Breath malodour or Halitosisis estimated to be the third most frequent reason for seeking dental treatment, following tooth decay and periodontal disease.1 Most commonly known as bad breath is used to describe noticeably unpleasant odors exhaled in breathing. Halitosis has a significant impact – personally and socially
HALITOPHOBIA
Exaggerated concern of having bad breath, known as halitophobia, delusional halitosis, or as a manifestation of Olfactory Reference Syndrome. These patients are sure that they have bad breath, although many have not asked anyone for an objective opinion.
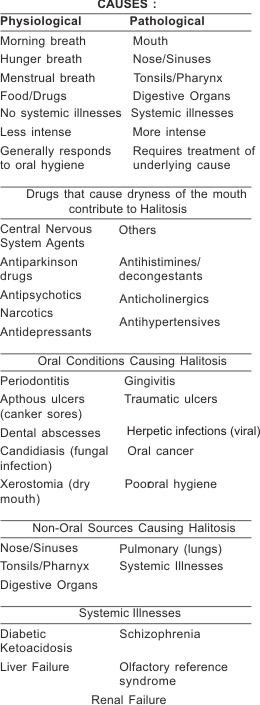
In most cases (85–90%), bad breath originates in the mouth itself. The intensity of bad breath differs during the day, due to eating certain foods (such as garlic, onions, meat, fish, and cheese), obesity, smoking, and alcohol consumption. Because the mouth is exposed to less oxygen and is inactive during the night, the odour is usually worse upon awakening (“morning breath”). Bad breath may be transient, often disappearing following eating, brushing one’s teeth, flossing, and rinsing with pecialised mouthwash.
Bad breath may also be persistent (chronic bad breath), which is a more serious condition, affecting some 25% of the population in varying degrees.2It can negatively affect the individual’s personal, social, and business relationships, leading to poor self-esteem and increased stress.
MOUTH
There are over 600 types of bacteria found in the average mouth. Several dozens of these can produce high levels of foul odors when incubated in the laboratory. The odors are produced mainly due to the anaerobic breakdown of proteins into
individual amino acids, followed by the further breakdown of certain amino acids to producedetectable foul gases. For example, the breakdown of cysteine and methionine produce hydrogen sulfide and methyl mercaptan spectively.Volatile sulfur compounds have been shown to be statistically associated with oral malodor levels, and usually decrease following successful treatment.3
Other parts of the mouth may also contribute to the overall odor, but are not as common as the back of the tongue. These locations are, in descending prevalence order: inter-dental and subgingival niches, faulty dental work, foodimpaction
areas in-between the teeth, abscesses and unclean dentures.
TONGUE
The most common location for mouthrelated halitosis is the tongue. Large quantities of naturally-occurring bacteria are often found on the posterior dorsum of the tongue, where they are relatively undisturbed by normal activity. This part of the tongue is relatively dry and poorly cleansed, and bacterial populations can thrive on remnants of food deposits, dead epithelial cells and postnasal drip. The convoluted microbial structure of the tongue dorsum provides an ideal habitat for anaerobic bacteria, which flourish under a continually-forming tongue coating of food debris, dead cells, postnasal drip and overlying bacteria, living and dead. When left on the tongue, the anaerobic respiration of such bacteria can yield either the putrescent smell of indole, skatole, polyamines, or the “rotten egg” smell of volatile sulfur compounds (VSCs) such as hydrogen sulfide, methyl mercaptan, Allyl methyl sulfide and dimethyl sulfide. Volatile sulphur compounds (VSC) produced in the oral cavity, are a major cause of oral malodour. Zinc (Zn) ions inhibit VSC formation.4
CLEANING THE TONGUE
The most widely-known reason to clean the tongue is for the control of bad breath. Methods used against bad breath, such as mints, mouth sprays, mouthwash or gum, may only temporarily mask the odors created by the bacteria on the
tongue, but can not cure bad breath because they do not remove the source of the bad breath. In order to prevent the production of the sulfurcontaining compounds mentioned above, the bacteria on the tongue must be removed; same
about the decaying food debris present on the rear areas of the tongue. Most people who clean their tongue use a tongue cleaner (tongue scraper), or a toothbrush. Ergonomic, specially designed tongue cleaners are a lot more effective (collecting and removing the bacterial coating) than toothbrushes (which merely spread the bacterial accumulations on the tongue and in the mouth).
