Introduction
Patients with complete denture often complain of reduced masticatory efficiency as compared to their natural counterparts. From previous studies, dentists have become more aware that tooth retention in association with complete dentures is valuable for the preservation of the structure of the alveolar bone and sensory proprioception.[1]
The concept of overdentures developed as a simple and economic alternative to prolong the retention and function of the remaining few teeth in a compromised dentition. This concept is not new but its use has been in literature back over 100 years. An overdenture is a removable complete or removable partial denture that has one or more roots of remaining teeth to provide support. Rather than extracting all compromised teeth, the crowns and pulpal tissue of selected teeth are removed. The remaining root projecting through the mucosa is restored and/or contoured. Overdentures with roots are more stable, retentive and patients can chew better than with denture supported on residual alveolar bone and mucosal tissue alone.
The presence of natural teeth under dentures can increase the lateral stability and retention of the denture base. These conditions in turn aid the patient in becoming accustomed to the prosthesis more readily. In theory, the proprioception provided by retained teeth should result in better perception of food particle size during chewing and thereby enable the patient with overdentures to masticate food more efficiently [1]
Rationale for over denture concept
• Extraction of all natural dentition and replacement with complete denture is not the most desirable treatment
• Preventive prosthodontics emphasizes the importance of any procedure that can delay or eliminate further prosthodontic problems
• The over denture is a logical method for a dentist to use in preventive prosthodontics.[2]
Indications
• For patients who face the loss of remaining natural adult dentition. Therefore, younger the patient greater the indication
• Patents with badly worn out dentition
• Cleft palate cases
• For congenital anomalies like microdontia, in selected partial anodontia cases. Amelogenesis imperfecta and dentinogenesis imperfecta
• Denture for patients with maxillofacial trauma.[2]
Contra Indications
• Uncooperative and under motivated patients
• Mentally and physically handicapped patients for whom good oral hygiene is difficult to maintain
• Economically compromised patients.[2]
A tooth retained overdenture is an excellent way of maintaining healthy viable bone around the roots of the teeth and a great way to support and retain a denture for improved speech, breathing, tongue position and increased taste.
In a 4-year-study, Renner et al showed that 50% of roots, used as overdenture abutments remained immobile. In addition, 25% of roots that were initially mobile became less mobile.Hence, they suggested, that teeth that are generally compromised can be used for overdentures after root canal therapy and decoronation.The use of attachments can re¬direct occlusal forces away from weak supporting abutments and onto soft tissue, or redirect occlusal forces toward stronger abutments and away from soft tissues. They act as shock absorbers and stress redirectors as well as provide superior retention.[3]
Implant supported overdenture help in regaining the lost supported structures for edentulous patients. The mandible is well suited for implant-retained overdentures, particularly when placed in the intercanine region. Various attachment systems are used nowadays amongst which, ball attachments have been proved to be quick.[4]
Dental precision attachments connect removable partial dentures a to fixed male/female locking mechanism. Some advantages to dental precision attachments include maintainable periodontal health, less force on abutment teeth, cosmetic appearance, longevity and stability.
The ‘male’ part is fixed to the crown or bridgework whereas the ‘female’ part holds the removable partial denture. There are a variety of male/female locking mechanisms available, these include ball and socket, friction grip slide attachment, latch burs, post and socket, spring retained socket and snap-on/screw in. The male part of dental precision attachments is often a high strength precious alloy whereas the female part consists of a more elastic alloy.
A patient might prefer one precision attachment over the other depending on ease of attachment. Some dental precision attachments are better suited for different areas of the jaw. Type of locking mechanism, material of precision attachment and intended use, all should be considered when choosing a dental precision attachment. In this case report various ball attachments were used in different patients.
Case Report - 1
A 50-year-old male patient had reported to the Department of Prosthodontics with few remaining natural teeth and a chief complaint of difficulty in chewing. Clinical examination revealed partially edentulous maxillary and mandibular arch. Teeth present in lower arch were 43,33,34. Loss of teeth had occurred due to decay, mobility and lack of oral hygiene practice in earlier life. Pre-operative intraoral periapical radiographs were taken which revealed that the tooth roots were surrounded by healthy periodontium and bone. It was concluded that mandibular canines could serve as abutments for an overdenture thus providing required retention and stability and a coping for 34 was planned. Diagnostic mounting revealed adequate interarch distance for necessary components and esthetic and functional placement of acrylic teeth.
