Introduction
The tongue appears in the embryos of approximately 4weeks as paired lateral lingual swellings (tuberculum impar )and a medial lingual swelling (hypobranchial eminence). These swellings originate from the first pharyngeal arch in the floor of the developing mouth.[1] Incomplete fusion or lack of proper orientation will lead to numerous congenital anomalies of tongue. Clipped tongue or ankyloglossia is a condition in which the midline sheath of tissue attached to the base of the tongue (lingual frenulum) causing restriction of tongue motion.[2]
The incidence of ankyloglossia ranges from 0.002% to 4.8% with a male to female ratio of 3:1.[3] Several studies establish diagnostic criteria based on the length of the lingual frenulum, amplitude of tongue movement, heart-shaped look when the tongue is protruded and thickness of the fibrous membrane. Kotlow’s (1999) classified the ankyloglossia on the basis of free tongue length into four classes as follows: Class I-Mild ankyloglossia 12-16mm, class II- moderate ankyloglossia 8-11mm, class III- ankyloglossia3-,7 mm and class IV- complete ankyloglossia <3mm.[4] In ankyloglossia, due to restricted movements, patients exhibit speech difficulties in pronunciation of certain consonants and diphthongs.[5]
Many descriptions of ankyloglossia are prefaced with statements such as, "Little research has identified the positive relationship between tongue-tie and speech disorders.
The present case report describes the management of clipped tongue associated speech articulation and ice cream licking difficulty through diode laser assisted frenectomy followed by speech therapy by interdisciplinary team approach.
Case Report
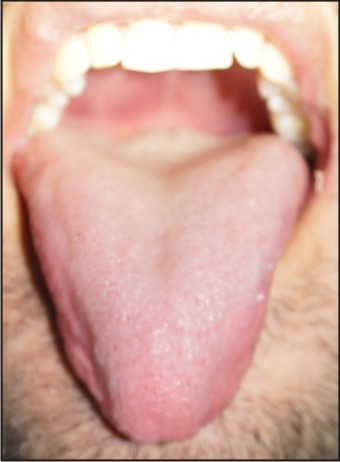
A 24-year-old male patient reported to the Department of Periodontology, Surendera Dental College and Research Institute, Sriganganagar for routine oral prophylaxis. During the conversation with patient, difficulty in speech articulation for consonants like t, d, n, l etc. was observed along with it patient also reported his inability to lick the ice cream cone since childhood. On intraoral examination, partial ankyloglossia of kotlow’s class III [4] was observed with inability to protrude his tongue up to lower lip ,shape of tongue was heart shape with notch on the tip of tongue (Fig 1). Patient was made aware and motivated for the management of same during phase I therapy. Patient was found to be periodontally healthy with bilateral angle’s class I malocclusion (Fig 2) without marginal tissue recession on the lingual aspect of mandibular incisors. The ENT and general physical examination was normal and speech therapist; after evaluating the general and functional test, lingual frenectomy followed speech therapy sessions recommended. Lingual frenectomy by diode laser (Biolase) was advised to the patient and written informed consent was taken.
 | Fig.1: Kotlow's class III ankyloglossia ,with Heart shape tongue and notch on tip of tongue.
 |
 | Fig.2: Bilateral angle's Class 1 malocclusion.
|
After administration of topical anesthesia, few drops of 2% lignocaine hydrochloride and 1:80,000 adrenaline was injected in the frenum. Diode laser 940nm (Biolase) (Fig 3) utilizing 300 micro meter fiberoptic was used in for the frenectomy procedure (Fig 4) at 1.4W in contact and pulse mode utilizing brushing stroke method from coronal to apical direction. The attachment of frenum to the alveolar ridge was also excised to prevent tension on the gingiva .Vitamin-E solution was applied to the wound site (Fig 5). Tongue movement was evaluated immediately after Frenectomy (Fig 6). No suturing and periodontal dressing was applied. Immediate post operative instructions and post operative excersises were advised as per recommendation of speech therapist. Post operative healing at one week was uneventful and satisfactory (Fig 7). Then patient was referred to speech therapist for speech therapy session. One month post operatively reported his ability to lick the ice cream comfortably whereas speech articulation was highly improved after 6 months of speech therapy session (Fig 8).
 | Fig.3: Diode laser 940nm (Biolase).
|
 | Fig.4: Laser assisting Frenectomy.
|
 | Fig.5: Vitamin E solution application.
