Introduction:
Clefts of lip and palate are the most common congenital deformities involving the oro-facial region[1] with an estimated incidence of 0.28-3.74 per live births.[2] It is a complex trait caused due to multiple genetic and environmental factors.[3]
The individuals with cleft lip or palate have to deal with numerous problems associated with functions related to the oral and nasal cavities[4] and higher risk of ear infections[5].The oro-nasal communication diminishes the ability to create negative pressure which is necessary for suckling.[6],[7],[8] The feeding process is also complicated by nasal regurgitation of food, excessive air intake that requires frequent burping and choking. Feeding time is significantly longer and fatigues both baby as well as mother.[6], [7]
Most individuals with cleft lip, cleft palate, or both require the coordinated care of providers in many fields of medicine and dentistry (like paediatrician, paediatric surgeon, maxillofacial surgeon, Paediatric dentist, Orthodontist , Prosthodontist) , as well as those in speech pathology, otolaryngology, audiology, genetics, nursing, mental health, and social medicine.
The immediate concern for a newborn with Cleft lip/palate is feeding. In infants with mild defects, feeding may be possible with some modification in mother and child position so as to obdurate the defect with mothers breast. But with most infants with Cleft palate, breast feeding may not be possible because of inability to create negative pressure necessary for suction. These infants require some form of obturator for defect to be able to feed properly. A feeding plate is an appliance which obturates the cleft and restores the separation between oral and nasal cavities. It creates a rigid platform towards which the baby can press the nipple and extract the milk[9]. It facilitates feeding[4],[7], reduces nasal regurgitation,[6],[7] reduces the incidence of choking and shortens the length of time required for feeding. It also helps to position the tongue in correct position to perform its functional role in the development of jaws, and contributes to speech development. Feeding plate restores the basic functions of mastication, deglutition and speech production until the cleft lip and/or palate can be surgically corrected.
Case Report
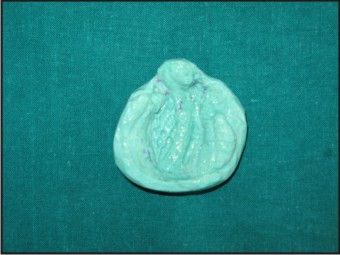
A four day old infant was brought to us as the infant was having difficulty in feeding due to the presence of bilateral cleft lip and palate. A thorough examination was done for the infant to evaluate the extent of the defect. (Fig.1) The History and examination revealed that the patient had Veau’s Class IV Bilateral cleft lip and palate[10]. No other extra oral or intraoral deformity was detected during the examination. As the immediate concern at this time was feeding and nutrition of the infant, it was decided to fabricate a feeding appliance for the infant, to enable him to be fed until further course of treatment was decided by the team. The parents were explained about the procedure and the benefits of the same.
 | Fig. 1 - Preoperative View Showing Bilateral Cleft Lip And Palate
 |
An Impression of the oral cavity was made with polyvinylsiloxane impression material putty consisitency (Aquasil soft Putty, Dentsply DeTrey, GmbH) (Fig. 2). The child’s face was kept towards the ground during the impression procedure so as to prevent any aspiration of the impression material. The child was continuously crying during the procedure which has an added advantage of ensuring a patent airway during the procedure.
The impression was poured with Dental Stone (type III) to obtain a cast of the oral cavity. The feeding Obturator was fabricated using autopolymerising acrylic resin. Two 18G Orthodontic wires were attached to the plate which extended out of the mouth. At the ends of the orthodontic wires, some acrylic resin was applied to prevent any injury to the child or parents due to the sharp ends of the wires. These wires are attached to prevent accidental ingestion or aspiration of the appliance.
The appliance was finished and polished and tried in the childs mouth. The appliance was delivered and the parents were explained about the use and the care of the appliance. The parents were advised to follow regular check-up visits every three months so that the growth can be monitored.The parents were very happy with the apploiance and the child was able to feed well with the obturator in place.
As the child grows, the appliance no longer fits properly, so at that time it may need to be remade.
