Introduction
Tooth trauma involving Coronal fractures of the anterior teeth are a common form of dental trauma that mainly affects children and adolescents.[1],[2] Approximately 25% of the population under the age of 18 years sustains traumatic injury in the form of anterior crown fracture. Accidental fall and blows or trauma during sports activities are the main reasons for injury in more than 40% and 20% of cases, respectively. The maxillary central incisors are most often injured in the accidents.2Many factors influence the management coronal teeth fractures, including extent of fracture, endodontic involvement, alveolar bone fracture, pattern of fracture restorability of fractured tooth, secondary traumatic injuries, presence/absence of fractured tooth fragment, occlusion and time.[3],[4],[5]
Traumatic injuries involving tooth fracture can be treated by reattachment of the tooth fragments using an adhesive system to provide what is considered to be the most conservative of restoration especially when there is minimum violation of the biological width.[6],[7],[8] Reattachment using modern dentine bonding agents may achieve functional and aesthetic success for up to 7 years and additionally generates a positive psychological response.[9]
This article reports a coronal tooth fracture case that was successfully treated using tooth fragment reattachment.
Case Report
A 25 year old male patient reported to the department of Conservative dentistry and Endodontics at National Dental College and Hospital sustaining a complicated crown fracture to his maxillary right canine due to a road accident (Figure 1). Fractured tooth fragment was still attached to the tooth with the help of gingival fibers (Figure 2). Clinical and radiographic examination revealed complicated oblique crown fracture that extended subgingivally on palatal area. The fracture fragment was carefully removed after anaesthetizing the patient. This fragment was washed under running water and stored in normal saline to prevent dehydration. After explaining all the possible treatment options to the patient, the patient desired to go for tooth fragment reattachment and maintain the tooth.
Root canal treatment was then carried out in the concerned tooth. To gain access to the subgingival fracture line and verify the extent of fracture, a lingual flap was raised (Figure 3). The root surface was recontoured with the finishing bur in order to facilitate healing. The fracture fragment was then etched with 37% orthophosphoric acid, rinsed, blot dried and then bonding agent was applied. Gutta percha was removed from the tooth till cement-enamel junction and the access cavity was then filled with flowable composite to make a composite rod. Tooth surface was similarly treated with etchant, rinsed and bonding agent was applied. Composite resin was applied to both tooth and fragment and the fragment was then carefully seated on the tooth and light cured on all surfaces. A firm pressure was applied on the fragment during curing in order to ensure its close apposition to the tooth (Figure 4 and 5). Excess material was removed after curing and was polished (ENHANCE polishing kit -Dentsply). Follow up was carried out after 3 months, 6 months, 1 year during which tooth remained normal in function and esthetics.
 | Fig 1 : Preoperative View
 |
 | Fig 2 : Fracture Fragment
|
 | Fig 3 : Access Opening
|
 | Fig 4 : Post Operative View
|
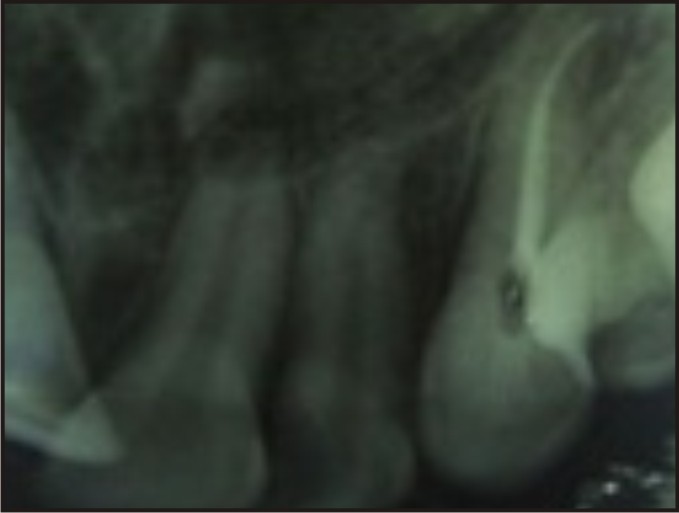 | Fig 5 : Post Operative X-ray
|
Discussion
Anterior tooth fracture can be most traumatic to a young patient, but the remarkable advancement of adhesive systems and resin composites has given promising results in reattachment of a fractured tooth thereby posing a positive emotional and social response from the patient for preservation of natural tooth structure.[8],[9],[10] One important complication in the present case was the subgingival extension of fractured margin on the palatal area. Upon probing this area during clinical examination it was determined that the biological width was only minimally invaded and that bone recontouring via crown lengthening would not be indicated or required as long as restorative margin was placed at or above the level of cemento-enamel junction. However, a dry and clean working field with proper use of bonding materials is the key for achieving success in adhesive dentistry. Short and medium term success outcomes have been seen in the previous reports.[8], [9], [11] Hence it can be concluded that reattachment of coronal tooth fragment is a viable technique that restores function and esthetics with a very conservative approach and the technique can be used as a treatment option in coronal fracture of anterior teeth especially in young patients.
References
1. Dietschi D, Jacoby T, Dietschi JM, Schatz JP. Treatment of traumatic injuries in the front teeth: restorative aspects in crown fractures. Pract Periodontics Aesthet Dent 2000;12(8):751-8,quiz 760.
2. Hamilton FA, Hill FJ, Holloway PJ. An investigation of dento-alveolar trauma and its treatment in an adolescent population. Part 1: the prevelance and incidence of injuries and the extent and adequacy of treatment received. Br Dent J 1997; 182:91-5.
3. Olsburgh S, Jacoby T, Krejci I. Crown fractures in the permanent dentition: pulpal and restorative considerations. Dent Traumatol 2002; 18(3):103-15.
4. Reis A, Francci C, Loguercio AD, e tal. Re-attachment of anterior fractured teeth: Fracture strength using different techniques. Oper Dent 2001;26(3):287-94.
5. Andreasen FM, Noren JG, Andreasen JO et al. Long term survival of fragment bonding in the treatment of fractured crowns. Quintesscence Int 1995;26:669-81.
6. El- Askary FS, Ghalab OH, Eldemerdash FH et al. Reattachment of a severely traumatized maxillary central incisor, one year clinical evaluation: a case report. J Adhes Dent 2006;8(5):343-9.
7. Reis A, Loguercio AD, Kraul A, Matson E. Reattachment of fractured teeth: a review of literature regarding techniques and materials. Oper Dent 2004;29(2):226-33.
8. Rappelli G, Massaccesi C, Putignano A. Clinical procedures for the immediate reattachment of a tooth fragment. Dent Traumatol 2002;18(5):281-4.
9. Monteiro S Jr, Andrada MAC. Tooth fracture reattachment : Case reports. Quintessence Int 1990;21(4):261-70.
10. Maia EA, Baratieri LN, de Andrada MA, et al. Tooth fragment reattachment: Fundamentals of the technique and two case reports. Quintessence Int 2003;34(2):99-107.
11. Oz IA, Haytac MC, Toroglu MS. Multidisciplinary approach to the rehabilitation of the crown-root fracture with original fragment for immediate esthetics: a case report with 4-year follow-up. Dent Traumatol 2006;22(1):48-52.
|