Introduction
Case Report
Case 1
30 years old female patient reported with chief complaint of irregular teeth and unaesthetic smile (Fig1a). On intra oral clinical examination there were spaces between the maxillary anterior teeth, 11 was overlapping 21, with short upper lip.
 | Fig 1 A : Case 1 Intra Oral Pre Operative (Before Treatment)
 |
Case 2
A female aged 35 years visited with complaint of pain, fractured filling and unsightly smile (Fig 1b).The patient’s medical history was unremarkable. On clinical examination revealed carious lesions in relation to 11,12,21,22, deep bite, retroclined maxillary central incisors, irregular teeth and 22 proclined and overlapping 21.
 | Fig 1 B : Case 2 Intra Oral Pre Operative (Before Treatment)
|
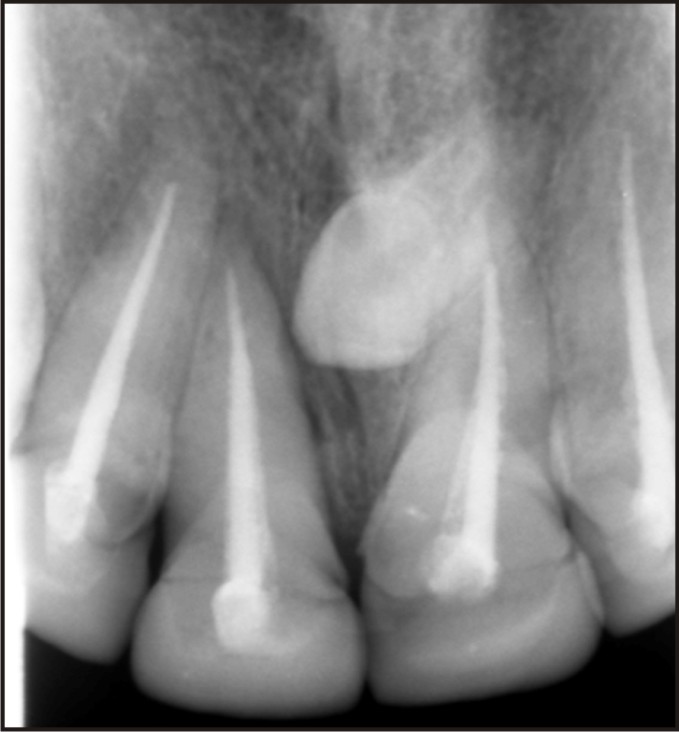
Diagnostic snap maxillary and mandibular arches impression were made in irreversible hydrocolloid for making diagnostic casts. The panoramic radiographs and intra oral peri apical radiographs were taken for maxillary anterior teeth. For case 1 Panoramic radiograph showed mesiodens supernumerary teeth (Fig 2). Orthodontic treatment was presented as first option to both the patients but they declined this treatment option, as the first patient was getting married after 3 months and the other patient did not wanted her teeth to be extracted. A diagnostic wax up of 4 maxillary anterior teeth (11, 12, 21, and 22) was then done, shown and discussed with patients (Fig 3a & 3b). The patients were satisfied with the outcome of diagnostic wax up and as suggested gave consent for elective endodontic treatment followed by all ceramic crowns in case 1 and ceramo metal crown for case 2 for enhancing their smile.
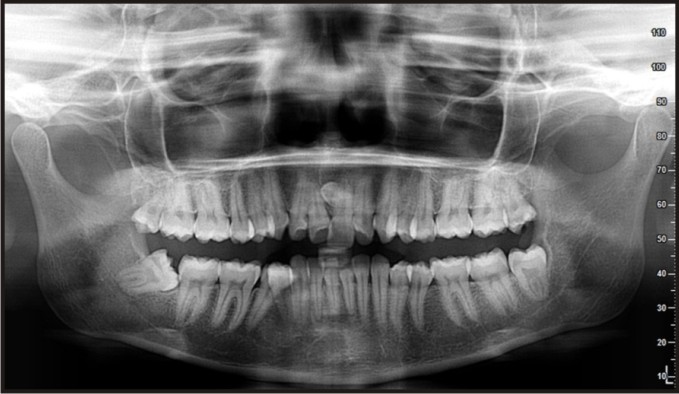 | Fig 2 : Panoramic Radiograph
|
 | Fig 3 A : Case 1 Diagnostic Wax Up Of Maxillary Anterior Teeth 11,12,21,22.
|
 | Fig 3 B : Case 2 Diagnostic Wax Up Of Maxillary Anterior Teeth 11,12,21,22
|
The option of ceramic laminates was ruled out as the existing alignment of teeth demanded greater preparation. The option of all ceramic ceramic crowns for case 2 was ruled out as the patient had deep bite. She was also suggested for crown lengthening and gingival recon touring surgery for better smile, but refused and wanted acceptable smile with minimum intervention .Endodontic treatment was planned and executed for all the maxillary incisors (Fig 4a & 4b). Then for case 1 these incisors were prepared with deep chamfer finish lines with rounded internal angles to receive all ceramic crowns (Fig 5a). For case2 after endodontics the remaining carious portion of teeth was removed and then restored with composite resin. Crown preparation was done and modified keeping in mind to achieve as far as possible to achieve aesthetic location (Fig 5b). Maxillary impressions were then made in single step double mix technique using addition type poly vinyl siloxane impression material.
