|
|
|
| Knowledge, Behaviour And Attitude Towards Oral Health In Population Of Sunam Town |
Harjit Kaur 1 , Sanjeev Jain 2 , Amandeep Kaur 3 , Sumit Kochhar 4 , Divya Saxena 5 , Gaurav Pandav 6
1 Professor And Head , Dept. of Periodontology - GNDDC, Sunam
2 Professor , Dept. of Periodontology - GNDDC, Sunam
3 P.G. Student , Dept. of Periodontology - GNDDC, Sunam
4 Sr.Lecturer , Dept. of Periodontology - GNDDC, Sunam
5 Sr.Lecturer , Dept. of Periodontology - GNDDC, Sunam
6 Sr.Lecturer , Dept. of Periodontology - GNDDC, Sunam
|
| Address For Correspondence |
Dr. Harjit Kaur
Professor And Head
Dept. of Periodontology
G.N.D.D.C. SUNAM |
| Abstract |
| Abstract : To maintain good oral health effective preventive measures are necessary and to establish efficient methods for self prevention one must have good knowledge and a positive attitude towards oral self-care.
Aim : The aim of the study was to assess dental knowledge, behaviour and attitude of general population towards oral health.
Materials and method : The questionnaires were administered to the total of 681 subjects. The questionnaire obtained information on age, gender, oral self care, knowledge of preventive dental care and attitude towards preventive dentistry.
Results : The mean percentage score for oral health knowledge, attitude and behavior were significantly higher in females than males (p-value 0.0001). Also, highly significant difference was found in the knowledge, attitude and behavior between subjects with age between 18- 35 years and subjects with the age between 36-60 years.
Conclusion : It may be concluded that gender plays a role in the perception of oral health, use of toothbrush and other interdental cleansing aids and dental visits as females were more particular about their oral health maintenance and have more positive dental health attitude and behaviour than males. Likewise, younger subjects are more concerned about their oral health than the older subjects. |
|
| Keywords |
| Attitude, knowledge, behaviour, oral health, questionnaire. |
|
| Full Text |
Introduction
Health is one of the most valuable assets one can possess. It is defined by the World Health Organization as a state of complete physical, mental and social well being and not merely the absence of disease or infirmity[11]. Oral health may be defined as a standard of health of the oral and related tissues which enables an individual to eat, speak and socialize without active disease, discomfort or embarrassment and which contributes to general well being. Oral diseases can be considered a public health problem due their high prevalence and significant social impact[11].
In the prevention of oral diseases, much emphasis has been placed on factors such as knowledge, attitude, beliefs and emotions and the way these may be subjected to behaviour modification techniques. Knowledge as defined by ‘Oxford dictionary’ is the ‘expertise and skills acquired by a person through experience or education’. The term knowledge is also used to mean the confident understanding (theoretical or practical) of a subject with the ability to use it for a specific purpose. An attitude is a relatively enduring organization of beliefs around an object, subject or concept which pre-disposes one to respond in some preferential manner. It is an acquired characteristic of an individual. People demonstrate a wide variety of attitudes towards teeth, dental care and dentists. These attitudes reflect their own experiences, cultural perceptions, familial beliefs and other life situations and they strongly influence the oral health behaviour. Health behaviour as defined by Steptoe A et al (1994)is ‘the activities undertaken by people in order to protect, promote or maintain health and to prevent disease[10].Oral health behaviour consists of individual and professional care, and includes toothbrushing, dental flossing, visiting a dentist and following a proper diet. Biology, environment, lifestyle, health care organizations and psychological factors are essential components of oral health behaviour[8]. Oral diseases adversely affect concentration and productivity due to intricate relationship between oral health and general health. Prevention of oral diseases can be achieved by optimal oral health practices which include tooth brushing, flossing, dental visits and proper diet[1]. For prevention it is important that there is improvement in the knowledge of the community, a promotion oforal health behaviour and a positive attitude towards self –care preventive methods.A proper knowledge about frequency, duration and technique of tooth brushing and flossing, a positive attitude towards professional dental care and zeal to maintain a good oral hygiene is required for the prevention and treatment of oral diseases[9].
Knowledge brings changes in the behavior and attitude of an individual. Though studies have been carried out regarding the oral health knowledge, attitude and behavior among different student populations, some educated classes and urban populations but literature is scarce about rural Indian population who constitute about 70% of the population. So this study was conducted to assessknowledge, behaviour and attitude of general rural population of Sunam towards oral health.
Materials & Method
This cross-sectional study was conducted in the rural population of Sunam. The study subjects were recruited from the villages. The study sample comprised of 681 subjects including males 336 (49.34%) and females345 (50.66%). The study sample was also divided on the basis of age with subjects between 18-35 years of age 333 (48.90%) and 36-60 years of age 348 (51.10%). All subjects were above 18 years of age, so that they can easily understand and answer the questionnaire.
The purpose of the study was informed and explained to the participants. A self assessment questionnaire was used as a survey instrument for this study. The questionnaire was designed to evaluate the oral health knowledge, attitude and behavior among all the participants which included three questions to check oral health knowledge, eight to know attitude and nine for behavior.
