.
• This is given as far posteriorly as possible, the goal is to cause contact on the posteriors contact point when the anteriors are brought together to induce the condyles to pivot downward over the posterior pivoting points.[7] [Figure:5].
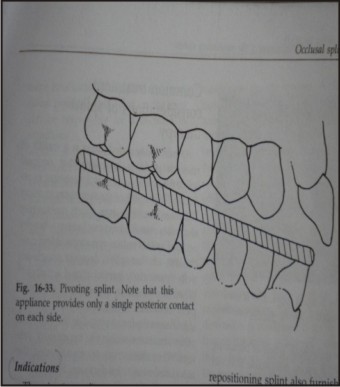 | Fig.5 - Pivoting Splint
|
Indications
• It is most useful in osteoarthritis. Originally, this appliance was thought to cause distraction of the condyles due to the pivot and it was used to treat joint sounds.
• But it has now been proved that it only causes loading of the joint with the condyles seated in the centric relation. This is because that the elevator muscles are located behind the pivot and cause elevation of the mandible
• Such an appliance should not be worn for more than a week as it will cause intrusion of the second molar on which the pivot has been constructed
Resilient Appliance: The Soft Bite Guard (SBG)
This splint, constructed of polyvinyl, is of uniform thickness and no attempt is made to balance it on the opposing teeth. It does not; therefore provide an occlusion of any specific prescription. It is quickly, easy and economical to make.
Fabrication
This polyvinyl splint is made by a vacuum forming technique onto either an upper or lower model. Occlusal registration is not necessary. [Figure:6].
 | Fig.6 - Resilient Appliance
|
Indications
• These splints can be considered as a first line simple emergency treatment for patients with symptoms of pain dysfunction syndrome, but it is not normally used as the sole treatment.
• The mode of action must be conjecture and is uncertain. It may absorb occlusal forces by virtue of its soft nature or it may act as a habit breaker (cognitive awareness theory)
• This splint cannot be occlusally adjusted.
• Athletic mouth guards
• Persons having severe bruxism
• Persons having chronic sinusitis with resultant severe sensitivity of posterior teeth.
• On occasion, however, these splints can exacerbate rather than alleviate the condition, as wearing such an appliance may cause parafunctioning to an even greater degree. Careful monitoring, therefore, is essential.
• The splint is generally worn at night, and if successful, the beneficial effects will have become apparent within 6 weeks.
• These splints are only functional for 4-6 months as they become firm and lose their flexibility.
The Localized Occlusal Interference Splint (LOIS):
• This splint is designed to deliberately overload the proprioceptive fibers of four teeth, as no other teeth touch during closure.
• Thus parafunctioning, especially clenching, is discouraged.
• Another effect of this splint is to increase the vertical component of the anterior guidance during lateral excursion. This may eliminate posterior interferences
Fabrication
• This splint is made from upper and lower impressions with a centric occlusion wax registration.
• It consists of an upper heat cured acrylic palate retained by Adams cribs or ball end clasps on the first molars and has two occlusally related balls ended wires anteriorly, generally on the canines or premolars, which deliberately interfere with the occlusion.
Indications
• This is an appliance used for patients who habitually clench teeth or who are bruxists. They may or may not have clinical symptoms of a TMD.
• The object of these splints is to 'overload' the periodontal receptors to two teeth in each arch, thereby reflexly reducing the muscle force generated by the patient. Its main function is as a 'habit breaker'.
Mandibular Orthopaedic Repositioning Appliance (MORA)
o The mandibular orthopedic repositioning appliance (MORA) is a mandibular posterior coverage splint, which usually includes a lingual bar connecting the posterior segments of the splint. It is made of hard acrylic and is also known as the Gelb splint. [Figure:7].
o Occlusal indentations serve to hold the mandible in a protrusive position.
o Although MORAs are comfortable for most patients to wear and may give relief of pain, there use may lead to malocclusion which is often more severe than malocclusions encountered with full coverage repositioning devices
o Because MORAs cover the posterior teeth only, dentoalveolar changes may occur such as intrusion of posterior teeth and extrusion of anterior teeth, both to variable degrees.
o It has been suggested that such appliances should be used either part time or adjusted to or replaced with a stabilization splint as soon as pain and dysfunction are minimized.
o Limiting the use of MORAs to 6 to12 weeks in duration is considered appropriate in order to avoid or minimize the occlusal sequelae.
 | Fig.7 - Mandibular Orthopaedic Repositioning Appliance
|
The Deprogrammer:
Rationale of using a deprogrammer
To produce a forced relaxation of the temporalis, masseter and pterygoid muscles allowing the TM joints to rest in a functionally comfortable position in the fossa.
The butterfly deprogrammer, followed by a bruxing guard built using the new functional (deprogrammed) bite registration can bring about immediate and permanent relief of pain in a majority of TMD cases.
The Deprogrammer Accomplishes Three Goals
1. The deprogrammer should bring about nearly immediate relief of acute symptoms. In general, pain is reduced or eliminated within one or two hours of insertion. Muscle relaxants, analgesics or other drugs are generally unnecessary.
2. The butterfly deprogrammer helps to confirm the diagnosis of TMD, and the appropriateness of jaw repositioning as a treatment.
3. It brings about relaxation of masticatory structures and allows for the determination of a functional centric jaw relation and the construction of a deprogrammed bite appliance.
It may be worn while sleeping and at other critical times of the day when the patient is likely to be bruxing or clenching.
The Nti - Tss System:
Dr. James P. Boydintroduced the NTI system. The tension suppression system is a prefabricated polycarbonate matrix that is worn over the front teeth while sleeping.