 | Fig 4 A : Case 1 Post Endodontic Intra Oral Peri Apical Radiograph Of Tooth
|
 | Fig 4 B : Case 2 Post Endodontic Intra Oral Peri Apical Radiograph Of Tooth
|
 | Fig 5 A : Case 1 Crown Preparation With 11,12,21,22.
|
 | Fig 5 B : Case 2 Crown Preparation With 11,12,21,22.
|
Provisional crowns made of poly methyl meth acrylate were closely fabricated to the contours of diagnostic wax up were than delivered. Try in was done keeping in mind the mid line, occlusal plane Restorations were checked to avoid any occlusal interference and the intended results of treatment regarding the change in shape and dimensions of teeth were shown to the patients, following their approval of aesthetics, phonetics and function, all ceramic (lithium disilicate enforced glass ceramic) crowns were delivered & luted with Resin based luting agent (Fig 6a) for case1. Ceramo-metal crowns in relation to 11,12,21,22 were delivered and luted with type II glass ionomer cement (Fig 6b) for case 2. Both the patients were satisfied and happy with their aesthetic new smile, excellent view of the anterior teeth (Fig 7a &7b). They were given necessary instructions regarding follow up visits and how to maintain the crowns and oral hygiene.
 | Fig 6 A : Case 1 Intra Oral Post Operative (After Treatment)
|
 | Fig 6 B : Case 2 Intra Oral Post Operative (After Treatment)
|
 | Fig 7 A : Case 1 Smile View (After Treatment)
|
 | Fig 7 B : Case 2 Smile View (After Treatment)
|
Discussion
The provision of dental care should be based on the ability to benefit an individual patient [1]. The benefits of dental treatment must, therefore, be balanced against their associated risks and costs in order to safeguard individuals from procedures and interventions which may be of little benefit, or even harmful, and to avoid wasting limited financial resources [2]. An increased inflow of adult patients has been witnessed in orthodontic practice during recent times. Adult orthodontics requires a different approach to the treatment than treatment for growing adolescent individuals due to varied reasons. Lack of growth potential makes growth modification procedures not applicable to adults and imposes limitations to certain tooth movements [3].The potential for orthodontic relapse has inspired the use of tooth preparation and restorative dentistry to recreate tooth dimensions and proportions commensurate with prosthodontic results from both n aesthetic and functional clinical outcome, thereby eliminating the potential for relapse and the need for forced orthodontic tooth movement [4]. The restorative treatment options available for enhancing smile and function rapidly include aesthetic contouring, bonding, porcelain laminates, and crown. A well planned and executed diagnostic wax up is an essential communication tool for both he patient and the laboratory [5]. For determining whether the restorative treatment could adequately camouflage the patient’s expectation for the end result.
The ability to reposition the crown into an ideal aesthetic location can more easily be accomplished when the tooth has been treated with root canal. Apart from this universally accepted indication, elective (intentional) RCT of teeth with normal pulps may become necessary. In1961, Bohannan and Abram’s,[6] first described this treatment as a component of an interdisciplinary oral rehabilitation of mal-aligned periodontally affected teeth with vital pulps, and summed up this procedure by saying that “no tooth or part of a tooth should be regarded as sacred if the prognosis of the remaining dentition is improved by its sacrifice”. The literature shows that elective / intentional RCT, whenever indicated, refers to RCT of a normal pulp, [7] a doubtful pulp prior to restorative procedures [8]. The other options of ceramic or composite laminates but they have limited indications like may be used for minor correction and favourable occlusal scheme and are not so permanent in nature. The composite laminates specially have low fracture resistance, and not being as durable as ceramics in dynamic environment like oral cavity. In such instances like in the above 2 cases jacket crowns are the viable options for long term results. It may be necessary to perform a crown lengthening procedure prior to aesthetic restoration of these teeth but in our case 1 the patients lip line hided the gingival discrepancy. These cases through the use of PFM and All Ceramic crowns signify the use of modern aesthetic and restorative techniques and materials with aesthetically pleasing appearance.
Conclusion
When age and time are primary concern for patients to enhance their appearance, the restorative space management regime can be used for long term acceptable aesthetic and functional results, making the patients aware of the limitations and explaining orthodontic option first and all other probable options.
References
1. Pine C, Harris R ,Sheiham A, Tsakos G. Oral health needs assessments. Community Oral Health. New Malden: Quintessence Publishing Co. Limited. 2007: 59-79.
2. Shaw WC, O Brien KD, Richmond S, Brook P. Quality control in orthodontics: risk/benefit considerations. British Dental Journal.1991; 170:33-37.
3. Vanarsdall RL, Musich DR.: Adult orthodontics: Diagnosis and treatment. Current principles and techniques. 4th edition, StLouis. Mosby: 2005
4. Gruel G: Predictable, precise, and repeatable tooth preparation for porcelain laminates veneers. Pract Proced Aesthet Dent 2003; 15(1):17-24
5. Small BA: Laboratory communications for aesthetic success. Gen Dent 1998; 46:566-8,572-4.
6. Bohannan HM, Abram’s L: Intentional vital pulp extirpation in periodontal prosthesis. J Prosthet Dent 1961; 11:781–789.
7. Livaditis GJ: Vital pulp therapy with bipolar electro coagulation after intentional pulp exposure of fixed prosthodontic abutments: a clinical report. J Prosthet Dent.2001; 86:400–406.
8. European Society of Endodontology (ESE): Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J 2006; 39:921–930.
|