Introduction
Under normal circumstances a tooth erupts when the root development is three- quarter of its final root length. The mandibular canines have marginally more root development when they erupt[1]. Infrequently mandibular permanent canines fail to erupt and are termed as impacted[2], [3]. It can be due to an obstruction from an odontome, over retained deciduous canine, supernumerary tooth, dentigerous or radicular cyst or frequently without any observable cause[4].
Occasionally it can become grossly displaced and has a capacity to travel large distances by crossing midlines, embedded in chin prominence or moving distally on the buccal side of first molar[5],[6]. Generally there are no symptoms of pain or selling associated with the impaction. It can go undetected for many years until a dentist notices the over- retained deciduous tooth[4].
When the eruption potential is arrested the tooth may stay in the basal bone and the root develops vertically downward towards the lower border of mandible.
A Panaromic radiograph gives a better view for such impactions as it is difficult to insert periapical film deep into the lingual Sulcus.
Case Report
A 17 year old male patient reported to the Department of Orthodontics and Dentofacial Orthopaedics, SBB Dental College with a chief complaint of rotated upper right side teeth. On examination rotation of # 13 and cross bite in relation to # 23 were noted. Moreover # 73 was over retained and # 33, 35 were missing. Patient gave a history of extraction of # 35 as it was grossly decayed. On examination of radiograph, # 33 was horizontally impacted crossing the midline. Further investigation of CBCT was carried out to find the exact relation of impacted # 33 with the adjacent teeth roots. CBCT showed horizontal impaction of # 33 in the periapical region of teeth # 44, 43, 42, 41, 31, 32, 73 largely labial to the apices of these teeth. The root apex of the tooth #43 apposed the lingual aspect of the pericoronal follicle surrounding impacted #33. The tooth was located such that the labial surface of the crown and the root of the impacted tooth apposed the adjoining labial mandibular cortex. There was acute mesio- lingual (hook-like) dilaceration of the apical third of the root in the region of #32, 73. The impacted tooth revealed normal morphology of crown and the coronal- radicular pulp with a Vertucci’s Type I root canal morphology. Mild dilacerations of the pericoronal follicle was noted causing expansion and thinning of the adjoining labial cortical plate .Focal effacement of the buccal cortex was also seen. #73 was also noted with root resorption of the apical third (Images 1 - 4).
 | Figure 1 – The root apex of the tooth #43 apposed the lingual aspect of the pericoronal follicle surrounding impacted #33.
 |
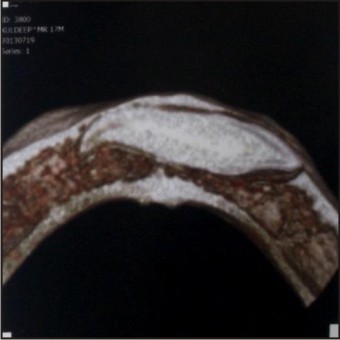 | Figure 2 - Acute mesio- lingual (hook-like) dilaceration of the apical third of the root in the region of #32, 73.
|
 | Figure 3 - Tooth was located such that the labial surface of the crown and the root of the impacted tooth apposed the adjoining labial mandibular cortex.
|
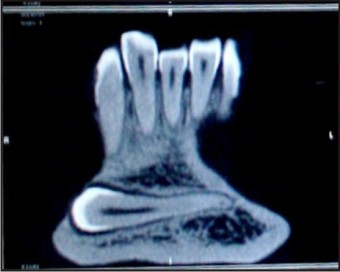 | Figure 4 - Horizontal impaction of # 33 in the periapical region of teeth # 44, 43, 42, 41, 31, 32, 73 largely labial to the apices of these teeth.
