Introduction
Tooth eruption is a process of biological maturation, which comprises the axial movement of a tooth from its intraosseous location through the alveolar process towards the functional position in the occlusal plane.[1] Impaction is the cessation of the eruption of a tooth caused by a clinically or radiographically detectable physical barrier in the eruption path or due to an abnormal direction of the tooth.[2] Delayed tooth eruption is the emergence of a tooth into the oral cavity at a time that deviates significantly from norms of eruption established for different races, ethnicities, and sexes.[3] Impaction may be bony or soft tissue impaction. Impaction of permanent teeth is one of the severe problems that can occur during the mixed dentition period or beyond.
The most common impacted tooth is third molar, followed by maxillary permanent canine and mandibular second premolar.[4] Primary retardation refers to the failure of eruption before emergence without a physical barrier in the eruption path and not due to an abnormal position and is caused by the disturbance in the primary follicle which fails to initiate bone resorption in eruption path.[5] While secondary retardation refers to the cessation of eruption of a tooth after emergence without a physical barrier in the eruption path and not due to an abnormal position and ankylosis is the main etiological factor.[6]
Dachi and Howell, 1961 found the incidence of impacted canine in maxilla is 0.92% and of other non-third molar impaction is to be 0.38%. The Impaction of permanent first molars is very low; the prevalence is 0.01% in normal population. The first permanent molar seems to be impacted more frequently than the second permanent molars.[7] Impaction of primary teeth is rare and when it happens the teeth are maxillary primary second molars.
Local factors for impaction are supernumerary teeth, odontogenic tumors (such as ameloblastic fibroma, odontogenic fibroma and odontoma), cysts, malformed teeth, delayed tooth development, insufficient arch space, inclination against the second primary molar, and mucosal barrier due to gingival fibrosis.[8] Any failure of the follicle of an erupting tooth to unite with the mucosa will entail a delay in the breakdown of the mucosa and constitute a barrier to emergence.
There are systemic factors that influence delayed eruption or impaction of teeth. The systemic factors include a familial tendency to retardation of eruption and metabolic or endocrine disturbances (hypothyroidism, hypopituitarism and Vitamin D deficiency), syndromes (Gardner’s syndrome, Cleidocranial dysplasia, Cleft lip and palate, Aarskog syndrome, Zimmerman laband syndrome).[3] In all these conditions multiple teeth are involved or entire dentition is involved. In the present case all the first permanent molars were involved but the causes were local.
Angle has postulated that permanent first molars are "key teeth" in occlusion, as they support the main mastication, influence the vertical distance between upper and lower arches and their eruption is especially important for the co-ordination of facial growth. Therefore, impaction of permanent first molar can alter the “key of occlusion” and result disturbed mastication, short lower facial height.[9] Moreover, management of these teeth after root development is complete and adaptive movements of adjacent teeth have occurred is difficult and the prognosis is poor.[10] There may be development of dentigerous cyst, pre-eruptive caries, periodontal problems or infection from the impacted tooth.
Case Report
An 8-year, 6-month-old girl reported to the department of Pedodontics and Preventive dentistry, Himachal dental college, Sundernagar with the complaint of not erupting permanent teeth. Medical history revealed no hypothyroidism or hypopituitarism and Vit D deficiency as well as no familial history of impacted teeth. On clinical examination, all the maxillary and mandibular first permanent first molars were impacted (Figure 1, 2). The maxillary and mandibular central incisors were erupted; therefore, the dental age of the patient is 8 years. On palpation, the crowns of the impacted teeth were palpable in their respective position and a thick band of mucosa over the crowns of the impacted teeth was found which was very firm. There was no other abnormality found on clinical examination.