|
 | Fig.6: Free tongue immediately after procedure.
|
 | Fig.7: Post operative healing at one week.
|
 | 6/5/2015
|
Discussion
Clipped tongue is an uncommon congenital oral developmental anomaly characterized by very short lingual frenulum capable of resulting in variable degree of reduction in tongue mobility, speech difficulty ,chiefly in the pronunciation of certain consonants and diphthongs.[5] In the case reported here, Kotlow’s class III clipped tongue patient presented with mechanical and speech relevance since it cause mechanical-functional modification. Patient reported difficulty in licking the ice cream cone and difficulty in speech articulation in association with altered frenulum attachment which was diagnosed on the basis of kotlow’s classification (1999)[4] as well as on general & functional test evaluation score reported as 5 and 29 respectively[6] by speech therapist which was in accordance with the reports of Lalakea ML and Messner AH 2003.[7] and was advised frenectomy followed by speech therapy.
Diode laser assisted frenectomy was carried out after stripping the 300 micro meter fibreoptic wire tip activation by firing it into a piece of cork at 1.4W in contact pulse mode to facilitate the formation of small amount of carbon at the tip, referred to as “hot tip effect”. It focuses a large amount of energy at contact point and allows accelerate tissue incision. As continuous mode of laser application leads to rapid rise in temperature in the target tissue therefore we preferred pulsed mode which provide time for the tissue to cool down and to prevent collateral tissue damage incident to excessive heat production.[8] Patient hardly reported any discomfort and bleeding during and after the procedure because heat build up leads to the sealing of the small blood vessels through tissue protein denaturation and stimulation of factor VII resulting in reduced post operative edema as well.[9] Lingual frenulum was completely eliminated and immediately after the procedure patient was able to protrude the tongue up to 13-15 mm. Laser’s sterilization of the surgical wound reduces the need for postoperative care and antibiotics. As number of myofibroblasts found after laser treatment are found to be less,[10] this helps in less wound contraction and scarring.Immediate post operative exercises advised;are not intended to increase muscle-strength or to improve speech, but to: 1 develop new muscle movements, particularly those involving tongue-tip elevation and protrusion, inside and outside of the mouth, 2 Increase kinesthetic awareness of the full range of movements the tongue and lips can perform. In this context, kinesthetic awareness refers to knowing where a part of the mouth is, what it is doing, and what it feels like, and 3.Encourage tongue movements related to cleaning the oral cavity, including sweeping the insides of the cheeks, fronts and backs of the teeth, and licking right around both lips; followed by speech therapy for 6 months which resulted in excellent outcome.
Conclusion
Clipped tongue associated speech articulation , cosmetic, social or personnel and functional difficulty will be best diagnosed and managed by interdisciplinary team for the better clinical, morphological and functional outcome as well as to meet patient expectations .
References
1. Langman J.: Head and neck section. Medical Embryology, 4th Ed. Baltimore: The Williams & Wilkins Company.1981; 363-402.
2. Obladen M. Much Ado about Nothing: Two Millenia of Controversy on Tongue-Tie. Neonatology.2010; 97(2):83-9.
3. Lalakea ML,Messner AH. Ankyloglossia: Does it matter? Pediatr Clin North Am 2003 Apr ; 50(2):381-97.
4. Kotlow L. Ankyloglossia (Tonue tie): A diagnosis and treatment quandary. Quintessence Int 1999 Apr; 30(4):259-62.
5. Shafer W, Hine M,Levy BM, Tomich CE. Developmental disturbances of oral and paraoral structures. A Textbook of Oral Pathology, 4th Ed. Philadelphia: Saunders, 2003:2-85.
6. Marchesan,IQ. Lingual frenulum Protocol. Int journal of Orafacial Myology 2012 Nov; 38:89-103.
7. Lalakea ML, Messner AH. Ankyloglossia: The adolescent and adult prospective. Otolaryngol Head Neck Surg 2003 May; 128(5):746-52.
8. Ewart NP. A lingual mucogingival problem associated with ankyloglossia: a case report. N Z Dent J 1990 Jan; 86(383):16-17.
9. Pirnat S. Versatality of an 810 nm diode laser in dentistry: an overview. J Laser Health Acad 2007; 4:19.
10. Zeinoun T, Nammour S, Dourov N, Aftimos G,Laomanen M :Myofibroblasts in healing laser excision wounds. Lasers Surg Med 2001; 28(1):74-9.
|