GUM DISEASE
There is some controversy over the role of periodontal diseases in causing bad breath. Whereas bacteria growing below the gumline (subgingival dental plaque) have a foul smell upon removal, several studies reported no statistical correlation between malodor and periodontal parameters.5The microbial colonies have shown to correlate with the presence of oral malodour.6 However some studies revealed that periodontal health and oral malodour are not associated with one another.7
NOSE
The second major source of bad breath is the nose. In this instance, the odor exiting the nostrils has a pungent odor which differs from the oral odor. Nasal odor may be due to sinus infections or foreign bodies.
TONSILS
Putrefaction from the tonsils is generally considered a minor cause of bad breath, contributing to some 3-5% of cases.
Approximately 7% of the population suffer from small bits of calcified matter in tonsillar crypts called tonsilloliths that smell extremely foul when released and can cause bad breath.
STOMACH
The stomach is considered by most researchers as a very uncommon source of bad breath (except in belching). The esophagus is a closed and collapsed tube, and continuous flow (as opposed to a simple burp) of gas or putrid substances from the stomach indicates a health problem - such as reflux serious enough to be bringing up stomach
contents or a fistula between the stomach and the esophagus - which will demonstrate more serious manifestations than just foul odor
DIAGNOSIS
Self diagnosis and home diagnosis Scientists have long thought that smelling one’s own breath odor is often difficult due to acclimatization, although many people with bad breath are able to detect it in others. Research has suggested that self-evaluation of halitosis isn’t easy because of preconceived notions of how bad we think it should be. Some people assume that they have bad breath because of bad taste (metallic, sour, fecal, etc), however bad taste is considered a poor indicator. For these reasons, the simplest and most effective way to know whether one has bad breath is to ask a trusted adult family member or very close friend (“confidant”). If the confidant confirms that there is a breath problem, he or she can help determine whether it is coming from the mouth or the nose, and whether a particular
treatment is effective or not. One popular home method to determine the presence of bad breath is to lick the back of the
wrist, let the saliva dry for a minute or two, and smell the result. This test results in overestimation, as concluded from research, and should be avoided. A better way would be to lightly scrape the posterior back of the tongue with a plastic
disposable spoon and to smell the drying residue. A spouse, family member, or close friend may be willing to smell one’s breath and provide honest feedback. Home tests are now available which use a chemical reaction to test for the presence of polyamines and sulfur compounds on tongue swabs, but there are few studies showing how well they actually detect the odor. Furthermore, since breath odor changes in intensity throughout the day depending on many factors, multiple testing may be necessary.
Professional diagnosis
Key points for dentists8:
1. Malodour is common on awakening(morning breath)
2. If real, is usually caused by diet, habits, dental plaque or oral disease
3. It can be measured with a halimeter
4. It often significantly improves with oral hygiene
5. It can sometimes be caused by sinus, nose or throat conditions
6. It is rarely be caused by a more serious disease
If bad breath is persistent, and all other medical and dental factors have been ruled out, specialised testing and treatment is required. Hundreds of dental offices and commercial breath clinics now claim to diagnose and treat bad breath. They often use some of several laboratorial methods for diagnosis of bad breath:
1. Halimeter: a portable sulfide monitor used to test for levels of sulfur emissions (specifically, hydrogen sulfide) in the mouth air. When used properly this device can be very effective at determining levels of certain VSC-producing
bacteria. However, it has drawbacks in clinical applications. For example, other common sulfides (such as mercaptan) are not recorded as easily and can be misrepresented in test results. Certain foods such as garlic and onions produce sulfur in the breath for as long as 48 hours and can result in false readings. The Halimeter is also very sensitive to alcohol, so one should avoid drinking alcohol or using alcohol-containing mouthwashes for at least 12 hours prior to being tested. This analog machine loses sensitivity over time and requires periodic recalibration to remain accurate.
2. Gas chromatography: portable machines, such as the OralChroma, are currently being introduced. This technology is specifically designed to digitally measure molecular levels of the three major VSCs in a sample of mouth air (hydrogen sulfide, methyl mercaptan, and dimethyl sulfide). It is accurate in measuring the sulfur components of the breath and
produces visual results in graph form via computer interface.9
3. BANA test: this test is directed to find the salivary levels of an enzyme indicating the presence of certain halitosis-related bacteria.