The panoramic radiograph showed vertical position of the impacted teeth with a thick band of mucosa covering the crown of the teeth and root formation of all the first permanent molars was almost complete i.e. Nolla’s 9th stage (Figure 7). There was no bone covering the crowns of the impacted teeth. All the teeth were developing at normal pace on radiographic evaluation.
 | Figure 1 & 2:Intraoral Preoperative Photographs Showing All Impacted First Permanent Molars
 |
 | Figure 2:Intraoral Preoperative Photographs Showing All Impacted First Permanent Molars
|
On the basis of following diagnosis, a decision of surgical exposure of the impacted teeth was made. Prior to surgical procedure routine blood examinations were carried out which were within normal limit. The operation was performed under local anesthesia in the department of pediatric dentistry. The overlying gingivae on the right side of maxillary and mandibular first permanent molars were excised to expose the crowns of the impacted teeth and left side molars were kept as control (Figure 3, 4). The exposed occlusal surfaces were covered with Coe-pack to prevent occlusal trauma and epithelization. The patient was instructed to take soft and cold diet for 24 hours and an antiseptic mouth rinse was prescribed to maintain oral hygiene.
 | Figure 3 & 4:Intraoral Photographs Showing Surgical Exposure Of Right Maxillary And Mandibular Impacted Teeth
|
 | Figure 4:Intraoral Photographs Showing Surgical Exposure Of Right Maxillary And Mandibular Impacted Teeth
|
Routine check up and radiographs were taken after regular interval to assess the improvement of eruption of the tooth. The right maxillary and mandibular tooth erupted into the oral cavity whereas left side molars failed to erupt (Figure 5, 6).
 | Figure 5 & 6:Impacted Right Maxillary And Mandibular Have Erupted In The Oral Cavity
|
 | Figure 6:Impacted Right Maxillary And Mandibular Have Erupted In The Oral Cavity
|
 | Figure 7:Panoramic Radiograph Showing Soft Tissue Impaction Of All Permanent First Molars.
|
Discussion
The sequential and timely eruption of teeth is critical in overall development of dentition of the child. Failure of eruption of single tooth or a group of teeth is an asymptomatic pathology, which means that it is usually a casual discovery and its diagnosis is made late. When this is so, repercussions on the permanent dentition may be already present. These include: malocclusions, shortening of the facial height, incomplete development of the alveolar process and risk of root resorption of neighboring teeth.
Tooth eruption is a complex process and is divided into five stages: pre eruptive movements, intra-osseous stage, mucosal penetration, preocclusal and post occlusal stages.[11] The eruption time of both primary and permanent teeth have got a specific date and variations of six months on either side of the usual eruption date may be considered normal for a given child. Rasmussen and Kotsaki[12], suggest when the emergence of a tooth is more than 2 standard deviations (SDs) from the mean of established norms for eruption times, it should be considered delayed eruption. Because the age at detection in most reported cases is around 10 years, pediatric dentists are more likely than general practitioners to encounter and diagnose such cases.
The eruption of permanent maxillary and mandibular first molar is observed to be around 6-7 years (Table 1, 2).[13] The dental age of a patient is calculated on the basis of last group of teeth erupted into the oral cavity, root resorption of the respective adjacent primary teeth and root development of the succedaneous permanent teeth.[11] Therefore, in the present case the dental age of the patient is 8 years and all the permanent first molars were impacted for more than two years. The impacted permanent first molar should be diagnosed and treated as early as possible to prevent various complications as discussed earlier. Kaban proposed that when roots have developed more than 50 % the impacted tooth should be exposed for spontaneous eruption.[10] In the present case the root development was almost complete and we didn’t delay the operation after diagnoses.
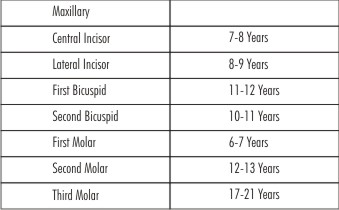 | Table 1:Eruption Date Of Permanent Maxillary Teeth
|
 | Table 2:Eruption Date Of Permanent Mandibular Teeth
|
The present case is very interesting because the prevalence of impaction of permanent first molar is very rare. The management of an impacted tooth often necessitates a complex surgical and orthodontic treatment as indicated by clinical observation of the particular impacted tooth. We opted for surgical exposure (Figure 3, 4) only and periodic follow up for their eruption since the teeth were impacted with soft tissue (Figure 7) and the child was in the growing stage. The surgical objective is to remove the impediment and to assist physiologic eruption by exposing the crown. After exposure of the crown, we usually give surgical pack to prevent epithelial growth over the tooth. In some cases a second surgical exposure may be necessary, if the wound closed with gingival growth following surgical exposure. When the tooth shows no tendency to erupt, then orthodontic traction is indicated.