Assessment of participant´s oral health knowledge included items on the knowledge about the use of interdental brush and floss and the knowledge about harmful effects of smoking.
Assessment of participant´s dental attitude included questions regarding regular visit to a dentist is necessary, attitudes towards health care in general and oral care in particular.
Assessment of participant’s oral health behavior included brushing habits (such as frequency, duration and time), reason for visiting a dentist and adverse habits.
Data Analysis
Categorical variables were presented as percentages. Pearson χ2 test was used for analysis of categorical variables. A P value of <0.05 was considered to indicate statistical significance. All calculations were performed using SPSS® version 17 (Statistical Packages for the Social Sciences, Chicago, IL). All tests were two sided.
Results
The total study population was 681, comprising 345 (50.66%) females and 336 (49.34%) males. The population between 18-35 years of age was 333 (48.90%) and between 36-60 yearswas 348 (51.10%) (Table - 1). The gender difference and the age difference was assessed using Chi-square statistics and a highly significant (p-value 0.0001) difference was found. Results showed that a significant difference (p- value < 0.0001) was found in the dental health knowledge scores of females and males, also between the two age groups as shown in (Table - 2). Similarly a significant difference (p- value < 0.0001) was found in both attitude and behavior scores of different gender and the age groups (Table-3 and Table-4).
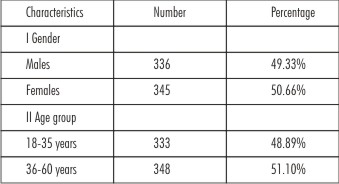 | Table 1 – Demographic Characteristics Of The Subjects
 |
 | Table 2 – Showing Knowledge Scores According To Gender And Age
|
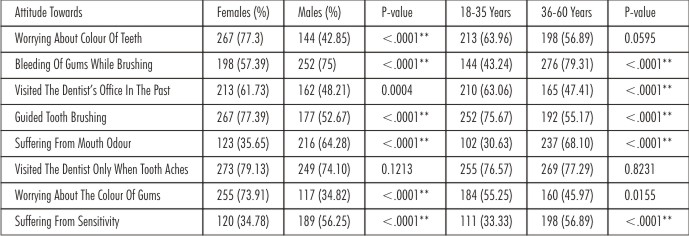 | Table 3 – Showing Attitude Scores According To Gender And Age
|
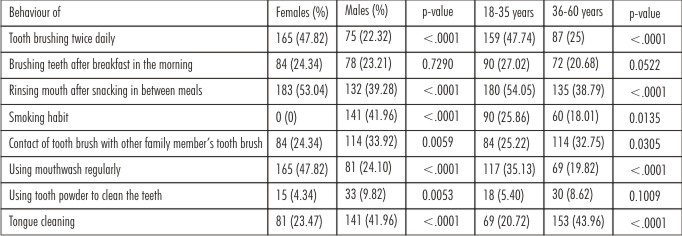 | Table 4 – Showing Behaviour Scores According To Gender And Age
|
Discussion
A dental health questionnaire focused on knowledge, attitude and behaviour concerning periodontal health was conducted among the rural population. The limitation of this study was that it was a self reported data. The questions were framed in very simple language. There is a strong relationship between dental health behaviour and periodontal disease.Lissau I et al (1990) observed that dental health behaviour in children and in adulthood were responsible for between 10 and 14% of the variance in level of periodontal disease indicator[5]. Asinferenced from the results, it is seen that age and gender both has an effect on oral health behaviour. The women and the young people are more conscious about their oral health as well as aesthetics than males and older people. Dental aesthetics is a topic of concern among all the people of the country and it is evident from our study that females and young people are more concerned about the colour oftheir teeth and gums than the males and old people. This condition may be explained on the basis that females and the younger people usually care more about their body and appearance (Table - 2). They would thus be more concerned about visiting the dentist and would tend to be more educated about their oral health[6]. Also they are more particular in following the dentist´s instructions in carrying out oral hygiene measures such as tooth brushing technique (frequency, duration and method), using interdental cleansing aids and use of mouth wash (Table - 4).The gender gap in oral health may have some genetic, hormonal and cultural influences.
Health belief theory (Eiser 1997) suggests that dental healthbeliefs should be associated with dental health behaviours. This implies that changing beliefs should result in changes in behaviour and attitudes. Broadbent JM et al (2006) investigated whether individuals who hold favourable oral health related beliefs over time have better adult oral health than who do not and found that unfavourable dental health beliefs are related to poorer health[2]. It resulted in increased risk of gingivitis, high plaque scores and tooth loss due to caries. A strong association between gender and oral health beliefs (and their stability was identified, with fewer males than females endorsing favourable dental beliefs. The present study also supports these findings.