Considering patient’s complaint, background and condition of the oral cavity; an overdenture was planned with attachments ( Preci-Clix- DFS Belgium).
First part involved intentional endodontic preparation with subgingival finish line in relation to 33,34 and 43. A short metal coping was given for 34.
Post space was prepared with the drilling bur, diamond bur was used to prepare the base of the post. Finally, the reamer was used to prepare the diameter of the post.Cementation of the post was done with glass ionomer cement FUJI II.
Following conventional technique segmental border moulding of the tray was done with low fusing impression compound. Then the spacer was removed and vent holes were made in the tray. Final impression was made with addition silicone (3M). Stainless steel post analogues were taken and re-indexed into the recess within the impression and master casts was made. (Figure 1, 2, 3, 4).
 | Figure 1. Showing Metal Housing With Retention Caps Placed Over The Posts On The Cast.
 |
 | Figure 2. Showing Large Tin Spacer Placed Over The Ball Coping And Is Contoured Around It And Gingival Area. Black Rubber Space Maintainer Was Placed On The Ball Over The Tin Spacer.Female Component Was Seated Over Both The Ball Copings.
|
 | Figure 3. Denture Was Processed In Conventional Manner.Thetin And Black Rubber Spacers Were Removed. The Rubber Insert Could Be Easily Changed In The Metal Housing To Adjust Retention.
|
 | Figure 4. Showing The Intaglio Surface Of The Mandibular Denture (With Female Housing).
|
Case Report – 2
A 40-year-old female patient had reported to the Department of Prosthodontics with few remaining natural teeth and a chief complaint of difficulty in chewing. Clinical examination revealed completely edentulous maxillary and partially edentulous mandibular arch. Teeth present in lower arch were 44, 43,33. Metal coping was given for 44.
EDS system was used for this overdenture. Female part of this system consists of only plastic ring which is directly inserted into denture in the chair side procedure. There is freedom from metal housing as seen in other system (Figure 5, 6, 7, 8).
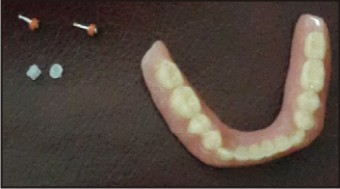 | Figure 5. Showing Final Mandibular Prosthesis With Eds Attachments.
|
 | Figure 6. Depicting Posts With Female Housing In Place.
|
 | Figure 7. Preparation Of Two Holes Corresponding To The Posts.
|
 | Figure 8. Self-cure Acrylic Used For Embedding The Female Housing And Sealing The Holes Within The Denture.
|
Case Report- 3
A 35-year-old completely edentulous lady reported to department. Overdenture was planned with two implants in mandibular arch in canine region. After doing clinical (visual inspection, bone mapping) and radiographic investigation two Bio horizon implants 3.0 diameter with 12 mm length were planned and placed in the mandibular arch. The intangilo surface of the denture was relieved and relined with temporary soft liner material (monoplast – B). After 3 months when satisfactory bone formation was observed, precision attachment placement was planned. (Figure 9).
Rest of the procedure of attachment is similar to that of chairside technique as in EDS system (Figure 10).
 | Figure 9. Female Metal Housing Was Attached To Implant. Holes Were Made In The Prosthesis To Make Room For Attachments.
|
 | Figure 10. Showing Implant Overdenture Attachments
|
Discusson
Conventional dentures rely upon the residual alveolar ridge and mucosa for support and retention. Many patients have problems adapting to their complete dentures, especially to the mandibular prosthesis.
Tooth supported overdenture is a viable and tissue tested alternative technique for those who cannot have implants due to various reasons like medical contra-indications, cost factors and also for patients who are not willing for the implants. The advantages includes effective and superior method of treatment for edentulous case, ease of maintenance, stable and retentive, reasonable cost compared to implants, familiar procedure and excellent patient acceptance.[5]
Preserving the teeth and making the denture, tooth and tissue borne, helps in preserving the supporting structures, both in health and function.
