Introduction
The achievement of a stable, functional and esthetic arch form has long been one of the prime objectives of orthodontics. A key aspect in the achievement of this goal is the identification of a suitable arch form to use in the treatment of each case. Many clinicians tend to adapt one particular arch form for the treatment of all malocclusions. The arch form chosen is often the one that creates, in the orthodontist’s opinion, the optimum esthetic and functional occlusion.
For more than 100 years, researchers have been trying to define the “ideal” arch form, frequently using the concept that the dental arch is symmetric in nature and can be represented by an algebraic or geometric formula.
It is commonly believed that the dental arch form is initially shaped by the configuration of the supporting bone, and following eruption of teeth, by the circumoral musculature and intraoral muscular forces[5].
Bonwill and Hawley (Tweed 1966)[26] described the alignment of the upper anterior teeth as a circumference arch, whilst MacConill and Scher (1949) maintained that the dental arch looked like a catenary curve[18]. Izard (1927), in trying to relate the dimension of dental arch to the facial dimensions, found that the arch form could be accurately represented by an elliptical curve[14].
Currier (1969) found that the curve of the incisal edge of incisors and canines, together with the buccal cusps of premolars and molars, could be expressed as an ellipse in both arches[9]. Brader (1972), on the other hand maintained that the teeth were arranged in formation as in the constricted end of a trifocal ellipse[5].
BeGole and Lyew (1998) developed a method, using cubic spline function, to analyse change in dental arch form pre- and post-treatment and post-retention[3].
The size and form of dental arches exhibit considerable variability within and among human groups. Determinants of arch size and shape are not well understood.
While it is obvious that the orthodontist treats the individual and not some abstraction of population, it also holds that people from different ethnic groups present with different conditions, the clinician should anticipate the differences in size and form rather than treating all cases to a single ideal.
A number of investigators[7], [8]have noticed that variation in arch forms in different ethnic groups and have observed that normal measurements of one ethnic group should not be considered normal for other ethnic groups. Different ethnic groups must be treated according to their own individual characteristics.
Therefore in orthodontics an individualization of treatment leads to more effective treatment by working within the patient’s natural arch form instead of making patients fit a single standard.
In the present study an attempt is made to evaluate the nature of arch form in a sample of south Indian population so as to individualize protocols for better results.
Materials And Method
Source of Data
Full mouth dental casts of 60 subjects (30 males and 30 females) between ages 17 – 25 years were obtained.
Method of collection of data
Selection Criteria
The following selection criteria were followed:
1. Patients belonging to local population
2. Patients with full complement of natural teeth. (With possible exception of third molars)
3. A bilateral class I canine and molar occlusion.
4. No history of orthodontic treatment.
5. No arch asymmetry
6. Crowding not > 3mm in either arch.
7. Absence of extensive restorations, cast restorations or cuspal coverage.
8. Absence of pathologic periodontal conditions.
Method
Digitization Of Arches
Eighteen buccal cusp tips and mid-incisal edge points were marked on each maxillary and mandibular cast. (Figure: 1) Each cast was photocopied (1:1 print) at 1X by placing the occlusal surface down on a photocopier in its photographic mode.
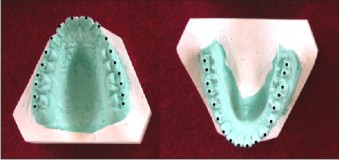 | Figure 1
 |
A millimetric scale was included in the each print to guard against magnification. A cardboard mask cover was used to cover the active surface of the photocopier. The photocopies were scanned using scanner and a digital image of occlusal surface of each cast was prepared.
All the digital images were transferred to computer software and the co-ordinates of mid-incisal edges and buccal cusp tips of all teeth were determined.
The original XY co-ordinates on the digitiser were corrected for magnification and adjusted to establish new XY co-ordinates in such a way that the mean inclination of the straight line connecting the right and left second molar cusp tips became parallel to original
X – Axis thus obtaining a common reference system for all dental arches independent of the orientation used for arch digitisation.
Single operator performed Tracing and digitisation of cusps.
