Introduction:
Preservation of dental arch and its function is one of the main objectives of Pediatric dentistry. Premature loss of deciduous & young permanent teeth may lead to mesial drifting of permanent teeth and consequent malocclusion and/or collapse of dental arches. As far as possible the pulpally involved tooth should be maintained in the dental arch if it can be made free of disease and restored to function.
Perforations represent pathologic or iatrogenic communications between the root canal space and the attachment apparatus. The causes of perforations are resorptive defects, caries or iatrogenic events that occur during and after endodontic treatment regardless of the cause. Perforation of the pulpal floor in multirooted deciduous teeth incites inflammation, which predisposes a tooth to periradicular breakdown and eventual loss of periodontal attachment, which in most instances is irreparable and frequently leads to loss of the tooth. Immediate repair of these perforations is recommended. Ingle et al reported that perforations were the second greatest cause of endodontic failure & accounted for 9.6% of all unsuccessful cases.[1] Many different materials have been used to repair these defects but none of them fulfill the criteria of an ideal repair material that includes sealability, biocompatibility & ability to induce Osteogenesis & Cementogenesis. In addition to providing a good seal, the material of choice for repair of root perforation must be biocompatible, radio-opaque, non toxic, non-absorbable, bacteriostatic, fungicidal, insoluble in the presence of tissue fluid and capable of promoting regeneration of periradicular tissues.
Mineral trioxide aggregate (MTA) was developed at the Loma Linda University, California, USA and introduced to Endodontic by Torabinejad et al in 1993 and has been used successfully in the repair of lateral root perforations and furcal perforations.[2] MTA powder consists of fine hydrophilic particles and has initial pH of 10.2 and final pH of 12.5 with 40 MPA compressive strength. The diverse application of MTA in the practice of pediatric dentistry is evident in its use as an apical-barrier in immature non-vital teeth & in the coronal fragment of fractured roots as a pulpotomy medicament in primary & permanent teeth, as well as a pulp-capping agent in young permanent teeth.
The diffusion of ions is important for periapical healing. The high pH of Calcium Hydroxide reduces the number of bacteria and acts on the inflammatory process as a local buffer. Ca++ is necessary for the immunological reaction of the complement system, to reduce local inflammation and initiate the remineralization process. When treating an infected tooth with a periradicular lesion, the idea would be to use a root canal dressing containing all properties present in Calcium Hydroxide, with fast ion dispersion in the form of thickened paste or associated with Iodoform (VITAPEX), which contains additional antiseptic properties.
Therefore the aim of this study was the comparative evaluation of Mineral Trioxide Aggregate (MTA) & Calcium Hydroxide/Iodoform paste (VITAPEX) as a reparative agent in furcation involvement of deciduous teeth evidenced clinically & radiographically.
Materials and Method:
Round Bar (Small)
Barbed Broaches
H-file Packets No. 10 & No. 15-40.
MTA – Angelus (Fig. 2)
VITAPEX - Calcium Hydroxide / Iodoform Paste (Fig.2)
MTA Carrier (dovgan) - straight or Flexible tip or messing gun. (Fig.1)
Condenser
Micro ball Burnishers & pluggers
 |
 |
 |
|
 |
|
The sample for this study was drawn from patients who reported to the Department of Pedodontics & Preventive Dentistry, Santosh Dental College & Hospitals, Ghaziabad, seeking dental treatment. Twenty pediatric patients with furcal involvement were taken up. The patients were randomly and equally divided into two groups. Each group were treated with MTA (Angelus) and VITAPEX respectively. All cases were evaluated clinically to determine the presence or absence of inflammation, sinus & mobility at zero, three & six months. Radiographic evaluation was also carried out to check severity of radiolucency at same time interval.
Patients with furcally involved deciduous teeth were taken up. Site was then dried with fine air syringe. Mixing of MTA is imperative should be prepared immediately before its use. MTA powder must be kept in airtight containers to prevent moisture contamination. The powder should be mixed with sterile water at a ratio of 3:1 on a glass slab with an aid of plastic or metal carrier to its intended site of operation. A small amount of liquid and powder were mixed to putty consistency because the MTA mixture is a loose granular aggregate and it does not stick very well to itself or to any instrument. MTS was carried to the cavity using specially designed carrier i.e. Dovgan carrier or Messing gun. Once the MTA was placed into the retro preparation, microball burnishers and micro pluggers were used to gently compact it. A small damp cotton pellet was used to gently clean the resected surface and to remove any excess MTA from the cavity. In case of Vitapex, mixing is not required since it comes in syringe form with the plastic lid covering the tip of the syringe. Site was dried with fine air syringe and is placed just over the site. Piston was gently pushed, placing the medicament over the site. A small damp cotton pellet was used to gently compact and clean the resected surface and to remove the excess Vitapex from the cavity.
