I) Introduction
Can a New Smile Make You Look More Intelligent and Successful?
A smile has a tremendous impact on perceptions of one’s attractiveness and one’s personality. Previous psychological research has shown that attractive people are perceived as more successful, intelligent, and friendly -Anne E. Beall
One who works with his hands is a Labourer,
One who works with his hands and mind is a Craftsman,
One who works with his hands, mind and heart, is an Artist
Dentist have been making beautiful smiles for centuries. Indeed, a dentist is an artist & esthetic dentistry an “Artist science”.
In the field of dentistry, the esthetic approach always has always been based on the imitative elaboration of forms, colors and structures whose intrinsic beauty is supposed to enhance the patient’s appearance. However the mental perception of an object and its concrete realization based on the perception must be considered purely static.[1]
Personality, motivations, desires, expectations, self-esteem ability to accept change, and willingness to cooperate are important factors for successful treatment. Therefore an awareness of self theory and a broad application of psychologic and sociologic principles can greatly enhance a dental practice that emphasizes esthetics.[2]
II) History
Vulcanite was the first universally acceptable denture material. Patented by Nelson Goodear in 1851, it was made by heating caoutchouc (Indian rubber) with sulphur, resulting in a firm yet flexible material. The open-faced crown was invented around 1880, the interchangeable porcelain facing (a ridged facing that fitted into a grooved pontic) was developed in the 1880s,and the porcelain jacket crown came into vogue in the early 1900s.By 1897 a relatively modern composition of silicate cement was developed. Further modifications continued until 1938, when the American Dental Association (ADA) published its definitive specification of acceptability known as "ADA Specification No.9." This was the first cosmetic dental material to be acceptedby the ADA. However, newer and more exciting innovations were about to arrive. In the 1930s chemically activated acrylic resins were developed. By the 1970s composite resins virtually replaced acrylic resins and silicate cements as "permanent" restorations. Refinements of this basic formula of resin matrix and glass filler are currently in use. Acid etching, often called bonding, radically changed cavity treatment by emphasizing conservation of tooth structure. It also allowed for the numerous veneering techniques introduced in the 1970s. Variations include direct resin veneers, commercially produced acrylic "shells," and laboratory-processed veneers of resin and porcelain. In 1916, Adams reported the use of hypochloric acid to treat fluorosis. In 1937, Ames reported a technique using a mixture of hydrogen peroxide and ethyl ether on cotton, heated with metal instrument for 30 minutes and applied over 5 to 25 visits to treat mottled enamel. The first commercially available 10% carbamide peroxide was developed and subsequently marketed by Omni International in 1989. Success can be attributed to great attention to detail in areas of planning the case, tooth preparation of teeth, fabrication and maintenance of this restorations.[1]
III) Esthetics In Restorative Dentistry: Why It Is Important?
Esthetic or cosmetic dentistry has become one of the main areas of dental practice, emphasis and growth for several years. Increasingly, patients seeking treatment for their oral condition with the primary concern of an esthetic enhancement[3]. In social interactions, our attention appears mainly on mouth and eyes of the face of the person speaking. As the mouth is the centre of communication in the face, the esthetic appearance of the oral region during smiling is a conspicuous part of facial attractiveness[4]. The last 50 years have witnessed an unimaginable amount of change in restorative dentistry.
Wayr23;S To Assess Smile:
There are certain vital elements of smile designing which includes the following:
1. Tooth Components : Dental midline, Incisal length , Tooth dimensions, Axial inclinations Zenith points , Incisal embrasures, Interdental contact area and Interdental contact points Sex, personality and age ,Symmetry and balance.
2. Soft Tissue Components: Gingival health ,Gingival level ,Smile line ,Interdental embrasure.
Dental Midline:
These are least noticed by the patients and dental personnel. As long as the midline is parallel with the long axis of the face, midline discrepancies of up to 4 mm will generally not be perceived as unesthetic. Slight corrections of midline can be corrected by restorative dentistry. The ideal treatment is orthodontics[3].