Arch Interpolation
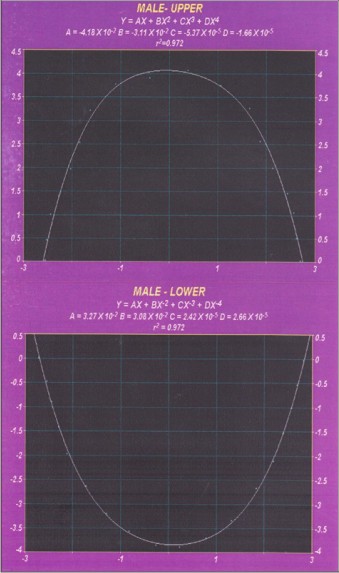
The X and Y co-ordinates of the mid-incisal edges and cusp tips in each arch were transferred to Table Curve 2D v5.01 Software (SYSTAT Software Inc.). Maxillary and mandibular arches were interpolated using fourth order Polynomial;
Y=AX + BX2 + CX3 + DX4
Of note, each of the four weighting co-efficients in the equation is interpretable in terms of an arch’s form, namely its left-right asymmetry (terms A and C) and its taperedness (B) and squareness (D).
The least square correlation co-efficient was calculated for each arch form.
Statistical comparisons were performed between mean co-efficients computed in male and female samples in maxillary and mandibular arches using two-tailed student’s t-test. A difference was considered to be significant if p £0.05. Mean co-efficients of each curve was used to draw male and female mean curves.
Arch Dimensions
Arch widths and depths were computer generated as straight-line distances between the dental landmarks. (Figure 2).
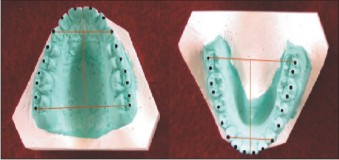 | Figure 2
|
The depths and widths were defined as follows:
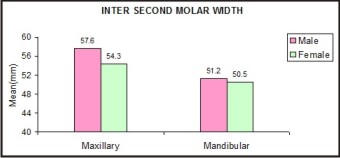
1. Inter-second molar width (Wm): Distance between the distobuccal cusp tips of second molars.
2. Inter-canine width (Wc): Distance between the canine cusp tips.
3. Second molar depth (Dm): Distance the contact of central incisors and the line that connects the distobuccal cusp tips of the second molars.
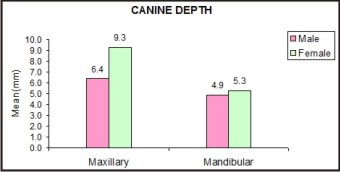
4. Canine depth (Dc): Distance between the contact of central incisors and a line that connects the canine cusp tips.
Results
Determination Of Mathematical Model
Means and standard deviations of the co-efficients of the fourth order polynomial are reported in TABLE NO.I along with their least square correlation co-efficients. The polynomial model accurately interpolated the data points in all the instances i.e., all mean correlation co-efficients were larger than 0.95. (r=1.0 for a perfect fit)
Comparison of polynomial co-efficients between males and females yielded significant differences in the maxillary arch as shown by the mean values of second (B), third (C) and fourth (D) degree co-efficients of the maxillary arch in TABLE NO.II On the contrary no significant differences were found in the mandibular arch.
Figures 3 and 4 shows the mean maxillary and mandibular arches in the males and females determined using the fourth order polynomial (Graph 1 - 4).