The literature reports that in the elderly population it is common to observe poor dentition, affected by periodontal disease and dental caries. In certain situations, the patient is limited to being rehabilitated with complete dentures due to the fact that no other option is available. However, the use of selective remaining teeth in strategic positions can greatly improve the final treatment result in terms of overdenture stability and retention. [6]
In a study done by Li Chen, the patients in the comparative masticatory efficiency test restored with implant-supported overden-tures and tooth-supported overdentures sho-wed higher comparative masticatory efficiency than those restored with conventional complete dentures.[7]
Attachment stabilizes the prosthesis and the patient is able to consistently reproduce a determined centric occlusion. However, it is important to minimize stress on abutment without compromising the denture strength.
The ball and socket type of attachment is seen to be user friendly for the patients. The snap fit of the denture in mouth makes the patient more comfortable during functional movements.[5]
With incorporation of attachments in the denture there is loss of considerable denture material from that site, which further leads to loss of strength at that portion of denture.
Follow up of four months for above three cases showed discoloration of denture around the area of attachments which were inserted by chairside procedure. This is due to deterioration of self-cure resin in oral cavity. Heat polymerized material have been proven to have higher mechanical properties when compared to auto polymerised material[8]. Insufficient flexural strength of auto polymerizing acrylic resin is lower than that of Heat polymerizing acrylic resin.[9] Breakage of prosthesis occurs around attachment region in chair side made overdenture. Common problems like denture sore occurs at gingival level of abutments as there is excessive bulging of tissue. Trimming of denture for such reasons further causes loss of thickness and strength.
Compared with the chair side processing of attachments there is no incidence of discoloration in laboratory technique. Also wax up can be recontoured in the laboratory processing to provide more room for future adjustments in acrylic around attachment areas.
Conclusion
Ball attachments are economical and easily available for overdenture. Fabrication with them is easier as compared with other attachments such as Graber, Dalbo, Rotherman and Zest anchor.
Laboratory procedure for attaching ball attachments provides more durable and long lasting prosthesis as compared with chair side procedure. These attachments are reliable and more acceptable by the patient.
References
1. Rissin L, House JE, ManlyRS and Kapur KK. Clinical comparison of masticatory performance and electromyographic activity of patients with complete dentures,overdentures and natural teeth. J Prosthet Dent 1978; 39:508-11.
2. Prakash VS, Shivaprakash G, Hegde S, Nagarajappa. Four and two tooth suppoeted-conventinal overdenture: 2 case reports. Int J Oral Health Sci 2013; 3:61-4.
3. Gupta N, Goyal D, Agarwal M, Gupta P, Mathur M. Overdenture with access post system : A case report.Int J Dent Clincs 2012;4:77-9.
4. Mhatre S, Ram SM, Mahadevan J, Karthik M. Rehablitation of an edentulous patient with implant supported overdenture. J Prosthet Dent 1998;80:559-64.
5. Hallikerimath RB, Patil V, Sh, Magadum S. Prosthodontic rehabilitation with Preci-clix overdenture system- A case report. Int J Clin Dent Sci 2010; 1:73-6.
6. De Souza BE, De Faria ADA, Ferrira SJJ, Goncales VAC, Piza PE, FellippoRamos V. Root-supported overdenture associated with temporary immediate prosthesis - A case report. Oral Health Dental Management 2014; 13:159-63.
7. Doundoulakis JH, Eckert SE, Lindquist CC, Jeffcoat MK.The implant-supported overdenture as an alternative to the complete mandibular denture.J Am Dent Assoc. 2003;134:1455-8
8. Arioli Filho JN, Butignon LE, Pereira RDP, Lucas MG, MolloJunior FDA. Flexural strength of acrylic resin repairs processed by different methods: water bath, microwave energy and chemical polymerization. J Appl Oral Sci 2011; 19:249-53.
9. Nagai E, Otani K, Satoh Y, Suzuki S. Repair of denture base resin using woven metal and glass fiber : Effect of methylene chloride pretreatment. J Prosthet Dent 2001; 85:496-500.
|