Incisal Length:
Published reports have shown that the average 30year old woman displays about 3.5 mm of maxillary incisor tooth structure when the lips are at rest. The prosthodontic literature has generally recommended setting denture teeth so that 2 mm of tooth structure is displayed at rest[2]. If patient displays less than 4 mm of the maxillary centrals at rest, the teeth need to be lengthened and this length will be achieved by adding to the incisal edge.
Tooth Dimensions:
If the incisal display at rest is 3 mm to 4 mm, and it is determined that the teeth are too short, then surgical crown lengthening procedures should be considered[3]. If there is insufficient tooth display at rest, normal lip mobility, the teeth are of the correct length, and there is inadequate tooth display during smiling, then this is diagnosed as vertical maxillary insufficiency. This is not a case that should be treated with esthetic tooth lengthening. This is an orthognathic problem and should be referred for proper treatment[5].
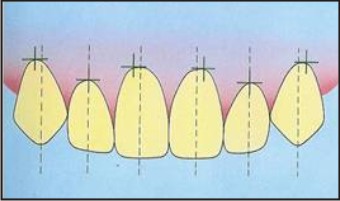
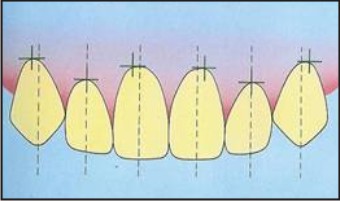
Axial inclinations:
Tooth inclinations compares the vertical alignment of maxillary teeth, visible in the smile line, to central vertical line. The evaluation of axial inclination can be done on a photograph of the anterior teeth in a frontal view. A line is sketched on each tooth from the midline of the incisal edge through the midline of the tooth at its gingival interface[1].
Zenith points:
It is the most apical point of the gingival tissues along the long axis of the tooth.
 | Zenith Point
 |
Incisal embrasures and contact points:
From central to canine, an open space is formed between the proximal surfaces of incisal edges from the contact points. These embrasure spaces terminate at the contact points with the adjacent teeth. Failure to provide adequate depth and variation to the incisal embrasure will make the teeth appear too uniform and contact areas too long which gives box like appearance of the dentition[1].
Sex, Personality and Age (SPA):
Minor differences in the length, shape and positioning of the maxillary teeth allow for dramatic differences.
For Female, the maxillary incisors should be round smooth, soft delicate and for male, should be cuboidal, hard and vigorous.
Youthful teeth: unworn incisal edge, defined incisal embrasure, low chroma and high value
Aged teeth: shorter; so less smile display, minimal incisal embrasure, high chroma and low value.
Personality:
Aggressive, hostile angry: pointed long “fangy” cusp form, passive soft: blunt, rounded , short cusp form[1].
Symmetry and Balance:
Lip symmetry involves the mirror image appearance of each lip when smiling. Independent evaluation of upper and lower lip is essential when analyzing both symmetry and fullness. Sometimes plastic surgery is necessary to provide results desired by the patients. Balance is observed as the eyes move distally from the midline, so that both the sides of the smile are well balanced[1].
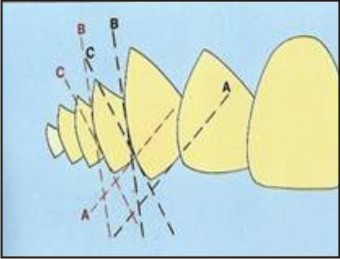
Gradation
When similar structures are aligned one after the other, they undergo a progressive visual reduction of size from the nearest to the farthest. The prerequisite of the "front-back progression" of the teeth is the alignment of the outline or contour of the buccal surface, incisal 1/3rd, median 1/3rd, and, at a lower rate, the gingival 1/3rd, as well as the alignment of the incisal¬ mesiobuccal Inclines. The presence of a poorly shaped tooth, differences in tooth length, gingival disharmonies and colored restorations create problems with respect to the gradation effect. The buccal corridor or lateral negative space between the buccal outline of posterior teeth and the corner of the mouth helps in achieving gradation effect in progressively altering tooth illumination. The front-back progression is determined by arch form and a key element, usually the canine or the premolar, is a prerequisite for ensuring the visualization of the gradation effect.
 | Gradation 1
|
 | Gradation 2
|
Soft Tissue Component Of Smile Design
Gingival health, level and harmony:
The gingival frame the teeth and add to the symmetry of the smile. The health, colour and texture of the gingival tissues are paramount for long term success and the esthetic value of the treatment. Healthy gingiva is usually pale pink in colour, stippled, firm and should exhibit a matte surface. A normal healthy gingival sulcus should not exceed 3 mm in depth.