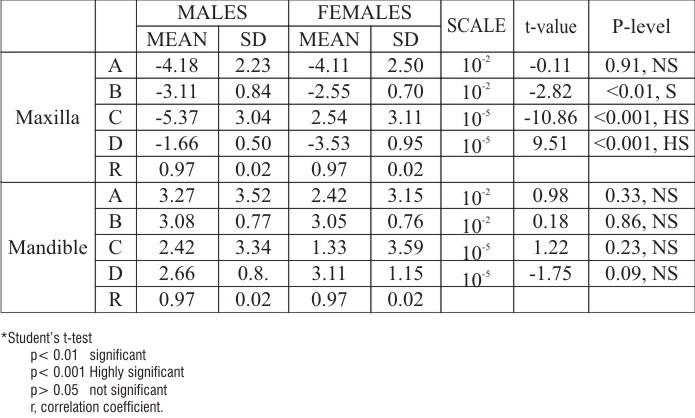 | Table No.I Fourth Order Polynomial – Mean Coefficients
|
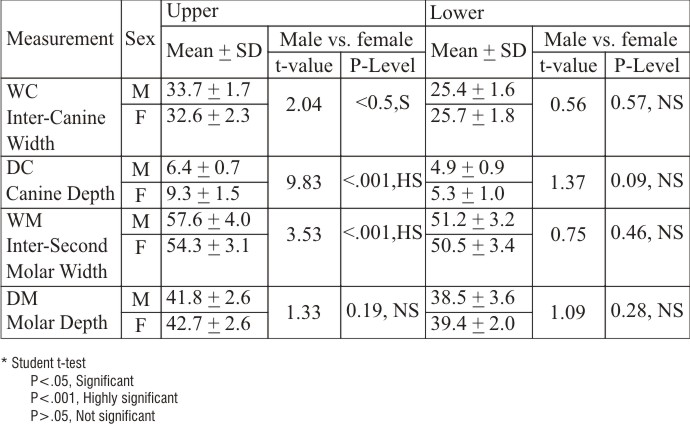 | Table No.II Comparison Of Canine Width, Canine Depth, Molar Width And Molar
|
 | Figure 3
|
 | Figure 4
|
 | Comparision Of Inter Canine Widths Of Males And Females
|
 | Comparision Of Canine Depths Of Males And Females
|
 | Comparision Of Inter Molar Widths Of Males And Females
|
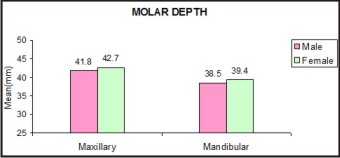 | Comparision Of Molar Depths Of Males And Females
|
Arch Dimensions
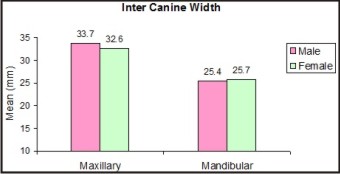
Comparison of arch dimensions between males and females showed that, the transverse measurements i.e., Wc and Wm were larger in male subjects as compared with those of females.(TABLE NO.II)
In the maxillary arch the inter-canine width and inter-second molar width were significantly larger in males as compared with that of females. However no significant differences were found in the mandibular arch. Also in the maxillary arch the canine depth was significantly more in females as compared with that of males. While in the mandibular arch there was no significant difference.
Discussion
Since Angle, orthodontists have tried to determine a single ideal arch form that can ensure the stability of therapeutic results. While it is obvious that orthodontist treats the individual and not some abstraction of the population, it also holds to reason that people with different ethnic groups present with different conditions and the clinician should anticipate the differences in size and form rather than treating all cases to a single ideal. Hence the study was undertaken to evaluate the nature of arch form in a local population and to investigate sexual differences between male and female arch forms so as to individualize protocols for better results
Dental arches have been extensively classified both using simple qualitative description and more complex mathematical methods. Parabolas and ellipses were the first fitting curves to be proposed in dentistry (Stanton 1922 and Izard 1927)[14], [25]. The catenary curve was introduced in 1949 (Baluta and Lavelle 1987; Jones and Richmond 1989; Pepe 1975)[1], [15], [21], but neither its mathematical interpolation, nor its fit seems suitable in clinical situations. Sampson (1981) using conic sections defined and plotted the mean curves for a 14-year old population, as well as the curves’ ranges of variation[23]. From a statistical point of view, cubic spline curves offer good curve fitting with correlations often exceeding 0.98 (Pepe 1975; BeGole 1980)[2], [21] but the curves do not have an immediate geometrical significance. The practical clinical application of these analyses seemed difficult. Braun et al (1998) described the use of Beta function to interpolate the dental arches[6]. Recently Velanzuela A.P. et al (2002) desribed the human superior dental arch form using Fourier transformation[27].
In the present study fourth order polynomial was used to interpolate the arch forms in a sample of south Indian population. This approach for the analysis of arch shape is not new, the dental and anthropological literature reported several curve fitting algorithms developed for this purpose.
It may be questioned that why this study did not deal with equations of greater degrees. One might assume that if fourth order polynomial is a good approximation, equations of greater degree should be even better. In theory this is quite true. Theoretically, there exists a unique polynomial equation of degree n+1 or less (where n is the number of data points) that will fit the data exactly. Such curves accurately fit the data points but they tend to be wavy rather than smooth. As ‘n’ increases, the likelihood of obtaining a completely accurate curve fit without this wave like property is reduced to nearly zero. Even if a smooth curve of high degree could be obtained, measurement errors and round-off error make such computations unwieldy, if not altogether impossible.