In this case the thick fibrous band of mucosa over the impacted permanent first molars did not allow the teeth to erupt but at the same time the teeth were not ectopically erupting. Mucosal barrier has been suggested as the etiologic factor in impaction in present case. Disturbance in permanent tooth eruption or impaction may occur after trauma to primary dentition that is related to abnormal change in the connective tissue overlying the tooth germ as suggested by various authors.[14] Impaction is very common among teeth with malformations confined either to root or crown after trauma.[15],[16],[17].
But in this case thick mucosa was formed due to trauma of chronic masticatory forces and fortunately there was no malformation or ectopic eruption of the permanent molars as depicted by OPG (Figure 7). Kramer et al.[18] pointed out that a dental follicle may become thickened when a tooth fails to erupt and that the thickened follicular fibrous tissue is often myxoid. It has been found that when multiple deciduous maxillary incisors have been lost before age of 5, soft tissue over the alveolus becomes hypertrophic and fibrotic, preventing the eruption of permanent central incisors.[10] Whatever the cause for formation of fibrous mucosa, the affected tooth gets impacted.
Refrences
1. Ten Cate AR.Oral histology: development, structure, and function. 3rd ed. St Louis, CV Mosby 1989; 275 -298.
2. Raghoebar GM, Boering G, Vissink A, Stegenga B. Eruption disturbances of permanent molar: a review. J Oral Pathol Med 1991; 20:159-66.
3. Suri L, Gagari E, Vastardis H.Delayed tooth eruption: Pathogenesis, diagnosis, and treatment. A literature review. Am J Orthod Dentofacial Orthop 2004; 126 (4) :432-445
4. Shafer WG, Hine MK, Levy BA:A textbook of oral pathology, Philadelphia, 1974, WB, Saunders.
5. Oliver RG, Richmond S, Hunter B. Submerged permanent molars: four case reports. Br Dent J 1986 ;160(4):128-30
6. Raghoebar GM, Boering G, Jansen HWB, Vissink A. Secondary retention of permanent molar: a histologic study. J Oral Pathol Med 1989; 18 (8): 427-31.
7. Dachi SF, Howell FV. A survey of 3874 routine full mouth radiographs. IL A study of impacted teeth. Oral Surg Oral Med Oral Pathol 1961; 1165-69.
8. Di Salvo NA. Evaluation of unerupted teeth: orthodontic viewpoint. J Am Dent Assoc 1971; 82 (4):829-35.
9. Angle E.H. Behandlung der Okklusionsanomalien der Zähne, Angle´s System, Hermann Meusser Verlag, Berlin 1908.
10. Kaban LB, Needleman HL, Hertzberg J:Idiopathic failure of eruption of permanent molar teeth.Oral Surg Oral Med Oral Pathol 42:155-163, 1976.
11. Proffit WR, Fields HW, Sarver DM. Contemporary orthodontics. 5th ed. St. Louis, Mo: Mosby; 2012.
12. Rasmussen P, Kotsaki A. Inherited retarded eruption in the permanent dentition. J Clin Pediatr Dent 1997; 21:205-11.
13. McDonald RE, Avery DR, Dean JA. Dentistry for the child and adolescent.9th ed. Maryland Heights, Mo: Mosby Elsevier; 2011.
14. DtBlase DD.Mucous membrane and delayed eruption .Dent practit 1971; 21(7):241-50.
15. Andreasen JO, Sundstrom B, Ravn JJ.The effect of traumatic injuries to primary teeth on their permanent successors.1.Aclinical and histologic study of 117 injured permanent teeth. Scand J Dent Res 1971; 79:219-83.
16. Broglia ML.Consideartions su un caso di intrusion traumatic di un dente deciduo causa di ritenzione del correspondente permanente.Minerva Stomatol 1959; 8:811-3.
17. Kamat SS, Kumar GS, Raghunath V, Rekha KP.Permanent maxillary central incisor impaction: report of two cases. Quintessence Int 2003; 34:50-2.
18. Kramer IRH, Pindborg JJ, Shear M: Histological Typing of Odontogenic Tumors, 2nd Ed. Berlin: Springer-Verlag, pp 23, 1992.
|