4. β-galactosidase test: salivary levels of this enzyme were found to be correlated with oral malodor.10
HOME CARE AND TREATMENT
Currently, chronic halitosis is not very well understood by most physicians and dentists, so effective treatment is not always easy to find. Six strategies may be suggested:
1. Gently cleaning the tongue surface twice daily is the most effective way to keep bad breath in control; that can be achieved using a tongue cleaner or tongue brush/scraper to wipe off the bacterial biofilm, debris and mucus. An inverted teaspoon may also do the job; a toothbrush should be avoided, as the bristles only spread the bacteria in the mouth,
and grip the tongue, causing a gagging reflex. Scraping or otherwise damaging the tongue should be avoided, and scraping of the Vshaped row of taste buds found at the extreme back of the tongue should also be avoided. Brushing a small amount of antibacterial mouth rinse or tongue gel onto the tongue surface will further inhibit bacterial action
2. Patients suffering from halitosis should take a well-balanced diet consisting of seeds, nuts, grains, vegetables, and fruits, with emphasis on raw and cooked vegetables, and fruits. In case of constipation, all measures should be adopted for its eradication. The patient should avoid refined carbohydrate foods, such as white sugar; white bread and products made from them, as well as meat find eggs.
3. Chewing gum: Since dry mouth can increase bacterial buildup and cause or worsen bad breath, chewing sugarless gum can help with the production of saliva, and thereby help to reduce bad breath. Chewing may help particularly when the mouth is dry, or when one cannot perform oral hygiene procedures after meals (especially those meals rich in protein). This aids in provision of saliva, which washes away oral bacteria, has antibacterial properties and promotes mechanical activity which helps cleanse the mouth. Some chewing gums contain special anti-odor ingredients.
Chewing on fennel seeds, cinnamon sticks, mastic gum or fresh parsley are common folk remedies.
4. Gargling right before bedtime with an effective mouthwash (see below). Several types of commercial mouthwashes have been shown to reduce malodor for hours in peerreviewed scientific studies. Mouthwashes may contain active ingredients which are inactivated by the soap present in most toothpastes. Thus it is recommended to refrain from using mouthwash directly after toothbrushing with paste (also see mouthwashes, below).[24]
5. Maintaining proper oral hygiene, including daily tongue cleaning, brushing, flossing, and periodic visits to dentists and hygienists. Flossing is particularly important in removing rotting food debris and bacterial plaque from between the teeth, especially at the gumline. Dentures should be properly cleaned and soaked overnight in antibacterial solution
(unless otherwise advised by your dentist).
6. Maintain water levels in the body by drinking several glasses of water a day.
MOUTHWASHES
Mouthwashes often contain antibacterial agents including cetylpyridinium chloride, chlorhexidine, zinc gluconate, essential oils, and chlorine dioxide. Zinc and chlorhexidine provide strong synergistic effect. They may also contain alcohol, which is a drying agent. Rinses in this category include Scope and Listerine. Other solutions rely on odor eliminators like oxidizers to eliminate existing bad breath on a short-term basis. Rinses in this category include
SmartMouth, Therabreath, Closys and others. A relatively new approach for home-care of bad breath is by oil-containing mouthwashes. The use of essential oils has been studied, was found effective and is being used in several commercial
mouthwashes, as well as the use of two-phase (oil:water) mouthwashes, which have been found to be effective in reducing oral malodor.
REFERENCES
1. Loesche WJ, Kazor C. Microbiology and treatment of halitosis. Periodontology 2000. 2002;28:256-79.
2. Bosy A, Oral malodor: philosophical and practical aspects. J Can Dent Assoc. 1997 Mar;63(3):196-201
3. Rosenberg M. Clinical assessment of bad breath: current concepts. J Am Dent Assoc. 1996 Apr;127(4):475-82.
4. The oral anti-volatile sulphur compound effects of zinc salts and their stability constants. Eur J Oral Sci.2002
Feb;110(1):31-4.
5. Bosy A, Kulkarni GV, Rosenberg M, McCulloch CA. Relationship of oral malodor to periodontitis: evidence of
independence in discrete subpopulations. J Periodontol. 1994 Jan;65(1):37-46.
6. John M, Vandana KL. Detection and measurement of oral malodour in periodontitis patients. Indian J Dent Res
2006;17:2-6
7. Association between oral malodour and periodontal diseaserelated parameters in a population of 71 Israelis. Oral Dis. 2005;11 Suppl 1:72-4
8. C. Sccully and D.H. Felix.Oral Medicine- update for the dental practitioner. Oral malodour. Brithish Dental Journal2005
oct;199(8):498-500
9. Murata T, Rahardjo A, Fujiyama Y, Yamaga T, Hanada M, Yaegaki K, Miyazaki H. Development of a compact and simple gas chromatography for oral malodor measurement. J Periodontol. 2006 Jul;77(7):1142-7. PMID 16805675.
10. Sterer N, Greenstein RB, Rosenberg M. Beta-galactosidase activity in saliva is associated with oral malodor. J Dent Res. 2002 Mar;81(3):182-5. |