Result:
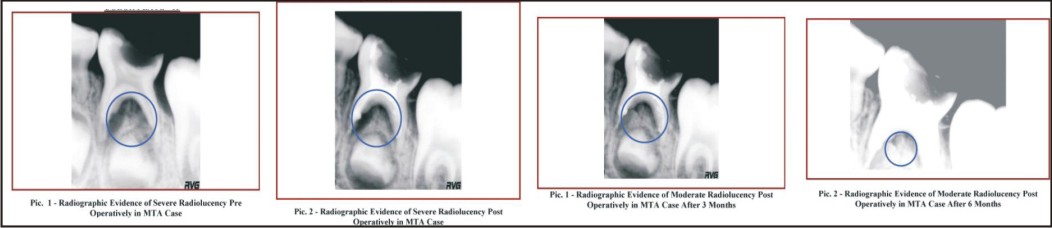
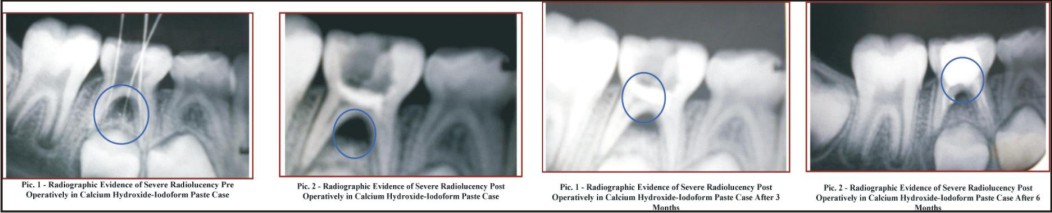
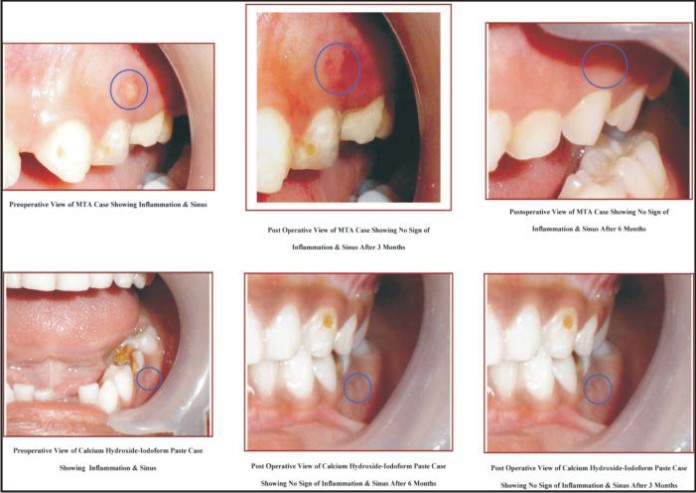
Amongst all repaired perforations, 30% of the Vitapex cases after six months of clinical & radiographic follow up were associated with inflammation, whereas sinus and mobility were clinically not observed. Whereas in case of MTA inflammation was not noticed after months. Furthermore, nine non-inflamed MTA cases had shown marked improvement in terms of radiolucency.
Discussion:
The primary goal of repairing the furcally involved deciduous teeth is to maintain the integrity and optimal health of oral tissues by keeping the two things in mind i.e. to maintain arch length and tooth space, to allow a tooth to remain in the oral cavity in a non-pathological state, to restore a tooth to its functionally efficient form and to maintain the child's esthetics and thereby prevent any psychological trauma.