Visiting the dentist for routine check up is defined as “preventive care use”. The preventive care behaviour in the females and younger age group people was better as compared to males and older age group people. For preventing periodontal disease it is important to focus on young people[7]. Regarding the visit to the dentist 61.73% of the females reported in affirmativewhile in males 48.21% said yes. Similar results were observed in both age groups which were 63.06% in younger age group and 47.41% in older age group. As the population is basically rural, the education level is poor and the major reason for visiting the dentist is pain in all the groups (Table - 3). The results indicated that though the subjects knew about the effects of poor oral hygiene but the knowledge about floss, tooth brushing technique, use of interdental cleansing aids and tongue cleaning needs to be improved (Table - 2). For developing this behaviour and attitude more motivational programmes should be included in dental health care of the population under study[3]. The results show that women are more particular about the toothbrushing frequency than men. Similar results were found in the studies byAl- Omari QD et al (2005)andKhami MR et al (2007) where women reported significantly higher frequencies of tooth brushing (P < 0.001), as compared with men.These findings were different from the findings in a study by Tseveenjav B et al (2003) who found no differences in the tooth-brushing frequency between male and female Mongolian dental students. As knowledge, attitude and behaviour of males and the older age group was poor as compared to females and younger age group they had poor dental health and suffered from bleeding on probing and halitosis than the other groups.
Though the relationship between dental health beliefs and behaviour has been established, however there was significant difference in oral health knowledge and behaviour in this study. The findings suggested that though males and younger age group people had more knowledge of effects of smoking, inspite of that more percentage of these groups had the habit of smoking (Table - 2 and Table - 4). The more percentage of younger age group had the habit of smoking, the reason behind this may be the factors like influence of the friends (peer pressure) or the other family members, economic status, family values and education level. Similar observations were reported bySharda AJ and Shetty S (2008) in a study conducted among dental students. They observed that there were positive changes in the oral health knowledge of the students from first year to fourth year but it was not changed into oral health behaviour and preventive behaviour among the students has to be improved so that the dental students, as future dental health providers, can set an example for their patients, family and friends by maintaining good oral health in their own mouth and advice the community about good oral health behaviours with conviction[10]. Folayan MO et al (2013) from their study among Nigerian students concluded that good knowledge of preventive dental care does not seem to be an equally appreciable impact on their oral health behaviour with less than a third of them practicing recommended self care measures[4].
Conclusion
The oral health knowledge, attitude and behaviour of this rural population was not very positive for which the reason may be the lower literacy rate. It was observed from the study that, females and young people were more particular about their oral health maintenance and has more positive dental health attitude and behaviour than males and older people respectively. It appears that, knowledge, attitude and behaviour among males and the older group people need to be improved. Oral health beliefs affect oral health outcomes. Thus, intervention of favourable oral health beliefsespecially in young minds may be a valid means of improving oral health outcomes.
References
1. Azodo CC andUnamatokpa B. Gender differences in oral health perception and practices among medical house officers. Stomatology. 2012;1
2. Broadbent JM, Thomson WM, Poulton R. Oral health beliefs in adolescence and oral health in young adulthood. J Dent Res. 2006;85(4):339-43.
3. Farsi JMA, Farghaly MM, Farsi N.Oral health knowledge, attitude and behaviour among Saudi school students in Jeddah city. Journal of dentistry.2004;32:47-53.
4. Folayan MO, Khami MR, Folaranmi N, Popoola BO, Safola OO, Ligali TO, Esan AO, Orenuga OO. Determinants of preventive oral health behaviour among senior dental students in Nigeria. BMC Oral Health. 2013;13(28).
5. Lissau I, Holst D, feiis-Hasche E. Dental health behaviours and periodontal disease indicators in Danish Youth: a 10 year epidemiological follow up. J ClinPeriodontol 1990;17:42-47.
6. MacEntee Ml, Stolar E, Glick N.Influence of age and gender on oralhealth and related behaviour in anindependent eideriy population. Community Dent Oral Hpidemiol 1993; 21: 23
7. Mizutani S, Ekuni D, Furuta M, Tomofuji T, Irie K, Azuma T, Kojima A, Nagase J, Iwasaki Y, Morita M.Effects of self-efficacy on oralhealth behaviours and gingivalhealth in university studentsaged 18- or 19-years-old. J ClinPeriodontol 2012; 39:844–849.
8. Neamatollahi H, Ebrahimi M, Talebi M, Ardabili MH and Kondori K.Major differences in oral health knowledge and behaviour in a group of Iranian pre-university students:a cross-sectional study. Journal of Oral Science, Vol. 53, No. 2, 177-184, 2011
9. Neerajaa R, Kayalvizhia G, Sangeethaa P. Oral Health Attitudes and Behavior among a Group of Dental Students in Bangalore, India. Eur J Dent 2011;5:163-167.
10. Sharda AJ andShetty S. A comparative study of oral health knowledge, attitude and behaviour of first and final year dental students of Udaipur City, Rajasthan. J Oral Health Comm Dent.2008;2(3):46-54.
11. Singh K, Kochhar S, Mittal V, Agarwal A, Chaudhary H, Anandani C.Oral health: knowledge, attitude and behaviour among Indian population. Educational research 2012: vol 3(1);066-071.
|
|
|
|
|
|
|