Introduction
Early childhood caries, may be defined according to the American Academy of Pediatric Dentistry “as the presence of one or more decayed, missing (due to caries), or filled tooth surfaces in any primary tooth in a child 71 months of age or younger”. [1]
Despite the introduction of various novel techniques, restoring the primary anterior teeth to its previous function, form and esthetics presents a challenge to the Pediatric Dentist. The children who require this treatment are usually the youngest and least manageable group of patients.In addition to that, technical problems related to primary incisors have to be faced. These teeth have short and narrow crowns leaving only a small surface for bonding, a pulp chamber that is relatively large to the crown size and enamel which is inheritantly difficult to etch due to its aprismatic structure.[2]
Hence, use of a resin-based composite reinforced with polyethylene fibers is preferred and the technique is referred to as the 'short post technique,' which requires root canal treatment and a short composite post.[3] Presented herewith are clinical case reports of 3 early childhood caries patients, whose dentition was restored with Glass fibre reinforced composite resin posts (GFRC), a new generation of fiber posts.
Case Report
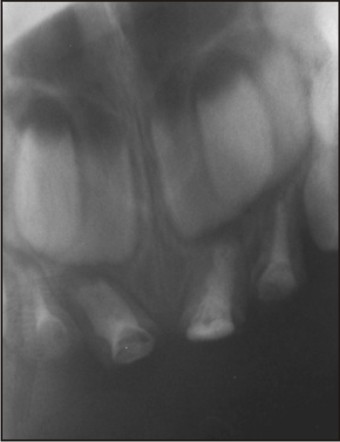
A four-year-old boy (CASE 1), reported to the Department of Pedodontics and Preventive Dentistry with the chief complaint of poor facial appearance due to discolored and worn out front teeth. Intra-oral examination revealed that 53, 54, 63, 64, 71, 72, 73, 74, 81, 82, 83, 84 were affected by dental carieswith root stumps of 52, 51, 61, and 62 (Fig 1). Intra-oral periapical radiographs revealed pulp involvement with respect to 52, 51, 61, 62. The root stumps were found to be firm, with less than 2 mm of the crown above the gingival margin being intact. Radiographic examination revealed no signs of exfoliation, with normal development of a permanent successor. Endodontic treatment and aesthetic rehabilitation of the mutilated incisors were planned as a part of full mouth rehabilitation.
 | Figure 1 – 4 Years Old Child (Case 1) With Grossly Decayed 51,52,61,62.
 |
Pulpectomy followed by obturation with respect to 51, 52, 61, 62 was carried out (Fig 2). The post space was prepared in the second appointment, three days later by removing approximately 3mm of zinc oxide eugenol material using a thin straight fissure bur. The post-space was air dried & a 1 mm base of glass ionomer cement (Fuji 2, GIC Corp, Tokyo, Japan) was placed to isolate the obturated material from the rest of post space.
 | Figure 2 – Obturation With Respect To 51,52,61,62.
|
The prepared post space was then cleaned with saline, air- dried & acid – etched with 37% phosphoric acid for 15 seconds. This space was rinsed and air dried with oil-free compressed air. A light cured bonding agent (3M ESPE, M.N, USA) was brushed on the etched surface and uniformly dispersed by a compressed air blast. It was then cured for 20 seconds using visible light curing unit.
Fibre splint by Polydentia SA Switzerland (2 mm) was then immersed in flowable composite resin (Estheticx flow, Dentsply) for post formation (Fig 3). Wet fibre material was inserted into root canal and condensed with some amount remaining in coronal area to function as post (Fig 4). It was then cured for 40 seconds.
The coronal enamel was then etched, bonded and artificial tooth was built up with composite. (Swisstec Coltene Whaledent) (Fig 5).
 | Figure 3 - Fibre Splint (2 Mm) Immersed In Flowable Composite Resin
|
 | Figure 4 - Wet Fibre Material Inserted Into Root Canal
|
 | Figure 5 - Coronal Enamel Etched, Bonded And Artificial Tooth Built Up With Composite
|
The patient was given post - operative instructions which included not to bite from the anterior teeth, avoid food which could cause staining for that day and to maintain oral hygiene using soft brush. The patient was followed up for a period of six months. No damage to any of the teeth was observed and restorations were found to be retained in place at the follow up visits.
Another child of five years (CASE 2) reported with grossly decayed maxillary incisors (Fig 6). Similar post and core treatment was performed with respect to 51,52,61,62 (Fig 7). However, 61 was pathologically resorbed and hence was advocated for extraction. Fibre - splint was then used as a splint from 52 to 62 to retain the pontic with respect to 61. It was found that the pontic was dislodged within a period of one month but the remaining three build ups were intact till six month follow period.
 | Figure 6 - 5 Years Old Child (Case 2) With Grossly Decayed 51,52,61,62.
|
 | Figure 7 - Post And Core Treatment Was Performed With Respect To 51,52,61,62.
|
Another three year old patient (CASE 3) reported to the department of pedodontics and preventive dentistry with extensively decayed 51, 61 (Fig 8). Similar post and core treatment was carried out for these teeth (Fig 9). It was seen that restorations of both 51 and 61 were lost after a period of one month.
 | Figure 8 - Three Years Old Child (Case 3) With Grossly Decayed 51, 61.
|
 | Figure 9 - Post And Core Treatment Performed With Respect To 51,61.
|
Discussion
The prevalence of ECC is high in India in the range of 50 – 70 % in 5 year old children as has been documented by several reports.[4],[5]
The necessity of re – establishing the integrity of primary teeth until their physiologic exfoliation has led to the development of newer techniques and materials.