There are various studies available in the literature in which MTA has shown significantly less dye penetration as compared to other materials. This material is composed mainly of mineral oxides, which react with water to set. Because of its hydrophilic characteristics, moisture of the surrounding tissue acts as an activator of the chemical reaction of this material. M Torabinejad and TR Pittford have supported the opinion that MTA is superior to Vitapex, since only one of a large number of experimental studies into furcal perforation has reported the presence of new cementum formed against the repair material with mixture of Calcium Hydroxide – Iodoform paste (VITAPEX).[3],[4] In our study, we attempted to compare clinically & radiographically, use of MTA and VITAPEX for repair of furcal perforation after three and six months follow up. All cases of VITAPEX showed inflammation but no sinus & mobility was seen after six months. Whereas MTA showed complete absence of inflammation also in addition to sinus and mobility, after six months. So this supports the Torabinejad study, which concluded that MTA is a far more suitable material for perforation repair.[5] Sluyk SR et al (1998) observed the evaluation of setting properties and retention characteristics of MTA when used as a furcation perforation repair material.[6] They observed that the presence of some moisture in the perforation during placement was advantages in aiding adaptation of MTA to the walls of the perforation. Same is not the case with VITAPEX, as seen and observed in our study. This may be because of the non-setting nature of the material, difficult to pack and its known caustic effect on vital tissue.
Craig M et al (2004) evaluated success rate of root perforation repairs using MTA. Pretreatment, immediate past treatment and at least one year follow up radiographs were evaluated in a double blind manner to determine the presence or absence of any pathologic changes adjacent to perforation sites.[7] Results of MTA in our study was to an extent similar to result of this study, as all MTA repaired cases demonstrated normal tissue architecture adjacent to the repair site at the recall visit. Teeth with existing lesion showed resolution of the lesion and teeth without preoperative lesions continued to demonstrate absence of lesion formation at the follow up visit.
What this paper ads-
• This paper provides a synopsis of the key comparison of MTA and VITAPEX as reparative agent in furcation involvement in deciduous teeth.
• This study reviews the evidence on the effectiveness of MTA when compared with VITAPEX.
• Better and clearer clinical & radiographic picture was postulated by this study.
Why this paper is important to pediatric dentists-
• This study provides readers especially pediatric dentist vital information on a relatively new restorative material which comes into direct contact with connective tissues (peri-apical tissues).
• This study will surely elevate hesitation of using a relatively new material amongst pediatric dentist and will certainly boost confidence in terms of global concern i.e. cost, handling characteristics and its success rate.
• This study will certainly help scientifically & clinically; pediatric dentist to use MTA in repair of furcal perforation.
Conclusion
Ten deciduous teeth with furcal perforation were repaired with MTA and Calcium Hydroxide- Iodoform Paste respectively in order to evaluate them clinically and radio graphically at three and six month’s interval.
Clinically, they are evaluated for presence and absence of inhalation, sinus and mobility at zero month, three months, six months. Similarly, radiographic evaluation was done by grading radiolucency into severe, moderate and absent at zero month, at three month and at six months.
Based on the outcome of the cases presented on this study, clinically after six months follow up, MTA has shown favorable response when compared with Calcium Hydroxide- Iodoform paste. Radiographically, moderate radiolucency was seen in all the cases treated with MTA but reduced after six months whereas 40% cases have shown severe radiolucency and 60% cases have shown moderate radiolucency in case of Calcium Hydroxide-Iodoform paste.
Long- term prognosis is still not certain and warrants observation for longer periods. Overall, MTA allowed a considerably more favorable response than Calcium Hydroxide-Iodoform paste.
References
1. TT Nakata,KS Bae,JC Baumgartner.Perforation repair comparing mineral trioxide aggregate and amalgam. Journal of Endodontics 1997 Apr; 23(40:259
2. Seung Jong Lee,Mehdi Monset,Toarabinejad M.Sealing ability of mineral trioxide aggregate for repair of lateral rootperforation.Journal of Endodontics 1993 Nov;19(11):541-544
3. TR Pitt Ford,M Torabinejad,CU Hong,SP Karivawasam.Assessment of Mineral Trrioxide aggregate as a retrograde root filling.Journal of Dental Research 1994;73(4):804
4. Torabinejad M, Chivan N. Clinical applications of mineral trioxide aggregate. Journal of Endodontics 1999;25(3):197-205.
5. Arens DE and M Torabinejad.Repair of furcal perforations with mineral trioxide aggregate: Two case report.Oral Surgery,Oral Medicine,Oral Pathology Oral RadiologyEndodontics 1996;82(1):84-88.
6. SR Sluyk,PC Moon,GR Hartwell.Evaluation of setting properties and retention characterestics of mineral trioxide aggregates when used as a furcation perforation repair material. Journal of Endodontics.1998 Nov;24(11):768-71.
7. Craig Main, Nina Mirzayan, Shahrokh Shabahang, Mahamoud Torabinejad.Repair of root perforations using mineral trioxide aggregate: a long term study. Journal of Endodontics 2004 Feb;30(2):80-83.
|