|
Discussion
Impacted canines are not uncommon in clinical practice, but intraosseous movement of impacted canines crossing the midline (transmigration) is a rare phenomenon. Radiographic examination is necessary to diagnose impacted transmigrant canines, among other anomalies. Surgical extraction is the treatment of choice for patients with transmigrant canines involving associated pathology. In some cases, the management of asymptomatic impaction can be limited to periodic clinical and follow-up visits. The absence of the permanent canine within the arch beyond the normal time of eruption suggests the presence of an impacted canine. A transmigrant canine may develop an associated pathology. The use of a panoramic radiograph is imperative and is recommended for discovering such rare malpositions. If the mandibular canine that has migrated across the mandible is associated with pathology, it may be removed. Otherwise, it should be kept under observation.[4] Panoramic radiograph provides a fair view of the horizontally impacted mandibular canines in mesio- distal plane. A true occlusal view is required to accurately localize the tooth in the third dimension.[5] In the midline region, the missing aspect will be depicted on the lateral cephalometric film that will have been taken for diagnosis of what initially appeared to the routine orthodontic treatment[6]. CBCT gives a clear three dimensional position of the impacted tooth and its relation to the roots of the adjacent teeth. In such type of cases extraction may sometimes be the only practical line of treatment available. It is due to presence of roots of adjacent teeth and narrow dimensions of the mandible[8]. There won’t be sufficient space to correct position of the tooth orthodontically. If the diagnosis of canine impaction and transmigration in patients is made earlier, it is possible that the tooth might have been in a better position for orthodontic eruption into the arch. Careful patient selection and preparation are therefore essential, as is cooperation between the orthodontist and oral surgeon.[9]
Conclusion
Mandibular permanent canine impactions are infrequent. Occasionally it can cross midlines, and gets embedded in chin prominence. CBCT gives a clear three dimensional position of the impacted tooth and its relation to the roots of the adjacent teeth. In such type of horizontal impactions extraction is the only practical solution. If a mandibular canine tooth is impacted, not only is surgical exposure sufficient but also traction force must be applied orthodontically after the surgical exposure. In addition, age influences the success of the treatment on impacted mandibular canine teeth more than the position and impaction level of the teeth.[10]
References
1. Gron A-M. Prediction of tooth emergence. J Dent Res 1962; 41: 573-85
2. Kuftinec MM, Shapira Y, Nahlieli O. A case report: Bilateral transmigration of impacted mandibular canines. J Am Dent Assoc 1995; 126: 1022-4
3. Shapira Y. Bilateral transposition of mandibular canines and lateral incisors: orthodontic management of a case. Br J Orthod 1978; 5: 207-9
4. Auluck A1, Nagpal A, Setty S, Pai KM, Sunny J Transmigration of impacted mandibular canines--report of 4 cases. J Can Dent Assoc. 2006 Apr; 72(3):249-52.
5. Becker A. The orthodontic treatment of impacted teeth. Second ed. Informa healthcare: 2007
6. Mupparapu M. Pattern of intra- osseous transmigration and ectopic eruption of mandibular canines: review of literature and report of nine additional cases. Dentomaxillofac Radiol 2002; 31:355-60
7. Peck S. On the phenomenon of intraosseous migration of unerupting teeth. Am J Orthod Dentofacial Orthop 1998; 113: 515-17
8. González-Sánchez MA1, Berini-Aytés L, Gay-Escoda C. Transmigrant impacted mandibular canines: a retrospective study of 15 cases. J Am Dent Assoc. 2007 Nov; 138(11):1450-5.
9. Celikoglu M1, Kamak H, Oktay H. Investigation of transmigrated and impacted maxillary and mandibular canine teeth in an orthodontic patient population. J Oral Maxillofac Surg. 2010 May;68(5):1001-6. doi: 10.1016/j.joms.2009.09.006. Epub 2010 Feb 25.
10. Aras MH1, Halicioğlu K, Yavuz MS, Çağlaroğlu M Evaluation of surgical-orthodontic treatments on impacted mandibular canines. Med Oral Patol Oral Cir Bucal. 2011 Nov 1;16(7):e925-8.
|