After 9 Months, it was found that the appliance has become ill-fitting due to the growth of the child, thus a new Obturator was fabricated at that time. Similar procedure was followed at this time also, and the appliance delivered with care instructions to the parents.
 | Fig. 2 - Impression Made With Polyvinylsiloxane Impression Material
|
 | Fig. 3 - Cast Poured With Dental Stone
|
 | Fig. 4 - Obturator Appliance With Wire Extensions
|
 | Fig. 5 - Obturator Fitting Well In The Infants Mouth.
|
Discussion
The child born with required special attention. The treatment of Cleft Lip and palate required comprehensive planning by a team of specialists to ensure normal physical, mental and psychological growth and well being of the patient. During the early period of the child’s life, the health of the child can be severely affected due to the cleft because of inadequate Nutrition to the child. The child usually takes about one-third to three fourth of the amount required for proper nutrition. This is due to the increased effort needed to suckwhich causes early fatigue in these infants, and the greatly increased and prolonged muscular action ted to widen the palatal deformity. The fatigue produced by the prolonged feeding and the necessary extra muscular activity, coupled with insufficient caloric intake can lead to severe malnutrition in these infants.[11]
The fabrication of a feeding appliance for the new born baby with cleft palate can be highly beneficial in ensuring proper nutrition and prevention of infection.[12],[13],[14]. It helps in creating a rigid platform against which the infant can press the nipple and suck effectively, reduces nasal regurgitation, reduces the time and effort required for feeding, helps to keep the tongue away form the cleft to allow unhindered growth of the palatal shelves and provides much needed reassurance to the parents.
Conclusion
Management of new born babies with cleft lip and palate is usually challenging. A team approach is usually required for correct treatment planning. Until surgical correction of the defect is carried out, an accurately fabricated feeding appliance plays an important role for the child to be fed properly and ensure adequate nutrition and growth of the child.
References:
1. Profit WR, Fields HW, Sarver DM. Contemporary Orthodontics.4th ed india: Mosby (an imprint of Elsevier) 007,p. 287-88.
2. McDonald R, Avery D, Dean J. Dentistry for the Child and the Adolescent. 8 th Ed St. Louis, Missouri: Mosby; 2004
3. Murray, JC. Gene/environment causes of cleft lip and/or palate. Clin. Genet. 2002. 61:248-256
4. Osuji OO. Preparation of feeding obturators for infants with cleft lip and palate. J Clin Pediatr Dent 1995;19: 211-14.
5. Sheahan P, Miller I, Sheahan JN, Earley MJ, Blayney AW. Incidence and outcome of middle ear disease in cleft lip and/or cleft palate. International journal of pediatric otorhinolaryngology. 2003;67(7):785-93.
6. Jones JE, Henderson L, Avery DR. Use of a feeding obturator for infants with severe cleft lip and palate. Spec Care Dentist 1982;2:116-20.
7. Choi BH, Kleinheinz J, Joos U, Komposch G. Sucking efficiency of early orthopaedic plate and teats in infants with cleft lip and palate. Int J Oral Maxillofac Surg 1991;20: 167-69.
8. Shprintzen RJ. The implications of the diagnosis of Robin sequence. Cleft Palate Craniofac J 1992;29:205-09.
9. Samant A. A one-visit obturator technique for infants with cleft palate. J Oral Maxillofac Surg 1989;47:539-40.
10. Kernahan DA, Stark RB. A new classification system for cleft lip and cleft palate.Plastic reconstr. Surg 1958,;22(5);441
11. John A Foote. Malnutrition in infants with cleft palate: with a description of a new external obturator. Am J Dis child. 1925; 30(3):343-346.
12. Turner L, Jacobsen C, Humenczuk M, Singhal VK, Moore D, Bell H. The effects of lactation education and a prosthetic obturator appliance on feeding efficiency in infants with cleft lip and palate. Cleft Palate Craniofac J 2001;38:519-24.
13. M. Rathee, A. Hooda, A.K. Tamarkar, S.P.S. Yadav: Role of Feeding Plate in Cleft Palate: Case Report and Review of Literature. The Internet Journal of Otorhinolaryngology. 2010 Volume 12 Number 1.
14. Oliver HT. Construction of orthodontic appliances for the treatment of newborn infants with clefts of the lip and palate. Am J Orthod 1969;56:468-73
|