Previous investigations (Sampson 1981, BeGole 1980; Germane et al 1991) interpolated only the first 12 teeth (first molar to first molar)[2], [12], [23]. Only Richards et al (1990) also took the second molar into consideration using fourth order polynomial[22].
In the present study buccal cusp tips and mid-incisal points were interpolated taking into account all the 14 anterior most teeth (second molar to second molar).
The fourth order polynomial provided good curve fitting for the buccal cusps and mid-incisal points of maxillary and mandibular arches with the mean correlation co-efficients greater than 0.95 (r=1 for a perfect fit). This has been shown previously by Sampson (1981) in 14-year-old white Michigan children[23], Ferrario et al (1994, 1999) in a sample of white Caucasian population[11] and Burris et al (2000) in American black and white population[7].
In the present study the dental arches resulted in symmetry as shown by first (A) and third (C) degree co-efficients in table no.1. This was already reported by Sampson (1981) for a group of 14-year-old children[23], also by Ferrario et al (1994, 1999) in a sample of white Caucasian population[10], [11] and by Burris et al (2000) in a sample of American blacks and whites[7]. On the contrary, woo (1931) and Livshits and Koblyiansky (1991) have shown that various craniofacial complexes are characteristically larger on one side of the skull than other[17], [28].
The fourth order interpolation showed significant difference in the second (B), third (C) and fourth (D) degree co-efficients of maxillary arch between males and females indicating that the female mean curves were significantly smaller than male mean curves, especially in the maxillary arch. Mandibular mean curves showed no significant differences
Arch Dimensions
In most studies it was shown that the arch dimensions depend on the sex of the subjects, with smaller values in females (Staley et al 1985; Lavelle 1975)[16], [24]. In our study the mean arch dimensions showed significant differences in maxillary arch, with males showing larger inter-canine width and molar width than females, while in the mandibular arch no significant differences were found. Merz et al (1991) and Ferrario et al (1994) reported similar gender differences[10], [19].
In the present study the mean maxillary inter-canine widths in males was 33.7mm and in females it was 32.6mm. While the mandibular inter-canine widths in males was 25.4mm and in females it was 25.7mm.
Previous investigations on ethnic variations in oral and dental dimensions report conflicting results. No ethnic differences in arch size of 2 African groups were reported by Hassanali and Amwayi (1993)[13]. Conversely, Nummikoski et al (1988) found that arch widths as assessed by radiographic study, were larger in Mexican and black Americans than in white Americans. Significant sex differences were also demonstrated[20].
The results of this study indicate the need for different arch forms for males and females.
The fourth order interpolation showed significant difference in the second (B), third (C) and fourth (D) degree co-efficients of maxillary arch between males and females indicating that the female mean curves were significantly smaller than male mean curves, especially in the maxillary arch.
Comparison of arch dimensions between males and females showed that, the transverse measurements i.e., inter-canine width and inter-second molar width were larger in male subjects as compared with those of females.
In the maxillary arch the inter-canine width and inter-second molar width were significantly larger in males as compared with that of females. However no significant differences were found in the mandibular arch.
Conclusions
The results showed, the fourth order polynomial accurately interpolated the data points in all instances, the polynomial indicated that the arches were symmetrical and showed significant difference between the males and female dental arches particularly in the maxillary arch. The arch dimensions showed that males had significantly larger maxillary arch as compared to that of females. These results of the study emphasis a need to redefine the concept of the ideal arch with different arch forms for males and females.
Acknowledegments
The members of Department of Orthodontics and Dentofacial Orthopedics, College of Dental Sciences, Davangere, Prof. Anmol Kalha and Dr Amit Shaikh are thanked for their support and encouragement.
We the authors wish to confirm that there is no known conflict of interest associated with this publication and there has been no financial support for this work that could have influenced its outcome.
References
1. Baluta J. and Lavelle C.L.B. 1987:“An analysis of dental arch form" European Journal of Orthodontics. 9: 165-171.
2. BeGole E.A. 1980:“Application of the cubic spline function in the description of dental arch form". J Dent Res. 59: 1549-1556.
3. BeGole E.A. and Lyew R.C. 1998:“A new method of analyzing change in dental arch form" Am J Orthod Dentofac Orthop. 113: 394-401.