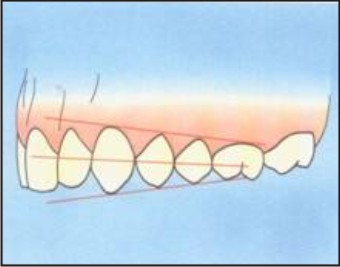
Smile Line:
Its an imaginary line drawn along the incisal edges of the maxillary anterior teeth. In an esthetic smile, the edges of the maxillary anterior teeth follow a convex or gull-wing course matching the curvature of the lower lip[2]. In a reverse smile line, the centrals appear shorter than the cuspids along the incisal plane. Lip line should not be confused with the smile line.
Interdental embrasures:
The darkness of the oral cavity shouldn’t be visible in the inter-proximal triangle between the gingival and the contact area. The black triangles will be avoided if the most apical point of the restoration is 5 mm or less from the crest of the bone. Sometimes this will require long contact area and will be extended towards the cervical. Which encourage the formation of healthy pointed papilla instead of the blunted tissue form that often accomplishes a black triangle.[6]
Facial Composition:
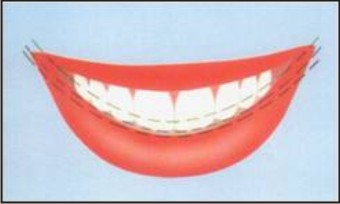
Lip line:
When smiling, the inferior border of the lip as it relates to the teeth and gingival tissues is the lip line. Dentistry has arbitrarily classified 3 types of smiles that, relating the height of the upper lip relative to the maxillary anterior central incisors which are referred to as presenting a low lip line, middle lip line,
high lip line.
Average lip line-exposes the maxillary teeth and only the interdental papilla.
Low lip line: exposes no gingival tissues when smiling.
High lip line: exposes the teeth in full display also gingival tissues above the gingival margins [7].
 | Lip Line
|
Interpupillary line:
This should be parallel with the horizon line and perpendicular to the midline of the face. Also it should be parallel with the commisure line and occlusal plane.
Esthetic Smile:
Golden Proportions: The application of the golden number to dentistry was first mentioned by Lombard and developed by Levin. Levin observed that the most harmonious recurrent tooth-to-tooth ratio was found in the golden proportion. This implies that the maxillary central incisor should be approximately 60% wider than the lateral incisor, which in turn should be 60% wider than the mesial aspect of the canine, the distal aspect of the canine being obscured from the facial aspect. He further demonstrated that the lateral negative space, the area that appears between the anterior segment of the teeth and the corner of the mouth on smiling, is in golden proportion to one half the width of this anterior segment. He developed a grid to help the prosthodontist detect what is esthetically wrong in the anterior proportional relationship.
 | Golden Proportion
|
Recurring Esthetic Dental (Red) Proportion:
The successive width proportion when viewed from the facial aspect should remain constant as we move posteriorly from midline which offers great flexibility to match tooth properties with facial proportions-Ward1. Generally the values of the RED proportions used are between 60% and 80%. Once the ideal size of the central incisor has been calculated, the width of the central incisor is multiplied by the desired RED proportion to determine the frontal view width of the lateral incisor. The resulting lateral incisor width is multiplied by the same RED proportion to yield the desired frontal view of the canine. A mathematical formula has been arrived to calculate the width of the maxillary central incisor for any RED proportion given a fixed view width. And this width is determined by measuring the frontal view width between the distal aspects of the 2 maxillary canine teeth which is (frontal view of the anterior 6 teeth)/2(1+RED+RED2) =width of central incisor[8].