Indication
Internal joint derangements
Obtaining ideal condylar orientation prior to comprehensive occlusal therapy
Treatment and prevention of MPD
Bruxism night guard
Migraine prevention/relief
Fabrication
It is a simple modification of the traditional anterior deprogrammer, thereby preventing canine and posterior teeth contacting in parafunctional movement
Excessive vertical opening will allow for a strain on a TMJ in excursive movement and may encourage a clenching response. So vertical opening must be kept to a minimum, without allowing for canine or posterior teeth occluding. [Figure:8,9,10].
 | Fig.8 - The Nti-tss System (1)
|
 | Fig.9 - The Nti-tss System (2)
|
 | Fig.10 - The Nti-tss System (3)
|
Anterior Midline Stop
(AMPS - anterior midline point stop) An object placed in the mouth on the front teeth reduces the temporalis contraction intensity to a greater extent. The AMPS can be used with other appliances with specific modifications to prevent temporalis contraction intensity and thereby in treatment and preventive therapies
Therapeutic Motion of the Joint (“TMJ”)
Based on active unstrained neuromuscularly integrative movements to the temporomandibular joints performed by the patient, using an Anterior Midline Point Stop (AMPS) appliance.
Unlike a “deprogrammer,” which can allow for canine contact on the device in excursive movement, the AMPS appliance’s design of a narrow horizontal ramp parallel to the occlusal plane prevents canine and posterior teeth from occluding, thereby allowing for unstrained protrusion and lateral excursions.
This allows controlled, unstrained exercises to be performed by the patient, to help return intra-articular health and function of the joint
General Features Of Appliance Therapy
Principles of working of a splint[8]
There are five theories concerning the mode of splint action.
1) The occlusal disengagement theory suggests that providing an ideal occlusion by the use of splint therapy reduces abnormal muscle activity.
2) The same is true of the maxillo-mandibular realignment theory, which aims to produce 'neuromuscular balance'. This presupposes that the pre-existing mandibular position is incorrect, thereby causing an 'imbalance'.
3) The resorted vertical dimension theory is based on the concept that the patient has lost vertical height thus causing abnormal muscle activity with presumable, an altered condyle / disc relationship. Restoration to the 'correct vertical height', it is suggested, allows the muscles to function at their 'correct length'.
These terms, however, are not satisfactorily defined. Furthermore, as general principal, permanent changes to the dentition as the first line of treatment can rarely, if ever, be justified
4) The TMJ repositioning theory implies that the condyle should be repositioned within the glenoid fossa. It has been suggested that the most desirable condylar position can be attained by the use of radiographs. [9]
Evidence indicates this is wrong. While a repositioning splint is used to treat an internal (intracapsular) derangement as a temporary and therapeutic appliance, there is no evidence to support the need to restore the occlusion permanently to what should be regarded as being only a temporary treatment position.
5) Finally, the cognitive awareness theory could be applied to all splints. It is based upon the concept that having something in the mouth alters behavior and the opportunity to indulge in harmful muscle activity is reduced. Apart from the physiological effect, this theory also recognizes the existence of a placebo effect
Appliances, irrespective of their design and intended use, create the following effects.[10]
1. They temporarily alter the existing occlusal condition
2. They alter the condyle to a more musculoskeletaly stable position or more structural and functional position.
3. They cause an increase in the vertical dimension.
4. They bring about cognitive awareness in the patient regarding their parafunctional activity and help to control them.
5. Placebo effect to the confident and calm method in which the clinician deals with the patient, reducing his anxiety levels and bringing about beneficial effects.
6. Increased peripheral input to the CNS causing decrease in bruxing activity
References
1. Okeson Management of Temporomandibular Disorders and Occlusion, 4th Ed.
2. Peter E. Dawson Evaluation diagnosis and Treatment of Occlusal problems, 2nd Ed
3. Capp NJ, Clayton JA. A technique for evaluation of centric relation tooth contacts.Part II: following use of an occlusal splint for treatment of temporomandibular joint dysfunction. J Prosthet Dent. 1985;54(5):697-705.
4. H. Clifton Simmons III, S. Julian Gibbs. Anterior Repositioning Appliance Therapy for TMJ Disorders: Specific Symptoms Relieved and Relationship to Disk Status on MRI.The Journal of Craniomandibular Practice 2005;23(2):89-99.
5. Bolender CJ. Orthodontic treatment of overbite by the Tip Edge technique in conjunction with an anterior bite elevator: Part 1. Orthod Fr. 2001;72(4):375-86.
6. Ari-Demirkaya A, Biren S, Ozkan H, Kucukkeles N. Comparison of deep bite and open bite cases: normative data for condylar positions, paths and radiographic appearances. J Oral Rehabil. 2004;31(3):213-24.
7. Tim J. Dylina, DDS : A common-sense approach to splint therapy Journal of Prosthetic Dentistry 2001; 86(5):539.
8. Faulkner KD. Bruxism: a review of the literature. Part I. Aust Dent J. 1990 Jun;35(3):266-76
9. Dabadie M, Renner RP. Mechanical evaluation of splint therapy in treatment of the edentulous patient. J Prosthet Dent. 1990 Jan;63(1):52-5.
10. Cranio The immediate effect of the variation of anteroposterior laterotrusive contacts on the elevator EMG activity.1993; 11:184-191.
11. Tim J. Dylina, DDS : A common-sense approach to splint therapy Journal of Prosthetic Dentistry 2001; 86(5):539
|