4. BeGole E.A., Fox D.L. and Sadowsky C. 1998:“Analysis of change in arch form with premolar expansion”. Am J Orthod Dentofac Orthop. 113: 307-315.
5. Brader A.C. 1972:“Dental arch form related with intra oral forces: PR=C”. Am J Orthod. 61: 541-561.
6. Braun S., Hnat W.P., Fender D.E. and Legan H.L. 1998:“The form of the human dental arch”. Angle Orthod. 68 (1): 29-36.
7. Burris B.G. and Harris E.F. 2001:“Maxillary arch size and shape in American Blacks and Whites”. Angle Orthodontist. 70: 297-302.
8. Cassidy K.M., Harris E.F., Tolley E.A. and Keim R.G. 1998:“Genetic influence on dental arch form in orthodontic patients”. The Angle Orthod. 68: 445-454.
9. Currier J.H. 1969:“A computerized geometric analysis of human dental arch form". Am J Orthod. 56: 164-179.
10. Ferrario V.F., Sforza C., Miani Jr. A. and Tartaglia G. 1994 “Mathematical definition of the shape of dental arches in human permanent healthy dentitions”. European Journal of Orthodontics. 16: 287-294.
11. Ferrario V.F., Sforza C., Piggio C.E., Serrao G. and Colombo A. 1999:“Three dimensional dental arch curvature in human adolescents and adults”. Am J Orthod Dentofac Orthop. 115: 1101-1105.
12. Germane N, Lindauer SJ, Rubenstein LK, Revere JH Jr, Isaacson RJ. 1991“Increase in arch perimeter due to orthodontic expansion.” Am J Orthod Dentofacial Orthop. 100(5):421-7.
13. Hassanali J, Amwayi P. (1993)“Biometric analysis of dental casts of Maasai who had extractions of mandibular central incisors and of the Kikuyu”;European Journal of Orthodontics; 15: 513-518
14. Izard G. 1927:“New method for the determination of the normal arch by the function of the face”. International Journal of orthodontics. 13: 582-585.
15. Jones M.L. and Richmond S. 1989:“An assessment of the fit of a parabolic curve to pre- and post-treatment dental arches”. British Journal of Orthodontics. 16: 85-93.
16. Lavelle C.L.B. 1975:“The shape of the dental arch”. Am J Orthod. 67: 176-184.
17. Livshits G, Koblyiansky E. 1991“Fluctuating asymmetry as a possible measure of developmental homeostasis in humans, a review”. Hum Biol.; 63:441–466.
18. MacConill M A, scher E A 1949:“The ideal archform of the human dental arcade with some prosthetic applications”. Dental Record 69: 285-302
19. Merz M.L., Isaacson R.J., Germane N. and Rubenstein L.K. 1991:“Tooth diameters and arch perimeters in a black and a white population”. Am J Orthod Dentofac Orthop. 100: 53-58.
20. Nummikoski P., Prihoda T., Langlais R.P., McDavid W.D., Welander U. and Tronje G. 1988:“Dental and mandibular arch widths in three ethnic groups in Texas: A radiographic study”. Oral Surg Oral Med Oral Path. 65: 609-617.
21. Pepe S.H. 1975:“Polynomial and catenary curve fits to human dental arches”. Journal of Dental Research. 54: 1124-1132.
22. Richards L C, Townsend G C, Brown T, Burgess V B1990 “Dental arch morphology in South Australian twins”. Archives of Oral Biology 35: 983-989
23. Sampson P.D. 1981:“Dental arch shape: A statistical analysis using conic sections”. Am J Orthod. 79 (5): 535-548.
24. Staley R N, Stuntz W R, Peterson L C 1985: “A comparison of arch width in adults with normal occlusion and adults with Class II, division 1 malocclusion”. American Journal of Orthodontics 88: 163–169
25. Stanton F L 1922:“Arch predetermination and a method of relating the predetermined arch to the malocclusion to show the minimum tooth movement”. International Journal of Orthodontics 8: 757-778
26. Tweed Charles H. 1966:“Clinical Orthodontics” Publisher: C. V. Mosby
27. Valenzuela A.P., Pardo M.A. and Yezioro S. 2002: “Description of dental arch form using the Fourier series.”Int J. Adult Orthod Orthognath Surg.17: 59-65. Woo, T.L. (1931) “on the asymmetry of the human skull”. Biometrika22: 324–352.
|