When there is severe loss of coronal tooth structure, the use of posts placed inside the canal after endodontic treatment will give retention, provide stability to the reconstructed crown, and withstand masticatory forces in function.[6]
In the restoration of the anterior teeth, esthetics and mechanical resistance to fracture are of great importance for obtaining a long-lasting result, which can be attained through reinforcement of the resinous matrix with fibers.[7]
There are a variety of root posts used in pediatric dentistry. A resin composite post building up directly, resin composite short post placement, alpha or omega shaped orthodontic wires, stainless steel pre-fabricated posts, nickel- chromium cast posts with macro retentive elements, natural teeth from a tooth bank or reinforced fibers.[8]
The development of the fibre reinforced composite technology has brought a new material into the realm of metal-free adhesive esthetic dentistry.[9] Different fiber types such as glass fibers, carbon fibers, Kevlar fibers, vectran fibers, polyethylene fibers have been added to composite materials.[10]
Carbon fibers prevent fatigue fracture and strengthen composite materials, but they have a dark colour, which is undesirable esthetically. Kevlar fibers made of an aromatic polyamide increase the impact strength of composites but are unaesthetic and hence their use is limited. Vectran fibers are synthetic fibers made of aromatic polyesters. They show a good resistance to abrasion and impact strength, but they are expensive and not easily wielded.[11]
Polyethylene fibers are esthetic but their flexural strength is less as compared to glass fiber reinforced composite posts. The biological posts require the availability of a tooth bank and are still subject to new studies for future conclusions.[12]
Glass fiber-reinforced composite resin posts (GFRC) are new to the pediatric world and can be used as an alternative to the other post systems. The properties of fiber- reinforced posts are dependent on the nature of the matrix, fibers, interface strength, and geometry of reinforcement. The advantages of this material over the older fibers are greater flexural strength (1280 MPa), and over 650 MPa of the older fibers, greater ease of handling, can be used in high stress-bearing areas and can be bonded to any type of composites. Scanning electron microscopic (SEM) evaluation has shown clearly the formation of a hybrid layer, resin tags, and an adhesive lateral branch. Successful bonding minimizes the wedging effect of the post within the root canal, requires less dentin removal to accommodate a shorter and thinner post, and leads to lower susceptibility to tooth fracture. These posts are placed in cervical one third of the canals, to avoid interference with the process of permanent tooth eruption. When compared to other fibres, they are almost invisible in resinous matrix. Due to these reasons, they are the most appropriate and the best aesthetic strengtheners of composite materials.[13]
In our patients, two of the cases have shown favourable results while in the third case; both the restorations were lost in one month. This patient was three year old and was posing difficulty in the maintenance of salivary isolation. Also the patient was too young to follow post-operative instructions. A long term study is still needed to evaluate the success of fibre reinforced composites.
Conclusion
The treatment described in the case report is simple and effective and represents a promising alternative for rehabilitation of grossly destructed or fractured primary anterior teeth. This technique of glass fibre-reinforced composite resin post and core has presented the paediatric dental world with an additional treatment option.
References
1. American Academy of Pediatric Dentistry: Policy on baby bottle tooth decay/ECC revised 2008
2. Hartman CR. The open- face stainless steel crown: an esthetic technique. J Dent Child 50:31-33, 1983.
3. Pithan S, Vieira Rde S,Chain MC. Tensile bond strength of intracanal posts in primary anterior teeth: An in vitro study. J ClinPediatr Dent 2002;27:35-40
4. Kalra G, Bansal K, Sultan A Prevalence of Early Childhood Caries and Assessment of its Associated Risk Factors in Preschool Children of Urban Gurgaon, Haryana.Indian Journal of Dental Sciences 2011;3:12-16.
5. Bagramian RA, Garcia- Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent 2009;22:3-8.
6. Vieira Cl, Riberio CC. Polyethylene fiber tape used as a post and core in decayed primary anterior teeth. A treatment option J. Clin Pediatric Dent 2001;26:1-4.
7. Fidel SR, Sassone L, Alvares GR, Guimaraes RP, Fidel RA. Use of glass fiber post and composite resin in vertical fractures tooth. Dent Traumatol 2006;22:337-9.
8. Chunawalla YK, Zingade SS, Ahmed BMN, Thanawalla EA. Glass Fibre Reinforced Composite Resin Post & Core In Decayed Primary Anterior Teeth –A Case Report. IJCDS 2011; 2(1):55-59.
9. Meiers JC, Kazemi B, Donadio M. The influence of fiber reinforcement of composite on shear bond strengths to enamel. J.Prosthet Dent 2003,89:338-393.
10. Vitale MC, Caprioglio C, Matrignone A, Marcheisu U, Botticelli AR. Combined technique with polyethylene fibers and composite resins in restoration of traumatized anterior teeth. Dent Traumatol 2004;20:172-177
11. Uzun G, Hersek N ,Tincer T. Effect of five woven reinforcements on the impact and transverse strength of a denture base resin J. Prosthet Dent 1999;81:616-620.
12. DeBoer J, Vermilyea SG, Brady RE. The effect of carbon fibers orientation on the fatigue resistance and bending properties of two denture resins. J. Prosthet Dent 1984,51:119-121.
13. Viera CL, Ribeiro CC. Polyethylene fiber tape used as a post and core in decayed primary anterior teeth: a treatment option. J Clin Pediatr Dent 2001;26:1-4.
|