Esthetics In Implants Dentistry
A partial denture or an implant often replaces missing teeth. Dental implant provides several advantages over the conventional tooth-borne fixed prosthesis. New requirements have emerged for surgical and prosthetic requirements when implants are involved. The use of an implant avoids unnecessary sacrifice of intact tooth structure and avoids long span dentures. Cylindrical shaped implants provide long lasting support to the prosthesis and also provides better survival rates. Studies on the longevity of implants consider the survival time and esthetic consideration of the implant. Functional and esthetic success is essential to long term successful outcome.
Periodontics To Enhance Esthetics
The combination of periodontal esthetic surgery with other restorative procedures can create a synergistic esthetic result.
Periodontal treatment consists of a variety of solutions to improve smile
1. Teeth stains - Scaling-polishing and vital bleaching
2. Black triangle- placing restoration 5mm or less from crest of bone
3. Aberrant frenulum-Frenotomy or Frenectomy
4. Excessive gingival display - Crown lengthening procedure
5. Loss of papillae - Reconstruction of papilla
6. Exposed root surfaces - Root coverage
7. Loss of tooth - Implant supported restorations
8. Loss of adjoining hard and soft tissues -Ridge augmentation
9. Excessive gingival pigmentation - Gingival dipigmentation
10. Asymmetry in gingival contours - Gingival recontouring
 | Crown Lengthing
|
Smile Design In Prosthodontics:
Smile Design For Full Mouth Rehabilitation: Full mouth rehabilitations deals with the science of treating a mutilated dental situation which involves treatment of many or all teeth and helps them function in harmony with the surrounding muscles and the TM joint. Full mouth rehabilitation is needed when the teeth are worn down, broken, missing or if u experience pain in the jaw joint, headaches , muscle tenderness or clicking of the jaw. This utilizes current technologies to reshape and rebuild ones teeth, gums and surrounding areas.
Role Of Orthodontics For Esthetics
The restorative dentist should consider pre-restorative orthodontic correction and should modify the treatment plan to accommodate the patient’s wishes. An esthetic treatment plan must consider whether orthodontic movements will enhance the success or stability or the final restorations.
Rational For Orthodontic Intervention
1) To enhance masticatory efficiency
2) Periodontal protection
3) Maintaining the oral hygiene
4) Temporomandibular joint protection
5) Speech improvement
6) Esthetics
 | Diastema Closure
|
V) Conclusion:
From the above discussion, it is vivid that the smile we create should be esthetically appealing and functionally sound too. We the dentist should carefully dignose analyze and deliver the best to our patients by considering all the above factors. In todayR23;s world, the smile is consider an important component of an individualR23;s over all appearance and well being. Scientific analysis of beautiful smiles has shown that the principle of Golden Proportion or RED proportions can be systematically applied to evaluate and to improve denture esthetics in predictable ways. The aim of smile design must be less tooth structure reduction and greater esthetics and durability.
References:
1. Mohan Bhuvaneswaran. Principles of smile design. J Conserv Dent . 2010 Oct – Dec; 13(4): 225-232.
2. Vig RG, Brundo Gc. The Kinetics of anterior tooth display. J Prosthet Dent. 1978:39; 502-504.
3. Edward A. McLaren, DDS, MDC : and Phong Tran Cao, DDS Smile Analysis and Esthetic Design: “In the Zone” INSIDE DENTISTRY JULY/AUGUST 2009.
4. Pieter Van der Geld , Paul Oosterveld and Annie Marie Kujjpers-Jagtman. Age-related changes of the dental aesthetic zone at rest and during spontaneous smiling and speech European Journal of Orthodontics 30(2008)366-373.
5. Robbins JW.Differential diagnosis and treatment of excessive gingival display. Pract Periodontics Aesthet Dent.1999;2:265-272.
6. Tarnow DP, Manager AW, Fletcher P. The effect of the distance from the contact point to the crest of the bone on the presence or absence of the interproximal papilla . J Periodontal . 1992; 63:995-6.
7. Patil Ratnadeep. Esthetic dentistry: An artistR23;s science .1st ed.Mumbai:PR Publications;2002.p.16-36.
8. Ward DH. Proportional smile design using the recurring esthetic dental (RED) proportion. Dent Clin North Am. 2001; 45:143-154.
|